After 40 failed trials for drugs injecting anti-amyloid antibodies (AAAs) one, Lecanemab[i], has finally shown a modest benefit on cognitive function in those with early-stage Alzheimer’s. But they come with a terrible cost – adverse effects that include brain swelling and haemorrage which occurred in one in five trial participants.. When a similar drug, Aducanumab, was conditionally approved by the US FDA last year, despite nine out of ten of their experts voting against it, many resigned in protest[ii]. Yet the pressure on pharma to get an amyloid drug to market, having spent over $42 billion[iii], is immense.
Let’s consider the alternative
Prevention with simple, doable changes to diet, lifestyle and supplementation with B vitamins and omega-3 fish oils.
The two most relevant measures of success of any treatment are reduction in the rate of brain shrinkage and a reduction in clinical dementia symptoms which lead to a diagnosis.
In relation to brain shrinkage the best AAAs have achieved is 2% less brain shrinkage. In a landmark trial by Professor David Smith and colleagues at the University of Oxford, B vitamin supplements, given to those with pre-dementia (mild cognitive impairment) have achieved a reduction in the rate of brain shrinkage of 52%, up to 73% in those with sufficient omega-3.[i] This effect was shown in those with raised blood levels of homocysteine, a marker for B vitamin status that is raised in approximately half of pre-dementia patients and many more with Alzheimer’s. We now know that B vitamins need omega-3 to make the biggest difference, and vice versa.[ii]
Clinical Dementia Rating (CDR) with B vitamins and Omega 3’s
What about actual clinical improvement, called Clinical Dementia Rating (CDR), which is what counts for the person concerned? A CDR score of zero means no clinically significant cognitive impairment. In the Oxford trial on B vitamins 65% of participants on B vitamins with higher omega-DHA status ended the 2 year trial with a clinical dementia rating of zero compared with 25% receiving placebo.[i] It was more than twice as effective as the recent drug. In a Swedish omega-3 trial those with sufficient B vitamin status, also had a marked reduction in clinical dementia rating, which was reduced by 1.5 points compared with placebo after 6 month’s treatment with omega-3.[ii] The improvement in clinical dementia rating reported for Lecanemab, which was a modest 0.45 point reduction. This was marginally better than a 0.39 difference for Aducanumab, compared to placebo.[iii][iv] In other words, no AAA drug has even reduced a CDR score by 1 point but both B vitamins and omega-3 have.
A trial in Holland, called B-proof, which had shown no significant effects overall in those supplementing B vitamins, recently reported that those with higher Omega-3 levels had a significant improvement in cognitive function. A French[i] and Chinese study[ii] reported a similar finding – the combination of B vitamins and omega-3 shows clear improvements in cognitive function – better than achieved by AAA drugs, without adverse effects.
So, on all three counts – brain shrinkage, cognitive function and clinical dementia rating – B vitamins plus omega-3 – wins out at a fraction of the cost since nutrients cannot be patented which is the requirement for the scale of profitability required by pharma.
Blood Sugar Levels and their impact
But, there’s two other points to make. Firstly, B vitamin and omega-3 status are but two of eight known actions that reduce risk or improve these critical criteria. Others are sugar, antioxidant rich fruit and veg, vitamin D, exercise, cognitive stimulation, gut health, sleep and stress.[i] Having a high blood sugar level from age 35 predicts Alzheimer’s risk.[ii] Being diabetic or having high insulin levels, which is a consequence of eating too many refined sugar and carbs, doubles risk.[iii] Having a high carb intake is associated with increasing amyloid plaques in the brain – so why not tackle the upstream cause? One study reported that “Those who ate the healthiest diet had an 88% decreased risk of developing dementia and a 92% decreased risk of developing Alzheimer’s disease.”[iv]Increasing lean muscle mass with resistance exercise is associated with better cognitive function and brain volume.[v]The charity foodforthebrain.org have a free, validated online Cognitive Function Test, followed by a Dementia Risk Index questionnaire, that not only measures your cognitive function, but also shows you exactly what your risk is and how to reduce it by targeting your ‘weakest links’ in these eight known prevention steps.
Then, there’s the issue of side-effects. For each of these prevention steps there are none. Or rather, there are plenty – less risk for diabetes, heart disease, arthritis, premature ageing, better energy, sleep and weight control to name a few.
