



The GL of Your Diet Determines Your Future Dementia Risk
The GL of Your Diet Determines Your Future Dementia Risk
by Patrick Holford

Why Blood Sugar Exposure Matters More Than Sugar Itself
From that simple fact comes a widespread assumption: that sugar fuels the brain and therefore more sugar must mean more mental energy.
In reality, the opposite appears to be true.
A large new study shows that the glycaemic load (GL) of your diet, which reflects how much glucose you expose your bloodstream to over time, is strongly linked to your future risk of dementia. The higher the glycaemic load, the higher the risk.
How Much Sugar Your Body Really Needs
As petrol is for your car, glucose is the primary fuel for your body. Glucose is the main fuel used by all cells.
There is also another fuel, ketones, much like cars can also run on electricity. We too are metabolic hybrids.
Now here is an astonishing fact. Your body contains around 100,000 kilometres of blood vessels. Your brain alone has around 1,000 kilometres of them. These vessels supply energy to around 30 trillion cells, each containing roughly 1,000 mitochondria, the tiny energy factories that power life.
And yet, across this entire system, there only needs to be around 4 grams of glucose in your bloodstream at any one time. That is one teaspoonful. That is all that is required for every cell in your brain and body to have energy at that moment.²
GL is a measure of how much glucose enters your bloodstream after eating or drinking a food. If there is not much glucose in the food, and you use it quickly, perhaps by moving or exercising, blood sugar levels stabilise rapidly.
The glycaemic load of a food depends on two things:
• the quality of the carbohydrate
• the quantity eaten
Quality refers to how fast glucose is released, known as the glycaemic index (GI). Fibre and protein slow this release. This is why white rice has a higher GI than brown rice, which contains fibre. Eat rice with fish, beans or meat, and the protein slows the release further.
GL also depends on portion size. A small serving of brown rice with fish is low GL. A large serving of white rice, even with fish, is high GL.
When Glucose Becomes Toxic to the Brain
What happens if you consume far more glucose than the body needs?
A can of sugary fizzy drink contains around 35 grams of sugar. That is roughly nine times more glucose than the total amount normally circulating in your bloodstream.
This excess is toxic. It damages blood vessels and the tissues they supply. Diabetes is diagnosed precisely because excess sugar damages the kidneys, eyes and nerves. The brain is no exception.
“The brain needs more energy than any other organ, so it contains the most mitochondria. Sugar damages mitochondria,” says Professor Robert Lustig, Professor of Neuroendocrinology at the University of California, San Francisco. If you have read Upgrade Your Brain or Alzheimer’s: Prevention is the Cure, you will already know that high sugar intake, sugary drinks and ultra processed foods increase dementia risk, worsen memory even in young people, and are associated with measurable shrinkage of brain regions involved in memory in teenagers.
Are You Eating Too Much Hidden Sugar?
The simplest way to assess your long term blood sugar exposure is to measure HbA1c.
HbA1c literally means sugar damaged red blood cells. If more than 6.5% of your red blood cells are sugar damaged, you are diagnosed with diabetes. Above 6% indicates pre diabetes. Even levels above 5.4% in teenagers predict brain shrinkage.
For optimal health you want to be below 5.4%, and ideally below 5%.
HbA1c is such a strong indicator of blood sugar resilience that it is included in Food for the Brain’s 5-in-1 DRIfT home blood test kit.
Balancing Blood Sugar with a Low Glycaemic Load Diet
Let us start with something simple.
An orange contains sugar, but also fibre and micronutrients. The fibre slows sugar release, mainly fructose, which takes time to convert to glucose, while feeding beneficial gut bacteria.
A glass of orange juice, however, contains the sugar of around three oranges, without the fibre. Three times the sugar, with no brakes. Eat your fruit. Do not drink it.
When you eat sugar or starches such as rice, digestive enzymes rapidly break them down into glucose. Protein, by contrast, takes several hours to digest into amino acids. This slows carbohydrate digestion further down the digestive tract.
This leads to a simple rule: eat carbohydrates with protein.
Brown rice releases glucose more slowly than white rice. Add beans, fish or meat, and the release slows further.
