In this guide, you’ll learn:
– What methylation is and why it matters.
– How homocysteine supports healthy methylation.
– Why methylation is important for brain, heart, and overall health.
– What causes homocysteine levels to rise.
– How to lower homocysteine through diet, lifestyle, and supplements.
– When homocysteine testing may be beneficial.
Methylation is a natural process that occurs in all living cells and is essential for normal growth, development, and overall health. It helps regulate how genes are switched on or off without changing the DNA sequence itself, allowing cells to perform different functions despite containing the same genetic information. Methylation and homocysteine are closely linked in biochemical pathways that affect cellular function and health. Methylation also contributes to maintaining genome stability and supporting normal cellular processes. Changes in normal methylation patterns have been linked to a range of diseases, including cancer, cardiovascular disease, and neurological disorders, highlighting its importance in both health and disease.
Homocysteine is a naturally occurring amino acid produced during the metabolism of methionine, an essential amino acid obtained from dietary protein. Although homocysteine is not obtained directly from food, it plays a central role in the methylation cycle as an intermediate in reactions that support normal cellular function. Under healthy conditions, homocysteine does not accumulate because it is continuously recycled or converted into other beneficial compounds through vitamin dependent metabolic pathways.
Efficient recycling of homocysteine depends on adequate levels of folate, vitamin B₁₂, and vitamin B₆. When these nutrients are deficient or the metabolic pathways become less efficient, homocysteine accumulates in the bloodstream and serves as a useful marker of impaired methylation and disrupted one carbon metabolism. Elevated homocysteine has been associated with an increased risk of cardiovascular disease, cognitive decline, pregnancy complications, and other chronic health conditions.
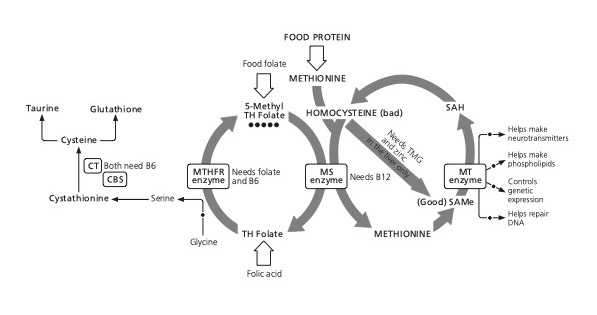
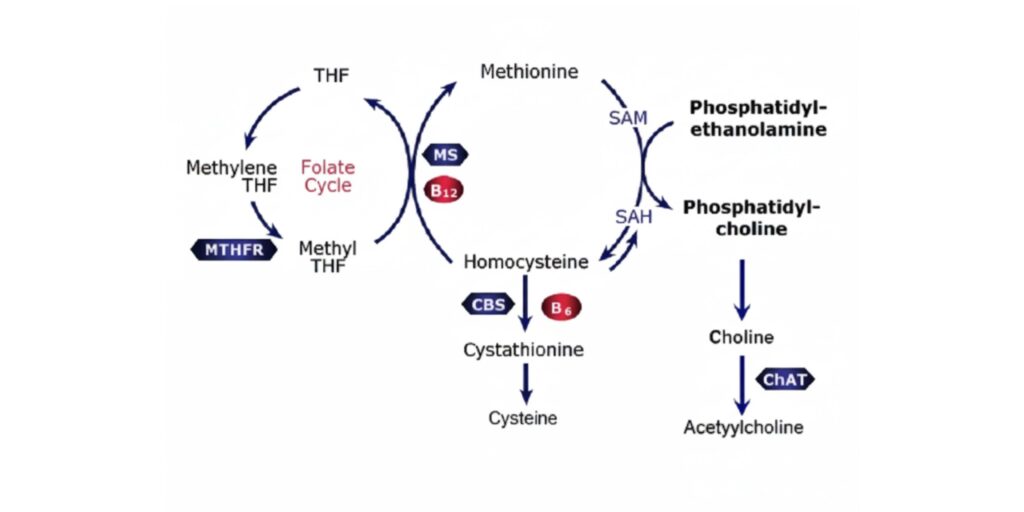
Methionine is an essential amino acid obtained from dietary protein and serves as the starting point of the methylation cycle. It is converted into S-adenosylmethionine (SAMe).