For the AAA drugs the side-effects are potentially devasting. Since one in five can be expected to experience brain swelling and microbleeds, regular brain scans will be necessary to monitor for these frequent complications. Is it right to expose an older person with cognitive decline to this scale of risk and medical intervention for such a modest benefit? The annual cost of treatment is expected to be above $10,000 but that doesn’t include the cost of medical monitoring or the cost of treatment when things go wrong. The cost benefit equation just doesn’t add up.
Early Intervention
Writing in the Financial Times last year Professor Smith says “ Your editorial is correct in saying ‘A resurrection of the amyloid approach must not divert resources and attention away from other ways to tackle dementia, which are in earlier stages of research and might give better results.’ These alternative approaches include identifying and then treating modifiable risk factors for dementia, of which about a dozen are already known. These account for about half of the cases of Alzheimer’s disease .” The high price proposed for the drug is disturbing, especially when a very much cheaper alternative treatment is available: high-doses of B vitamins and omega-3 from seafood or supplements. He estimates that early intervention , targeting all the prevention steps recommended by the Food for the Brain Foundation could cut a person’s risk by two thirds.
WE currently have 2 events on sale so that you can take a deep dive on this topic: ⭐️ MASTERCLASS – 4 hour conference with world leading experts on Alzheimer’s – Practitioner level. Book tickets here: https://foodforthebrain.org/aipmasterclass/
🧠 Upgrade Your Brain – 8 steps to reduce your Alzheimer’s risk with with Patrick Holford – A condensed version of the masterclass that is 90 minutes long and aimed at the general public. Book your tickets here: https://www.eventbrite.co.uk/e/upgrade-your-brain-tickets-415953948457
Food for the Brain is a non-for-profit educational and research charity that offers a freeCognitive Function Testand assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing theCognitive Function Testyou are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices.
[1] Oulhaj A, Jernerén F, Refsum H, Smith AD, de Jager CA. Omega-3 Fatty Acid Status Enhances the Prevention of Cognitive Decline by B Vitamins in Mild Cognitive Impairment. J Alzheimers Dis. 2016;50(2):547-57. doi: 10.3233/JAD-150777. PMID: 26757190; PMCID: PMC4927899.
[2] Jernerén F, Cederholm T, Refsum H, Smith AD, Turner C, Palmblad J, Eriksdotter M, Hjorth E, Faxen-Irving G, Wahlund LO, Schultzberg M, Basun H, Freund-Levi Y. Homocysteine Status Modifies the Treatment Effect of Omega-3 Fatty Acids on Cognition in a Randomized Clinical Trial in Mild to Moderate Alzheimer’s Disease: The OmegAD Study. J Alzheimers Dis. 2019;69(1):189-197. doi: 10.3233/JAD-181148. PMID: 30958356.
[3] Cummings JL, Goldman DP, Simmons-Stern NR, Ponton E. The costs of developing treatments for Alzheimer’s disease: A retrospective exploration. Alzheimers Dement. 2022 Mar;18(3):469-477. doi: 10.1002/alz.12450. Epub 2021 Sep 28. PMID: 34581499; PMCID: PMC8940715.
[6] Oulhaj A, Jernerén F, Refsum H, Smith AD, de Jager CA. Omega-3 Fatty Acid Status Enhances the Prevention of Cognitive Decline by B Vitamins in Mild Cognitive Impairment. J Alzheimers Dis. 2016;50(2):547-57. doi: 10.3233/JAD-150777. PMID: 26757190; PMCID: PMC4927899.
[7] Jernerén F, Cederholm T, Refsum H, Smith AD, Turner C, Palmblad J, Eriksdotter M, Hjorth E, Faxen-Irving G, Wahlund LO, Schultzberg M, Basun H, Freund-Levi Y. Homocysteine Status Modifies the Treatment Effect of Omega-3 Fatty Acids on Cognition in a Randomized Clinical Trial in Mild to Moderate Alzheimer’s Disease: The OmegAD Study. J Alzheimers Dis. 2019;69(1):189-197. doi: 10.3233/JAD-181148. PMID: 30958356.
[9] Awaiting actual Lecanemab, trial – see press release ref 1 above
[10] Maltais M, de Souto Barreto P, Bowman GL, Smith AD, Cantet C, Andrieu S, Rolland Y. Omega-3 Supplementation for the Prevention of Cognitive Decline in Older Adults: Does It Depend on Homocysteine Levels? J Nutr Health Aging. 2022;26(6):615-620. doi: 10.1007/s12603-022-1809-5. PMID: 35718871.
