
Polyphenol Power. Keep your Brain Young with Antioxidants.
—–
By Patrick Holford
Life is a balancing act between making energy by combusting glucose or ketones with oxygen, which generates ‘oxidant’ exhaust fumes and dealing with these ‘oxidant fumes’ which harm the body.
Skin goes crinkly, age spots develop all due to oxidation. That’s what makes apples go brown, leaves change colour and iron rust. In the end, we lose, which is why all oxygen-based life forms have a finite life – and why your brain and body do inevitably age.
However, you can not only add years to your life, but also life to your years by improving your intake of antioxidants and polyphenols found in whole foods, fruits, vegetables and herbs and spices. A study in Finland and Sweden compared those with a ‘healthy’ versus ‘unhealthy’ diet in mid-life for future risk of developing Alzheimer’s disease and dementia 14 years later (1). Those who ate the healthiest diet had an 86-90% decreased risk of developing dementia and a 90-92% decreased risk of developing Alzheimer’s disease. Some of the benefit comes from low sugar diets, high in omega-3 and B vitamins and some from foods high in antioxidants and polyphenols which we will focus on here.
Your intake of these versus your intake and generation of oxidants, for example from smoking and pollution, is a major determinant of brain health. An illustration of this is the fact that both smoking and pollution exposure increase risk of cognitive decline and dementia, while vitamin C, which is the antioxidant par excellence, reduces risk.
(This is why we have developed our brand new Glutathione at home blood test – the first of its kind where you can accurately test your antioxidant status from home and support our further research into this important area. You can find out more and pre order the test here )
—
Oxidants vs antioxidants – moving the balance in your favour
Smoking increases risk of Alzheimer’s just as much as having low B vitamin or omega-3 status, according to the US National Institute of health’s analysis (2). Smoking is something a person can easily change. Air pollution, for many, is not. It is measured in the amount of particulate matter (PMs) and people living in polluted cities are exposed to more. A study of women living in cities in the US found that those exceeding the ‘safe’ levels (greater than 12 μg/m3) had ‘increased the risks for global cognitive decline and all-cause dementia respectively by 81% and 92%’. (3)
While you may not be able to change where you live, can you mitigate the effects of pollution? The answer is yes – in two ways. Firstly, by increasing your intake of antioxidants and also by improving your B vitamin status since the body detoxifies many toxins, including toxic metals from lead to mercury, by methylation. A similar study to the one above found that residing in locations with PM exposure above the safe level was associated with a higher risk of dementia but only among people with lower intakes of the homocysteine lowering B vitamins (B6, folate, b12) (4). ‘Vitamin C in the diet or taken as supplements might help’ concludes another.(5)
Smokers need at least twice as much vitamin C as non-smokers just to have basic vitamin C levels in their blood (serum). Men do worse than women. Even with an intake of 200mg a day they do not achieve this basic blood level, which is already two to three times the recommended dietary intake and what you’d get in four oranges (6). It is certainly wise for any smoker to supplement vitamin C, perhaps adding 50mg per cigarette – 500mg if you smoke 10 a day, although there is a good case for everyone to supplement 1,000mg a day, or 2,000mg a day if over 50.
Nature always provides a solution to help us with our evolution. It seems obvious to me we need vitamin C to combat excessive pollution.
Vitamin C is a keystone nutrient as far as swinging the antioxidant equation in your favour. It’s made in all living things, from animals to plants, including yeasts and funghi. It’s probably been the essential ‘exhaust recycler’ of all oxygen-based lifeforms. Production is even activated when oxidants are sensed. Animals also make more when stressed or exposed to viruses. Us humans, and all other primates, are one of very few species who can’t make it. The first non-vitamin C making animal to be discovered was the guinea pig. That’s how it became the ‘guinea pig’ for research since, like us, it’s dependent every second of every day on vitamin C from diet. Bats, a few birds and the teleost family of fish have also lost the ability to make vitamin C.