From this we can extract three practical rules:
• Eat fruit. Do not drink it
• Always eat carbohydrate with protein
• Make fibre the primary ingredient of every meal
What a Low GL Meal Actually Looks Like
Compare these two breakfasts:
Cornflakes with a banana or Oats with chia seeds and berries
Cornflakes are fast releasing sugar. Oats are slow releasing. A banana raises blood sugar more than two bowls of berries.
Chia seeds, rich in soluble fibre, dramatically slow sugar release. A portion of oats with chia and berries is around 10 GL. Cornflakes and a banana can reach 30 GL.
You want meals around 10 GL and snacks around 5 GL. Three meals and two snacks equals around 40 GL per day.
Eat 40 GL per day to lose weight. Around 60 GL to maintain it.
Eat little and often, and start the day with a low GL breakfast.
A friend of mine, Dr David Unwin, who is a leading diabetes doctor, converted our low GL calculations into ‘teaspoons of sugar equivalent’ to give a visual idea to his diabetic and overweight patients of how sugar is hidden in common foods. See the table below.
| Food | GI | Serving size | GL | Teaspoons of sugar |
| Cereals | ||||
| Coco Pops | 77 | 30g | 20 | 7.3 |
| Cornflakes | 93 | 30g | 22 | 8.4 |
| Mini Wheats | 59 | 30g | 13 | 4.4 |
| Shredded Wheat | 67 | 30g | 14 | 4.8 |
| Special K | 54 | 30g | 12 | 4.0 |
| Bran Flakes | 74 | 30g | 13 | 4.8 |
| Porridge | 63 | 150ml | 6 | 2.2 |
| Bread | ||||
| White | 71 | 30g | 10 | 3.7 |
| Brown | 74 | 30g | 9 | 3.3 |
| Rye (69% wholegrain rye flour) | 78 | 30g | 11 | 4.0 |
| Wholegrain barley (50% barley) | 85 | 30g | 15 | 5.5 |
| Wholemeal (stoneground flour) | 59 | 30g | 7 | 2.6 |
| Pitta (wholemeal) | 56 | 30g | 8 | 2.9 |
| Rough oatcake | 35 | 10.4g | 2 | 0.7 |
| Fruit | ||||
| Banana | 62 | 120g | 16 | 5.9 |
| Grapes (black) | 59 | 120g | 11 | 4.0 |
| Apple (Golden Delicious) | 39 | 120g | 6 | 2.2 |
| Watermelon | 80 | 120g | 5 | 1.8 |
| Nectarines | 43 | 120g | 4 | 1.5 |
| Apricots | 34 | 120g | 3 | 1.1 |
| Strawberries | 40 | 120g | 1 | 0.4 |
Adapted, with permission, from David Unwin’s charts in the Journal of Insulin Resistance (2016)
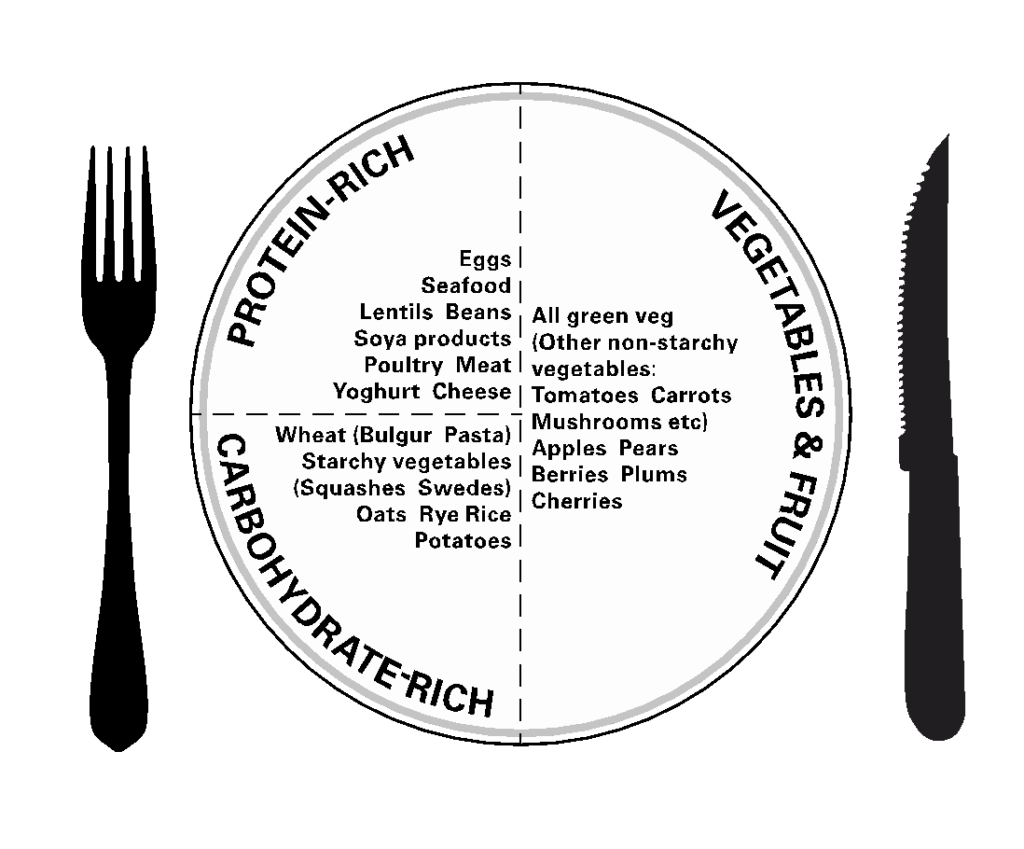
The Balance of Your Plate
Half your plate should be vegetables and fruit. A quarter should be protein. A quarter carbohydrate.