SAMe is the body’s primary methyl donor. It supplies methyl groups that are required for hundreds of biological reactions, including the regulation of gene expression, neurotransmitter synthesis, phospholipid production, and many other cellular processes.
During methylation, SAMe transfers a methyl group to molecules such as DNA, RNA, proteins, lipids, and neurotransmitters. These reactions regulate gene activity, support normal brain function, contribute to detoxification, and maintain numerous physiological processes. After donating its methyl group, SAMe is converted into homocysteine.
Homocysteine is a normal intermediate in the methylation cycle. Under healthy conditions, it is rapidly metabolised and does not accumulate. Instead, it follows one of two pathways: it is either recycled back into methionine to sustain the methylation cycle or converted into cysteine through the transsulfuration pathway, which ultimately contributes to the production of glutathione, one of the body’s most important antioxidants.
The remethylation of homocysteine back to methionine requires folate and vitamin B₁₂, while the transsulfuration pathway depends on vitamin B₆. Together, these vitamin dependent pathways maintain normal methylation and prevent excessive homocysteine accumulation. When they are impaired because of nutrient deficiencies, genetic variation, or other metabolic disturbances, homocysteine levels rise, making it a clinically useful marker of impaired one carbon metabolism.
If you’d like to see how this process works visually, this short animation provides a clear overview of the methylation cycle and the role of homocysteine below.
Methylation can become impaired when the body is unable to maintain an adequate supply of methyl groups or when the enzymes involved in the methylation cycle do not function efficiently. Common causes include deficiencies of key nutrients such as folate, vitamin B₁₂, and vitamin B₆, which are required to recycle homocysteine back into methionine. Genetic variations in enzymes involved in one carbon metabolism, such as the MTHFR gene, can also reduce methylation efficiency. In addition, factors including ageing, poor diet, smoking, excessive alcohol consumption, chronic disease, and certain medications may disrupt normal methylation patterns. Impaired methylation can lead to elevated homocysteine concentrations and altered DNA methylation, both of which have been associated with an increased risk of cardiovascular disease, neurological disorders, and other chronic health conditions.
Several other factors may also contribute to raised homocysteine and impaired methylation. These include smoking, excessive coffee or alcohol consumption, diabetes, rheumatoid arthritis, thyroid disorders, coeliac disease, Crohn’s disease, obesity, physical inactivity, chronic stress, and certain long term medications such as proton pump inhibitors and corticosteroids. Ageing and inherited genetic variants affecting enzymes involved in one carbon metabolism, including MTHFR, may further reduce the efficiency of methylation.
Methylation is involved in thousands of biochemical reactions that occur every second throughout the body. By transferring methyl groups to DNA, proteins, lipids, and other molecules, methylation helps regulate essential biological processes that support health throughout life. When methylation functions efficiently, it enables cells to grow, repair, communicate, and respond appropriately to their environment. Conversely, impaired methylation may contribute to elevated homocysteine levels and has been associated with an increased risk of several chronic diseases.
One of methylation’s most important functions is regulating gene expression. Rather than changing the DNA sequence itself, methylation influences whether certain genes are switched on or off, allowing different cells to perform specialised functions despite containing the same genetic information. Methylation also contributes to DNA repair and genome stability, helping to protect cells from accumulated damage over time.
Methylation is required for the production and regulation of several neurotransmitters, including dopamine, serotonin, noradrenaline, and melatonin. These chemical messengers play essential roles in mood, motivation, memory, learning, concentration, and sleep. Efficient methylation therefore supports normal brain function and psychological wellbeing. Learn more about the connection between methylation and mental health, including how methylation influences neurotransmitter production and emotional wellbeing.