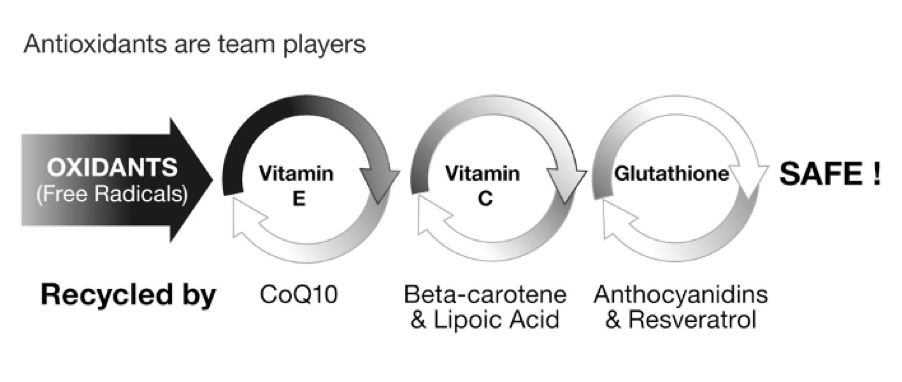
You’ll see in this figure below and from watching the film above, that vitamin C disarms water-based oxidants, such as smoke, and vitamin E disarms fat-based oxidants such as burnt fat. Then, there are other key antioxidant team players that help to neutralise the reactive oxidants that damage our brain and body.
—
—
Your best bet is probably to both eat a diet with a broad spectrum of antioxidants and also supplement them. The older you are the more you are likely to need. Key antioxidants are:
- Vitamin A, C and E – associated with reducing Alzheimer’s risk
- Lipoic acid (7) – protects the memory-friendly neurotransmitter acetylcholine and dampens down brain oxidation and inflammation)
- Glutathione (8) or N-acetyl Cysteine (NAC)(9) – protects the brain and improves methylation thus having potential in dementia prevention.
- Co-enzyme Q10 – protects the mitochondria in the brain from oxidative stress (10)
- Resveratrol – resveratrol has antioxidant, anti-inflammatory and neuroprotective properties and prevents hippocampal brain damage. (11)
It doesn’t really make a lot of sense to supplement one without the others.
Individually, their impact on your brain health may be less than when combined. A study of 4,740 Cache County Utah elderly residents found that those supplementing both vitamin E and C cut their risk of developing Alzheimer’s by two thirds. Taking either cut risk by a quarter (12). A recent meta-analysis of all studies on factors that could prevent Alzheimer’s by one of our Scientific Advisory Board members – Professor Jin Tai Yu of Fudan University in Shanghai, China – shows that ‘either a high vitamin E or C intake showed a trend of attenuating risk by about 26%’ making these nutrients ‘grade 1’ top level prevention risk factors (13).
All those listed above – vitamin C, E, glutathione and N-acetyl cysteine, Coenzyme Q10 and resveratrol – work together and are often found in combined antioxidant supplement formulas. There are many other team player ‘cousins’ from B vitamins to minerals such as magnesium, selenium and zinc found respectively in greens, seafood, nuts and seeds.
There are two ways to increase your intake – through food and from supplements. Foods can be measured for their ‘Total Antioxidant Capacity’ or TAC for short. It’s worked out from an equation involving eight key antioxidants from vitamin A, carotenes (think carrots), lycopenes (rich in tomatoes), lutein and zeaxanthine (rich in green vegetables), vitamin E (is nuts and seeds), but most of all vitamin C (rich in berries, broccoli, peppers and other vegetables).
The higher the TAC score of your diet the lower is your risk of cognitive and memory decline. This was the finding of a recent study of 2,716 people over age 60. The researchers measured the TAC score from their diet, splitting them into the highest to lowest quarter of TAC score, and compared this to a number of memory tests. Those in the highest quarter, eating the most antioxidant-rich foods had half the risk of decreasing memory. The higher the TAC score the better their memory function was. (14)
—
Go Rainbow, ‘Mediterranean’ and eat five or more servings of fruit and vegetables a day
So, what do you need to eat and drink to preserve your memory and protect your brain?