[11] Li M, Li W, Gao Y, Chen Y, Bai D, Weng J, Du Y, Ma F, Wang X, Liu H, Huang G. Effect of folic acid combined with docosahexaenoic acid intervention on mild cognitive impairment in elderly: a randomized double-blind, placebo-controlled trial. Eur J Nutr. 2021 Jun;60(4):1795-1808. doi: 10.1007/s00394-020-02373-3. Epub 2020 Aug 28. PMID: 32856190.
[13] Zhang X, Tong T, Chang A, Ang TFA, Tao Q, Auerbach S, Devine S, Qiu WQ, Mez J, Massaro J, Lunetta KL, Au R, Farrer LA. Midlife lipid and glucose levels are associated with Alzheimer’s disease. Alzheimers Dement. 2022 Mar 23. doi: 10.1002/alz.12641. Epub ahead of print. PMID: 35319157.
What makes us humans so different to other apes is our larger brain, especially the cortex. It is three times larger than a chimpanzee. How did this happen? How did Homo Sapiens evolve our level of intelligence despite sharing almost the same genes?
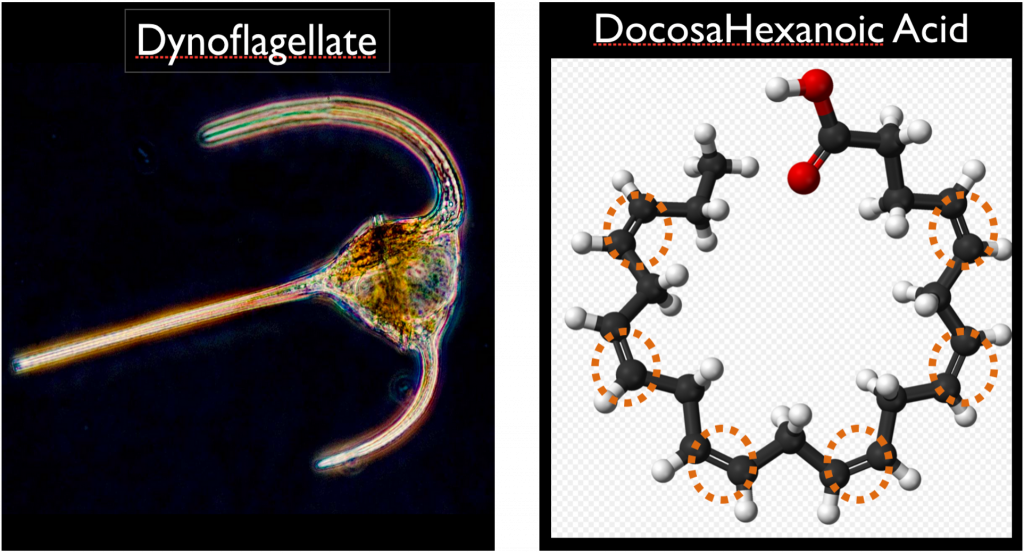
The brain’s origin, for all species, is from the ocean. It had to be as that is where life began. Millions of years ago the rudimentary eye cell, dinoflagellate, which is a type or marine phytoplankton, used a specific fat – the omega-3 fat docosahexanoic acid (DHA) – to convert solar photon energy into the first nerve impulse or twitch – a twitch towards food. That is the origin of the nervous system and brain.
Back in the ‘80’s, when zoologist Professor Michael Crawford analysed the types of fat in different animal’s organs and muscles they varied according to their dietary environment, except the brain. He discovered that the brain is always rich in DHA. The more DHA the brighter the animal, with the sea mammals and us humans having exceptionally high levels.
Recently it has been proven that DHA (docosahexanoic acid) has a unique structure involving six double bonds, arranged in a horseshoe shape, which actually makes it a semi-conductor with unique electrical properties. Its close cousins, ALA (alpha linolenic acid) in chia or flax, and EPA (eicosapentanoic acid) don’t have this potential. It’s all about DHA. While some EPA converts into DHA less than 1 per cent of ALA in plant-based sources of omega-3 such as chia seeds converts to DHA, the richest source of which is marine-based food from rivers and the sea.
Over 6 million years ago our hominid ancestors split from other apes (chimps, gorillas and bonobos), culminating in Homo Sapiens around 100,000 years ago. It clearly wasn’t genes that made us different. We share 98.5% of the same genome. It had to be the environment our ancestors exploited. During this time brain size steadily increased up to 1.45kg 10,000 years ago, roughly three times the size of a chimpanzee, at 384g.