Methylation contributes to the body’s natural detoxification processes by supporting the metabolism and elimination of a variety of compounds. It is also involved in the production of phospholipids that form healthy cell membranes, the synthesis of creatine for cellular energy, and numerous other metabolic pathways that maintain normal cell function throughout the body.
Healthy methylation helps regulate homocysteine metabolism by recycling homocysteine back into methionine. When this process becomes less efficient, homocysteine levels may rise, increasing the risk of vascular damage. Elevated homocysteine has been associated with cardiovascular disease, stroke, and impaired blood vessel function, making methylation an important contributor to cardiovascular health.
The brain has a particularly high demand for efficient methylation. Healthy methylation supports memory, learning, cognitive performance, and healthy ageing by maintaining nerve cells, supporting neurotransmitter production, regulating inflammation, and contributing to DNA repair. Elevated homocysteine has been linked with brain atrophy, cognitive decline, and an increased risk of dementia, making it one of the most widely studied biomarkers of brain health. Learn more in our dedicated guide to Homocysteine and Brain Health.
Key Takeaway
Methylation influences many of the body’s most important biological processes, from regulating genes and repairing DNA to producing neurotransmitters and maintaining cardiovascular and brain health. Because homocysteine reflects how efficiently the methylation cycle is functioning, measuring and managing homocysteine levels can provide valuable insights into overall health and may help identify opportunities for early nutritional intervention.
| If methylation is working well | If methylation is impaired |
| Healthy homocysteine levels | Elevated homocysteine |
| Efficient DNA repair | Reduced DNA repair |
| Normal neurotransmitter production | Mood and cognitive changes |
| Healthy blood vessels | Increased cardiovascular risk |
| Supports healthy ageing | Higher risk of chronic disease |
Elevated homocysteine is a modifiable risk factor that can often be reduced through appropriate nutritional and lifestyle interventions. As homocysteine is an intermediate in the methylation cycle, maintaining healthy concentrations supports normal methylation and one carbon metabolism. Reducing elevated homocysteine is therefore considered an important strategy for promoting metabolic health and may contribute to lowering the risk of cardiovascular disease, cognitive decline, and other conditions associated with impaired methylation.
The most effective way to lower homocysteine is to ensure an adequate supply of the nutrients required for its metabolism, particularly folate, vitamin B₁₂, and vitamin B₆. These vitamins enable homocysteine to be recycled back into methionine, allowing the methylation cycle to continue efficiently. Alongside adequate nutrient intake, lifestyle factors such as regular physical activity, avoiding smoking, limiting alcohol consumption, and maintaining a balanced diet also support healthy homocysteine metabolism. You can learn more about the science and practical strategies for lowering homocysteine in our dedicated guide.
Diet is the first step in supporting healthy homocysteine levels. Many foods naturally provide the folate and B vitamins required for efficient methylation, making dietary intake the foundation of homocysteine management. Discover which foods help lower homocysteine and how they can support healthy methylation.
Although a balanced diet is sufficient for many individuals, some people may require additional nutritional support. Older adults, individuals with vitamin deficiencies, reduced nutrient absorption, or genetic variations affecting one carbon metabolism may benefit from targeted supplementation. Clinical research has consistently demonstrated that supplementation with folic acid, vitamin B₁₂, and vitamin B₆ can effectively lower homocysteine concentrations. Read more about supplements for lowering homocysteine, including the evidence supporting key nutrients involved in methylation.
Before deciding on dietary or supplement interventions, it is helpful to know your current homocysteine level. Testing provides an objective measure of methylation efficiency and can identify individuals who are most likely to benefit from targeted nutritional support.