Basically, eat a Mediterranean style ‘rainbow coloured’ diet. A Mediterranean diet has more fish, less meat and dairy, more olive oil, fruit and vegetables including tomatoes, legumes (beans and lentils) and whole grain cereals than a standard Western diet. It also includes small quantities of red wine. There are variations of this kind of diet, called the MIND diet and the DASH diet, but the core components are the same and as researchers drill down, we are learning what to eat and drink to keep your mind sharp and brain young, and how much.
The trick is to really start thinking of the colours you’re eating and gravitate for the strong colours.
Mustard and turmeric, for example, are strong yellows. Dijon mustard is great – no sugar. But if you like good old-fashioned English mustard go for it. Have a teaspoon every other day.
Add turmeric to almost any steam-fry, curry or soup.
Bright oranges include butternut squash, sweet potato, carrots – but do buy organic. Translucent mass produced carrots are tasteless and have a higher water content, ie less actual carrot.
Tomatoes are particularly good for you. Buy seeded, not seedless watermelons. Blend the flesh in a blender, perhaps with some ice. The black husk of the seeds drops to the bottom. The flesh of the seeds, full of essential nutrients, becomes part of this mouth-wateringly refreshing drink. Great for detox. Strawberries are a low GL fruit. Red, yellow, green and orange peppers are all rich in vitamin C.
Anything purple, magenta or blue is brilliant for you. From beetroots (eat them raw, grated into salads) to blueberries, blackberries and raspberries. Strawberries are particularly good. According to a study, part of the Rush Memory and Aging Project at Rush University, Chicago, having a higher intake cut Alzheimer’s risk by a quarter. They are high in both vitamin C and flavanoids, a high level of which were also confirmed to cut risk by a third. (15)
Strong greens are always beneficial – from spinach, kale, Brussels sprouts, broccoli, tender stem, watercress, rocket, asparagus, artichoke, green beans, peas, kohlrabi, and cauliflower (although not green).
Polyphenol power
Some of these foods are particularly rich in ‘polyphenols’ a group of health promoting molecules which also includes flavonoids, sometimes called flavanols. Blue foods such as blueberries contain another polyphenol called anthocyanins. Tea, the cacao in chocolate, red wine, red onions, olives and all the blueish berries are rich sources of polyphenols. Many of these polyphenol rich foods act as antioxidants but they do much more than this. They improve circulation in the brain, lower blood pressure and dampen down inflammation which lies behind many conditions from depression to dementia. Once again, the principle of what’s good for the heart is good for the brain.
One of the first important studies was carried out in Norway more than a decade ago by Eha Nurk and Helga Refsum and colleagues in Norway. (16)(17) They found that:
Tea – the more you drink the better. The tea benefit has been confirmed more recently in a study in Singapore, with green tea being marginally better than black tea.(18) However, this benefit was not found in a UK Biobank study, which reported tea and coffee drinking to be associated with worsening cognition compared to abstainers. (19)
Chocolate – peaks at 10g, or about 3 pieces – and let’s say dark, 70 or more percent, thus with less sugar, is likely to be better, as sugar is a strong indicator of cognitive decline. If a chocolate is 80% cacao that means almost 20% will be sugar. More recent studies giving cocoa, a rich source of flavanols, have shown improved cognition, possibly by improving circulation.(20) This has been confirmed in a big COSMOS trial involving over 20,000 people given a cacao extract supplement rich in flavanols versus a placebo for five years. (21) The reduction in cardiovascular risk was even greater than that of a Mediterranean diet.
Wine – consumption reduces risk of cognitive decline up to an intake of 125ml a day, which is a small glass. A thorough study in the British Medical Journal in 2018, which had followed over 9,000 people over 23 years, showed that both abstinence and drinking more than 14 units of alcohol a week, which is equivalent to a medium glass of wine (2.3 units) every day, also increases risk (22). This is consistent with studies showing that a small glass of wine a day decreases risk of cardiovascular disease. Red wine, high in resveratrol is likely to be most beneficial.