Homo Aquaticus
We have over twenty profound anatomical, physiological and biochemical differences apart from our vastly different psychological advancement as in intelligence and language. More than anything, it is this, illustrated by our brain size, that makes us different. But, before looking closely at the circumstances, and diet, that almost certainly drove our gain in brain size and intelligence, let’s take a look at the fundamental differences we have. These have been so clearly delineated in an excellent book, The Waterside Ape, by Peter Rhys-Evans, and ear, nose and throat surgeon. He explores why we:
Stand upright
Have (virtually) no body hair
Have a layer of sub-cutaneous fat
A waxy, waterproof layer, the vernix, at birth
A diving reflex at birth, meaning we are able to swim before we can walk, and hold our breath underwater
A descended larynx, a precursor of being able to have complex language/speaking
Enlarged sinus cavities
A nose shape that is good for keeping the water out while swimming
Ears that actually form a protective boney protusion in those who spend a lot of time diving
Different kidneys, in how they filter salt and water
Manual dexterity
Crinkly fingers when in water for a few minutes
Of course, the story we’ve all been told is that we came out of the trees, into the savannah and stood upright for better hunting. Anyone who has been on safari will know that a) you don’t stand a chance catching anything by standing upright – you crawl; and b) all the good hunters can sprint much faster than man (lion 80kph, leopard 60kph, cheetah 100kph, man under 30kph) precisely because four legs are better than two. But, can you explain any one of these other changes, let alone our increase in intelligence, by moving from the trees into the savannah for hunting? If so, how did we suddenly develop manual dexterity, tools and spears overnight to even survive? Also, why do certain ‘sea nomad’ tribes exist, such as the Moken and Bajou, who can hold their breath for up to 10 minutes under water, spending up to five hours a day in the sea, giving birth in the sea? Their spleen is adapted to oxygenate tissue, as it is in dolphins, to enable long dives. Where did that evolutionary adaptation come from?
The only logical explanation that I have encountered, which eloquently fits all these adaptations, in that our hominid ancestors exploited the waterside – wetlands, swamplands, rivers, estuaries and coasts. In the process of so doing, became upright, and started to eat a diet high in marine foods, providing the essential nutrients for brain development, that is omega-3 DHA, phospholipids, plus vitamin B12, iodine, and all those other essential elements from magnesium to selenium. From this perspective let’s briefly examine all the changes listed above, between us and other apes:
Stand upright – better for wading in water, so gradually our anatomy adapts but, even so, we are prone to the problems of uprightness, eg hips and knees because it is anatomically inferior to walk on all fours, with better weight distribution.
Have (virtually) no body hair and a layer of sub-cutaneous fat – consistent with semi-aquatic mammals better for floating and insulation
A waxy, waterproof layer, the vernix, at birth – found in no land mammals, only other semi-aquatic mammals such as seals and chemically identical
A diving reflex at birth, meaning we are able to swim before we can walk, and hold our breath underwater
A descended larynx, a precursor of being able to have complex language/speaking – being upright, and diving, could have led to this vital adaptation. This, by the way, only occurs after a year or so, before which a baby’s language cannot develop the complexity of sounds and voice control only we have
Enlarged sinus cavities, which help to keep the head above water, but still have drainage holes in the ‘wrong’ place, eg good if on all fours but bad if upright, which is why we are prone to sinus problems.
A nose shape that is good for keeping the water out while swimming
Ears that actually form a protective boney protusion in those who spend a lot of time diving
Manual dexterity – if we were wading, and swimming, not walking on all fours, we have ‘free’ hands. Opening shells would develop manual dexterity.
Crinkly fingers when in water for a few minutes – perfect for catching fish.
Part of the idea of the ‘savannah’ theory is that food became scarce with climate changes so we switched to hunting. But the water’s edge was, until recently, abundant with easily accessible food. Even 200 years ago, in 1706, Daniel Dafoe wrote this regarding the Firth of Forth. “Off the Pentland Firth the sea was one third water and two thirds fish; the operation of taking them could hardly be call’d fishing, for they did little more than dip for them into the water and take them up.” Our estuaries were packed with mussels, oysters and crabs.