Testing homocysteine levels provides a practical way to assess the efficiency of the methylation cycle and identify individuals who may benefit from dietary or nutritional intervention. As elevated homocysteine can occur without obvious symptoms, testing offers an opportunity to detect impaired one carbon metabolism before it contributes to long term health problems. A simple blood test, performed either in a clinical laboratory or using a validated home blood spot kit, measures the concentration of homocysteine in the blood. For the most accurate result, testing is typically carried out after an overnight fast, as recent food intake, particularly high protein meals, can temporarily increase homocysteine levels.
Although reference ranges vary between laboratories, evidence suggests that disease risk begins to increase well before homocysteine reaches the traditional upper limit of 15 µmol/L. Some researchers have proposed that concentrations above approximately 6 to 7 µmol/L may already indicate suboptimal methylation and increased long term health risk. For this reason, homocysteine is increasingly viewed as a marker to optimise rather than simply a value that should remain within the laboratory reference range.
Homocysteine results should be interpreted alongside an individual’s nutritional status, medical history, and other clinical findings, as an elevated level is a biomarker of impaired methylation rather than a diagnosis of a specific disease. If homocysteine concentrations are raised, dietary modification, optimisation of folate and B vitamin intake, and where appropriate, targeted supplementation can often reduce levels. Repeat testing after several months may be useful to monitor the effectiveness of these interventions and ensure that homocysteine has returned to a healthy range.
Further information on preparing for a homocysteine test, interpreting results, and recommended follow up can be found in the Food for the Brain Homocysteine Testing Guide.
Measuring homocysteine is one of the most useful ways to assess methylation efficiency and identify nutritional imbalances that may increase long term disease risk. While the previous sections explain why homocysteine is important, the following expert guide provides a more detailed overview of how homocysteine is measured, how results should be interpreted, and the practical considerations involved in laboratory testing.
Measurement of Homocysteine
written by Dr Gillian Hart BSc (Hons), PhD, Cert Mgmt (Open), MIBMS
The importance of homocysteine as a risk factor is becoming much more familiar as evidence grows. An increasing number of studies now show that homocysteine predicts potential health problems. It is clear now that raised plasma homocysteine concentrations both predict and precede the development of cardiovascular disease including stroke. A study (published in the British Medical Journal) showed homocysteine level in blood plasma predicts risk of death from cardiovascular disease in older people even better than any conventional measure of risk including cholesterol, blood pressure or smoking.
Raised levels of homocysteine are also linked to Alzheimer’s, dementia, declining memory, poor concentration and judgment and lowered mood. Women with high homocysteine levels find it harder to conceive and are at risk from repeated early miscarriage. High homocysteine has also been linked to migraines. Those with conditions such as diabetes and osteoporosis are at increased risk of raised homocysteine levels. Finally,homocysteine has been shown to play a crucial role as a key marker for disease development. It can even determine longevity and health throughout a person’s lifespan.
Homocysteine is a naturally occurring amino acid that the body produces during the methylation process. It has the formula C4H9NO2S and appears in blood plasma as a protein derivative when body chemistry is out of balance. A homologue of the amino acid cysteine, differing by an additional methylene (-CH2-) group, it is not obtained from the diet. Instead, it is biosynthesized from methionine via a multi-step process that probably occurs in every cell of the body (Figure 1).
Methionine is an amino acid, ingested as a component of food protein. It is found primarily in meats, eggs, dairy products, fish, chicken, seeds, nuts and some vegetables. Methionine is activated to S-adenosylmethionine (SAM) by the enzyme methionine adenosyltransferase. Circulating levels of homocysteine are usually low due to its rapid metabolism via one of two pathways:
The body relies heavily on vitamin derived cofactors to metabolise homocysteine. When levels of vitamin B12, folic acid or vitamin B6 are low, homocysteine levels rise and hyperhomocysteinaemia can develop. Homocysteine can accumulate in the body causing cell damage and the onset of major disease. The reason is because the biochemical transformation process is not working properly, usually due to lack of these needed vitamins. If these pathways are lacking the required vitamins and minerals, dangerous homocysteine levels and potential ill health can result.