All the above are rich in a polyphenol called epicatechin. Jeremy Spencer, an advisor to Food for the Brain, who is Professor of Nutritional Biochemistry and Medicine at the University of Reading, where he specialises in studying the health benefits of polyphenols and other compounds in plants, has shown that these polyphenol rich plants improve blood brain flow in specific regions of the brain that improve attention, decision-making, impulse control and emotion, thus improving overall ‘executive’ function (23). What’s more, the level of flavanols you have in your bloodstream predicts your memory. The biggest impact of increasing flavanols, was seen in the COSMOS study, in those in the lowest third for dietary intake specifically seeing improvement in aspects of memory that link to the hippocampus, that central area of the brain that degenerates in Alzheimer’s (24).
—
The Best Fruit and Veg to Eat for Your Brain
Which vegetables pack the biggest punch as far as polyphenols and antioxidants are concerned and are also lower in sugar or low GL?
Taking all these factors into account – the GL, antioxidants and polyphenols these are the dozen best rated fruit and veg. But do not think of this list as finite as more and more research reveals the amazing healing power of nature’s fruits and vegetables.
—
| Lowest GL | Antioxidant | Polyphenol | |
| Cacao | *** | *** | *** |
| Olives | *** | *** | *** |
| Blueberries | *** | *** | *** |
| Kale | *** | ** | *** |
| Blackcurrants | ** | *** | ** |
| Strawberries | *** | *** | ** |
| Broccoli | *** | ** | *** |
| Artichokes | *** | ** | *** |
| Cabbage (red) | *** | *** | ** |
| Asparagus | *** | ** | ** |
| Onions (red) | ** | * | *** |
| Avocado | *** | ** | ** |
| Apples | ** | ** | ** |
| Beetroot | * | * | *** |
| Cherries | ** | ** | ** |
—
The optimal intake for brain protection is 5 to 6 servings of fruit and veg a day.
Half a plate of a main meal counts as two. A handful of berries would count as one. So, if half your plate for two main meals is vegetables, and you had some berries with your breakfast and another piece of fresh fruit or perhaps some broccoli heads or tenderstem or carrots dipped in hummus as a snack, or half an avocado with some high polyphenol olive oil, you’ve achieved six servings.
The first step is to eat ‘whole’ foods, and especially fresh plant foods with an emphasis on those listed above that are more likely to be high in antioxidants and polyphenols. (Also see the Alzheimers Prevention Diet.) There are some nutrients such as vitamin C for which just eating whole foods doesn’t guarantee you are achieving an optimal intake and are well worth supplementing.
My advice is to supplement 500mg to 1,000mg of vitamin C twice a day and also take an antioxidant formula or antioxidant rich multivitamin containing vitamins A, C, E, lipoic acid, glutathione or NAC, resveratrol and CoQ10.

Summary
- Support our research and be one of the first to test your antioxidant status with the Glutathione Index test. Pre order here
- Take the FREE Cognitive Function Test here.
- Want to get recipes to help you increase your antioxidant intake? Pre order the Upgrade Your Brain Cook App here
—
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices.
Please support our research by becoming a Friend of Food for the Brain.

References
- Eskelinen MH, Ngandu T, Tuomilehto J, Soininen H, Kivipelto M. Midlife healthy-diet index and late-life dementia and Alzheimer’s disease. Dement Geriatr Cogn Dis Extra. 2011 Jan;1(1):103-12. doi: 10.1159/000327518. Epub 2011 Apr 27. PMID: 22163237; PMCID: PMC3199886.
- Beydoun MA, Beydoun HA, Gamaldo AA, Teel A, Zonderman AB, Wang Y. Epidemiologic studies of modifiable factors associated with cognition and dementia: systematic review and meta-analysis. BMC Public Health. 2014 Jun 24;14:643. doi: 10.1186/1471-2458-14-643. PMID: 24962204; PMCID: PMC4099157.
- Cacciottolo M, Wang X, Driscoll I, Woodward N, Saffari A, Reyes J, Serre ML, Vizuete W, Sioutas C, Morgan TE, Gatz M, Chui HC, Shumaker SA, Resnick SM, Espeland MA, Finch CE, Chen JC. Particulate air pollutants, APOE alleles and their contributions to cognitive impairment in older women and to amyloidogenesis in experimental models. Transl Psychiatry. 2017 Jan 31;7(1):e1022. doi: 10.1038/tp.2016.280. PMID: 28140404; PMCID: PMC5299391.