Vegetables supply antioxidants that neutralise the exhaust fumes produced when mitochondria burn fuel. This becomes more important as we age and mitochondrial efficiency declines.
Protein slows sugar release and provides essential building blocks. Carbohydrate portions must be modest.
Whole grains and starchy vegetables vary widely in GL. Wholemeal pasta and brown basmati rice are far better than white pasta or white rice. Swedes, carrots and squash are better than potatoes. Boiled potatoes are better than baked. French fries are the worst of all.
all.
| Starchy vegetables and cereals Pumpkin/squash Carrot Swede Quinoa (cooked) Beetroot Cornmeal Pearl barley (cooked) Wholemeal pasta (cooked) White pasta (cooked) Brown basmati rice (cooked) White rice (cooked) Couscous (soaked) Broad beans Sweetcorn Boiled potato Baked potato French fries Sweet potato | 7 GL points 1 large serving (185g) 1 large (158g) 1 large serving (150g) 1 large serving (120g) 1 large serving (112g) 1 serving (116g) 1 small serving (95g) half a serving (85g) a third of a serving (66g) 1 small serving (70g) a third of a serving (46g) a third of a serving (46g) 1 serving (31g) half a cob (60g) 3 small potatoes (74g) half (59g) a tiny portion (47g) half |
Beans and Lentils: Nature’s Blood Sugar Regulators
Beans and lentils are uniquely effective because they contain both protein and carbohydrate in one food. This keeps their GL low while allowing generous portions.
When combining beans with other starches, reduce the starch portion by half. A cup of lentils with half a cup of rice, not equal amounts.
By applying these principles you can restore blood sugar control, regain energy, reduce dementia risk, reverse type 2 diabetes and improve cognitive clarity.
The Proof Is in Your HbA1c
Red blood cells live for around three months. Follow a low GL diet for three months, then retest HbA1c.
This approach is detailed in The Low GL Diet Cookbook. Specific supplements can accelerate recovery, including fibre such as glucomannan, chromium and cinnamon compounds to improve insulin sensitivity, and HCA from tamarind to promote glucose burning rather than storage.
What to Do Next
If glycaemic load affects dementia risk, the next step is simple: measure, act, and check again.
Test your blood sugar resilience.
HbA1c shows how much sugar damage has occurred over the last three months. It is included in Food for the Brain’s DRIfT 5-in-1 home test, alongside other key brain health markers. If HbA1c is high, a low GL diet gives you a clear way to bring it down.
Check how your brain is functioning now.
The free Cognitive Function Test takes around 20 minutes and provides an objective snapshot of memory, attention and processing speed. Many people spot early changes years before any diagnosis.
Make changes, then retest.
Follow a low GL diet for three months, then re-test HbA1c and cognitive function to see whether the changes are working.
Prevention works best when it is measured.
References:
- Novau-Ferré N et al. Glycemic index, glycemic load, and risk of dementia: a prospective analysis within the UK Biobank cohort. Int J Epidemiol. 2025.
- Wasserman DH. Four grams of glucose. Am J Physiol