The proposed mechanisms by which hyperhomocysteinaemia can cause harm are common to several conditions. For example, vascular damage, cognitive impairment, neurological complications, congenital defects and pregnancy complications
A detailed review of these mechanisms is outside the scope of this article. However, raised homocysteine is associated with damage to the arteries. One mechanism involves homocysteine interfering with how cells use oxygen, which results in a build up of damaging free radicals. Oxidation triggers many diseases including heart disease, strokes, cancers and autoimmune diseases.
Reactive chemical forms, such as free radicals, can oxidize low-density lipoproteins producing oxy-cholesterols and oxidized fats and proteins within developing arterial plaques. This oxidation injury, along with changes in nitric oxide metabolism, appears to contribute to the damage caused. Researchers suggest that methylation defects and impaired DNA repair caused by disturbed folate metabolism contribute to carcinogenesis.
Nitric oxide is an important regulator and mediator of numerous processes in the nervous, immune and cardiovascular systems, and decreased methylation.
Homocysteine also stimulates the growth of smooth muscle cells, causing deposition of extracellular matrix and collagen. In turn this causes a thickening and hardening of artery walls. Overall though, the exact mechanisms involved in the increased risk of ill health with raised homocysteine, still remain a mystery in many respects. More studies are needed to elucidate the exact associations.
Many factors are thought to raise levels of homocysteine. Among these are poor diet, poor lifestyle especially smoking and high coffee and alcohol intake.
Additional factors include some prescription drugs, diabetes, rheumatoid arthritis and poor thyroid function as well as with chronic inflammatory diseases in general, and some intestinal disorders such as coeliac and Crohn’s diseases.
Levels increase with age and higher levels are more common in men than women. Levels can also increase with oestrogen deficiency and with some long term medications, including corticosteroids. Strict vegetarians and vegans may also be at risk as well as people who suffer from stress.
As with cholesterol, family history and genetic make-up can play a part in causing raised levels, as can obesity and lack of exercise. Even people with an active, healthy lifestyle may still be at risk, if there is a family history of high levels of homocysteine or disease.
Researchers have identified a rapidly increasing number of variations in the genes that regulate the enzymes involved in methionine metabolism. Reduction in the activity of genes such as the one that regulates the enzyme methyl-enetetrahydrofolate reductase (MTHFR) increases mean homocysteine levels. This gene is present in its homozygous form in about 10% of most European populations. However, the frequency varies widely geographically and between different ethnic populations.
The measurement of total homocysteine which includes the sum of the concentrations of free and bound homocysteine in the blood plasma, is technologically difficult. After blood sampling, the blood cells produce and release homocysteine. This results in an increase in measured levels of about 10 percent per hour at room temperature. Thus it is vital to follow a specific process within 30 minutes of collection:
Collect blood plasma (using EDTA or heparin to prevent coagulation) and then centrifuge the sample to remove the blood cells from the plasma. Even the most efficient transport from clinic or GP practice to laboratory centrifuge rarely renders this feasible. Collection of blood serum is not appropriate due to the relatively long clotting time required. Once separated from the blood cells the homocysteine is stable in plasma for at least 4 days at room temperature, and much longer refrigerated or frozen.
Some manufacturers now provide blood collection vacutainers, which contain a stabiliser solution that can help delay the urgent need for centrifugation.
There are several other important factors to consider when blood sampling. As methionine, ingested as protein in the diet, is the only source of homocysteine, it would be expected that food intake would cause increased concentrations of homocysteine in plasma. A protein rich meal can significantly raise total homocysteine levels, so clinicians generally recommend that the person taking the test should be overnight fasted at the time of blood sampling.
Urine homocysteine measurement is not useful as renal excretion does not seem to be an important route of elimination. Only about 1% of the homocysteine filtered by the glomeruli is normally found in the urine. The rest is reabsorbed and metabolized. In saying that, some GPs do offer urine measurement, as it is easy to collect. However, you should interpret the results with caution because they are likely to detect only extreme hyperhomocysteinaemia.