- Chen C, Whitsel EA, Espeland MA, Snetselaar L, Hayden KM, Lamichhane AP, Serre ML, Vizuete W, Kaufman JD, Wang X, Chui HC, D’Alton ME, Chen JC, Kahe K. B vitamin intakes modify the association between particulate air pollutants and incidence of all-cause dementia: Findings from the Women’s Health Initiative Memory Study. Alzheimers Dement. 2022 Nov;18(11):2188-2198. doi: 10.1002/alz.12515. Epub 2022 Feb 1. PMID: 35103387; PMCID: PMC9339592.
- Yu JT, Xu W, Tan CC, Andrieu S, Suckling J, Evangelou E, Pan A, Zhang C, Jia J, Feng L, Kua EH, Wang YJ, Wang HF, Tan MS, Li JQ, Hou XH, Wan Y, Tan L, Mok V, Tan L, Dong Q, Touchon J, Gauthier S, Aisen PS, Vellas B. Evidence-based prevention of Alzheimer’s disease: systematic review and meta-analysis of 243 observational prospective studies and 153 randomised controlled trials. J Neurol Neurosurg Psychiatry. 2020 Nov;91(11):1201-1209. doi: 10.1136/jnnp-2019-321913. Epub 2020 Jul 20. PMID: 32690803; PMCID: PMC7569385.
- Carr AC, Lykkesfeldt J. Factors Affecting the Vitamin C Dose-Concentration Relationship: Implications for Global Vitamin C Dietary Recommendations. Nutrients. 2023 Mar 29;15(7):1657. doi: 10.3390/nu15071657. PMID: 37049497; PMCID: PMC10096887.
- A. Maczurek, et al., ‘Lipoic acid as an anti-inflammatory and neuroprotective treatment for Alzheimer’s disease’, Advance Drug Delivery Review, 2008;60(13-14):1463-70
- Pocernich CB, Butterfield DA. Elevation of glutathione as a therapeutic strategy in Alzheimer disease. Biochim Biophys Acta. 2012 May;1822(5):625-30. doi: 10.1016/j.bbadis.2011.10.003. Epub 2011 Oct 12. PMID: 22015471; PMCID: PMC3277671.
- Hara Y, McKeehan N, Dacks PA, Fillit HM. Evaluation of the Neuroprotective Potential of N-Acetylcysteine for Prevention and Treatment of Cognitive Aging and Dementia. J Prev Alzheimers Dis. 2017;4(3):201-206. doi: 10.14283/jpad.2017.22. PMID: 29182711.
- Yang X, Zhang Y, Xu H, Luo X, Yu J, Liu J, Chang RC. Neuroprotection of Coenzyme Q10 in Neurodegenerative Diseases. Curr Top Med Chem. 2016;16(8):858-66. doi: 10.2174/1568026615666150827095252. PMID: 26311425.
- Gomes BAQ, Silva JPB, Romeiro CFR, Dos Santos SM, Rodrigues CA, Gonçalves PR, Sakai JT, Mendes PFS, Varela ELP, Monteiro MC. Neuroprotective Mechanisms of Resveratrol in Alzheimer’s Disease: Role of SIRT1. Oxid Med Cell Longev. 2018 Oct 30;2018:8152373. doi: 10.1155/2018/8152373. PMID: 30510627; PMCID: PMC6232815.
- Basambombo LL, Carmichael PH, Côté S, Laurin D. Use of Vitamin E and C Supplements for the Prevention of Cognitive Decline. Ann Pharmacother. 2017 Feb;51(2):118-124. doi: 10.1177/1060028016673072. Epub 2016 Oct 5. PMID: 27708183.
- See reference 5.