The increased need in clinical chemistry laboratories for methods of homocysteine determination, in correlation with cardiovascular diseases and nutritional deficient status, has led to the development of different analytical methods for measurement.
Methods include amino acid analysis, high performance liquid chromatography (HPLC), capillary electrophoresis, gas chromatography-mass spectrometry (GC-MS) and immunoassay. HPLC is the gold standard reference method. Different total homocysteine measurement methods do usually give comparable results. However, because methods and laboratories vary, you should use caution when comparing values obtained from different laboratories.Studies have shown that single measurements can classify persons with respect to their average plasma homocysteine level quite well. However, because inter-method and inter-laboratory variability can affect results, you should monitor homocysteine concentrations over time using the same method and the same laboratory. Choosing laboratory testing services is thus a critical process.
There is no consensus about the upper reference limits for plasma homocysteine concentrations. Among apparently healthy individuals “normal” concentrations commonly range from 5 to 15µmol/L. However, studies on targeted segments of the population have shown that the upper limit of 15µmol/L is far too high in well-nourished populations without obvious vitamin deficiency. It is clear now that each increase of 5µmol/L in homocysteine level increases the risk of coronary heart disease events by approximately 20%, independently of traditional coronary heart disease risk factors. Risk for coronary artery disease increases across a continuum of homocysteine concentrations, with substantial risk appearing between 10 and 15 µmol/L.Some report that any homocysteine measurement over 6.3µmol/L represents an increased risk.
There is little doubt that homocysteine measurement will become a routine screening tool for risk assessment in the future, but that current reference limits will change from being based on values from a presumed normal healthy population towards a baseline where ‘normal’ is the optimum level. Experts recommend carefully monitoring homocysteine levels.
The good news is that many people can normalise high homocysteine levels. Evidence shows that diet and vitamin supplementation effectively reduce plasma homocysteine. It is clear though that vitamin supplementation can normalise levels even when serum vitamin levels are within the normal range, or even in the high range. Metabolic, environmental and genetic factors make it virtually impossible to determine individual nutritional requirements without first carrying out a homocysteine test; the test result can then define the diet and supplementation regime required. The most important nutrients that help lower homocysteine levels are folate, the vitamins B12, B6 and B2, zinc and trimethylglycine (TMG).
This article has provided an overview of the importance of homocysteine measurement, whilst highlighting some of the limitations associated with sample handling and testing. There will always be people who are at high risk of raised homocysteine, but the only way to find out definitively is to perform a validated homocysteine test, and then monitor levels regularly going forwards.
Dr Gill Hart is a Biochemist with over twenty-five years’ experience in the development and evaluation of hospital standard tests and testing services.
References
1. de Ruijter, W. et al, “Use of Framingham risk score and new biomarkers to predict cardiovascular mortality in older people: population based observational cohort study”. British Medical Journal, 2009, 338: a3083.
2. Seshadri, S. et al, “Plasma homocysteine as a risk factor for dementia and Alzheimer’s disease”. New England Journal of Medicine, 2002, 346:476-483.
3. Rugolo, S. et al, “Hyperhomocysteinemia: associated with obstetric diabetes and fetal malformations”. Minerva Ginecologica, 2005, 57:619-25.
4. Savage, D. et al “Sensistivity of serum methylmalonic acid and total homocysteine determinations for diagnosing cobalamin and folate deficiencies”. American Journal of Medicine, 1994, 96:239-46.
5. Klee, G. “Cobalamin and folate evaluation; measurement of methylmalonic acid and homocysteine vs vitamin B12 and folate”. Clinical Chemistry, 2000, 46:1277-83.
6. Bolander-Gouaille, C. In “Focus on homocysteine and the vitamins involved in its metabolism”. Published by Springer-Verlag, France, 2002, Chapter 3, p33.