- Peng, M., Liu, Y., Jia, X. et al. Dietary Total Antioxidant Capacity and Cognitive Function in Older Adults in the United States: The NHANES 2011–2014. J Nutr Health Aging 27, 479–486 (2023). https://doi.org/10.1007/s12603-023-1934-9
- Agarwal P, Holland TM, Wang Y, Bennett DA, Morris MC. Association of Strawberries and Anthocyanidin Intake with Alzheimer’s Dementia Risk. Nutrients. 2019 Dec 14;11(12):3060. doi: 10.3390/nu11123060. PMID: 31847371; PMCID: PMC6950087.
- Nurk E, Refsum H, Drevon CA, Tell GS, Nygaard HA, Engedal K, Smith AD. Intake of flavonoid-rich wine, tea, and chocolate by elderly men and women is associated with better cognitive test performance. J Nutr. 2009 Jan;139(1):120-7. doi: 10.3945/jn.108.095182. Epub 2008 Dec 3. PMID: 19056649.
- Nurk E, Refsum H, Drevon CA, Tell GS, Nygaard HA, Engedal K, Smith AD. Cognitive performance among the elderly in relation to the intake of plant foods. The Hordaland Health Study. Br J Nutr. 2010 Oct;104(8):1190-201. doi: 10.1017/S0007114510001807. Epub 2010 Jun 16. PMID: 20550741.
- Feng L, Chong MS, Lim WS, Lee TS, Kua EH, Ng TP. Tea for Alzheimer Prevention. J Prev Alzheimers Dis. 2015;2(2):136-141. doi: 10.14283/jpad.2015.57. PMID: 29231231.
- Cornelis MC, Weintraub S, Morris MC. Caffeinated Coffee and Tea Consumption, Genetic Variation and Cognitive Function in the UK Biobank. J Nutr. 2020 Aug 1;150(8):2164-2174. doi: 10.1093/jn/nxaa147. PMID: 32495843; PMCID: PMC7398783.
- Lamport DJ, Pal D, Moutsiana C, Field DT, Williams CM, Spencer JP, Butler LT. The effect of flavanol-rich cocoa on cerebral perfusion in healthy older adults during conscious resting state: a placebo controlled, crossover, acute trial. Psychopharmacology (Berl). 2015 Sep;232(17):3227-34. doi: 10.1007/s00213-015-3972-4. Epub 2015 Jun 7. PMID: 26047963; PMCID: PMC4534492.
- Sesso HD, Manson JE, Aragaki AK, Rist PM, Johnson LG, Friedenberg G, Copeland T, Clar A, Mora S, Moorthy MV, Sarkissian A, Carrick WR, Anderson GL; COSMOS Research Group. Effect of cocoa flavanol supplementation for the prevention of cardiovascular disease events: the COcoa Supplement and Multivitamin Outcomes Study (COSMOS) randomized clinical trial. Am J Clin Nutr. 2022 Jun 7;115(6):1490-1500. doi: 10.1093/ajcn/nqac055. PMID: 35294962; PMCID: PMC9170467.
- Sabia S, Fayosse A, Dumurgier J, Dugravot A, Akbaraly T, Britton A, Kivimäki M, Singh-Manoux A. Alcohol consumption and risk of dementia: 23 year follow-up of Whitehall II cohort study. BMJ. 2018 Aug 1;362:k2927. doi: 10.1136/bmj.k2927. PMID: 30068508; PMCID: PMC6066998.
- See Professor Peremy Spencer’s presentation at the Alzheimer’s is preventable masterclass (2022); also see Spencer JP. The impact of fruit flavonoids on memory and cognition. Br J Nutr. 2010 Oct;104 Suppl 3:S40-7. doi: 10.1017/S0007114510003934. PMID: 20955649.
- Brickman AM, Yeung LK, Alschuler DM, Ottaviani JI, Kuhnle GGC, Sloan RP, Luttmann-Gibson H, Copeland T, Schroeter H, Sesso HD, Manson JE, Wall M, Small SA. Dietary flavanols restore hippocampal-dependent memory in older adults with lower diet quality and lower habitual flavanol consumption. Proc Natl Acad Sci U S A. 2023 Jun 6;120(23):e2216932120. doi: 10.1073/pnas.2216932120. Epub 2023 May 30. PMID: 37252983; PMCID: PMC10265949.