7. Upchurch, G. et al, “Homocysteine, EDRF and endothelial function”. Journal of Nutrition, 1996, 126:1290S-1294S.
8. Cortelezzi, A. et al, “Hyperhomocysteinemia in myelodysplastic syndromes: specific association with autoimmunity and cardiovascular disease”. Leukemia & Lymphoma, 2001, 41:147-50.
9. Mutus, B et al, “Homocysteine-induced inhibition of nitric oxide production in platelets: a study on healthy and diabetic subjects”. Diabetologia, 2001, 44: 979-82.
10. Duthie, S. “Folic acid deficiency and cancer: mechanisms of DNA instability”. British Medical Bulletin, 1999, 55:578-92.
11. Robertson, K. “DNA methylation, methyltransferases, and cancer”. Oncogene, 2001, 20:3139-55
12. Carmody, B. et al, “”Folic acid inhibits homocysteine-induced proliferation of human arterial smooth muscle cells”. Journal of Vascular Surgery, 1999, 30: 1121-8.
13. Majors, A. et al, “Homocysteine as a risk factor for vascular disease. Enhanced collagen production and accumulation by smooth muscle cells”. Arteriosclerosis Thrombosis and Vascular Biology, 1997, 17:2074-81.
14. Bolander-Gouaille, C. and Bottiglieri, T. In “Homocysteine related vitamins and neuropsychiatric disorders”. Published by Springer-Verlag, France, 2003, pp58-108.
15. Rozen, R. “Genetic modulation of homocysteinemia”. Seminars in Thrombosis and Hemostasis, 2000, 26: 255-61.
16. Wilcken, B. et al, “Geographical and ethnic variation of the 677C>T allele of 5,10 methylenetetrahydrofolate reductase (MTHFR): findings from over 7000 newborns from 16 areas world wide”. Journal of Medical Genetics, 2003;40:619-625.
17. European Patent EP1518118
18. Rasmussen, K. and Møller, J. “Total homocysteine measurement in clinical practice”. Annals of Clinical Biochemistry, 2000, 37: 627-648.
19. Refsum, H. et al, “Facts and Recommendations about total homocysteine determination: an expert opinion”. Clinical Chemistry, 2004, 50: 3–32.
20. Garg, U. et al, “Short-term and long-term variability of plasma homocysteine measurement”. Clinical Chemistry, 1997, 43: 141-145.
21. Hart, G. “Fundamentals to look for when choosing laboratory testing services”. Nutrition Practitioner, 2008, Spring/Summer.
22. Bolander-Gouaille, C. In “Focus on homocysteine and the vitamins involved in its metabolism”. Published by Springer-Verlag, France, 2002, Chapter 8, p206.
23. Nygard, O. et al, “Major lifestyle determinants of plasma total homocysteine distribution: the Hordaland Homocysteine Study”. American Journal of Clinical Nutrition, 1998, 67:263-70.
24. Ubbink, J. et al, “Results of B-vitamin supplementation study used in a prediction model to define a reference range for plasma homocysteine”. Clinical Chemistry, 1995,41:1033-7.
25. Humphrey, L. et al, “Homocysteine level and coronary heart disease incidence: a systematic review and meta-analysis”. Mayo Clinic Proceedings, 2008, 83:1203-12.
26. Robinson, K. et al, “Hyperhomocysteinemia and low pyridoxal phosphate: common and independent reversible risk factors for coronary artery disease”. Journal of Circulation, 1995, 92:2825-30.
27. Holford, P. and Braly, J. (2003) “The H Factor”. Published by Piatkus, UK.
28. Nilsson, K. et al, “Plasma homocysteine in relation to serum cobalamin and blood folate in a psychogeriatric population”. European Journal of Clinical Investigation, 1994, 24:600-6.
29. Faurshou, M. et al, “High prevalence of hyper-homocysteinemia due to marginal deficiency of cobalamin or folate in chronic myeloproliferative disorders”. American Journal of Hematology, 2000, 65: 136-40.