Historically, wherever early man is found so too is evidence of seafood consumption, with remains of shells, fish bones etc. from Pinnacle Point in South Africa, where early remains are found together with sea shells, to Wales. When a 40,000 year old Homo sapiens was found in the Gower peninsular DNA evidence showed that a quarter of their diet was seafood.
A marine food diet high in critical brain building nutrients, especially DHA, phospholipids and B12, is the best explanation for our cerebral expansion. “Docosahexaenoic acid (DHA), the omega-3 fatty acid that is found in large amounts in seafood, boosts brain growth in mammals. That is why a dolphin has a much bigger brain than a zebra, though they have roughly the same body sizes. The dolphin has a diet rich in DHA. The crucial point is that without a high DHA diet from seafood we could not have developed our big brains. We got smart from eating fish and living in water.” says Crawford.
The dry weight of the brain in 60 per cent fat and DHA makes up over 90 per cent of the structural fat of neurons (brain and nerve cells). The intelligent membrane that makes up all neurons is composed of phosphorylated DHA – that is DHA attached to phospholipids. The most abundant phospholipid is phosphatidyl choline, found predominantly in fish, eggs and organ meats. These are bound together by a process called methylation, itself dependent on vitamins B12, folate and B6. While folate and B6 is found in both plant foods and seafood, B12 is only found in foods of animal origin, and is especially high in all marine foods.
The evidence that exists suggests we were eating a diet rich in marine food, as well as plant foods along the water’s edge, enjoying the ‘fruité del mare’. We would have eaten much more than we do today – at least double the calories. Today’s convenience world has dramatically reduced the calories we need to expend hunting and gathering food, travelling and staying warm.
The idea that we were eating twice as much and at least a quarter from marine foods makes sense of what we know about the optimal intake of both omega-3 fats rich in DHA, phospholipids and vitamin B12, lack of which are the main drivers of today’s endemic dementia. This would be equivalent to at least half our diet today needing to be from marine foods rich in fats.
Optimal amounts of omega-3 from seafood is estimated at 2 grams a day by Joseph Hibbeln at the US National Institute’s of Health, while choline is estimated at 400mg to 800mg. An optimal intake of B12 is probably 10mcg. None of these can easily be achieved even by eating seven servings of oily fish a day. (Choline is rich in all fish, but DHA is only rich in oily fish, fish roe and liver.)
In the chart below the last column combines EPA and DHA and shows the amount provided in an 85g serving. None provide 2,000mg, although they do get close, suggesting that we would have needed to eat at least a serving of fish or seafood a day, if not more.
Fish and Seafood (per 85g)
EPAmg
DHAmg
EPA+DHAmg
Atlantic Salmon (farmed)
587
1238
1825
Atlantic Herring
773
939
1712
Atlantic Salmon (wild)
349
1215
1564
Bluefin Tuna
309
970
1279
Mackerel (canned)
369
677
1046
Sockeye Salmon (wild)
451
595
1046
Rainbow Trout (farmed)
284
697
981
Sardines (canned)
402
433
835
Albacore (or white) Tuna (canned)
198
535
733
Shark (raw)
267
444
711
Swordfish
117
579
696
Sea Bass
175
473
648
Pollock
77
383
460
Flat Fish (Flounder/Sole)
207
219
426
Halibut
77
318
395
Oysters (farmed)
195
179
374
Dungeness Crab
239
96
335
Scallops
141
169
310
Mixed Shrimp
145
122
267
Clams
117
124
241
Yellowfin Tuna
40
197
237
Catfish (wild)
85
116
201
Catfish (farmed)
42
109
151
Cod
3
131
134
Mahi-Mahi (dolphin fish)
22
96
118
Tilapia
4
111
115
Brain size remains reasonably constant from 100,000 to 10,000 years ago, then starts to shrink, perhaps coinciding with the birth of agriculture and diets based more on meat, milk and plants than marine foods. Today, average brain size is 1.35kg.
The evolution of intelligence and self-awareness
Apart from brain size and, more pertinently, brain to body size ratio, what sets us apart from other animals is self-awareness. Animals have the equivalent of thoughts and feelings but humans are relatively unique in being able to witness one’s own thoughts and feelings, that is self- awareness. This is not an easy thing to measure, but some other mammals, notably dolphins, gorillas and chimpanzees, also have a degree of self-awareness. Other contenders for higher cognition include octopuses and elephants, all large brained creatures. However, it isn’t just size that counts. In essence, there are three evolutions of the brain. First, the reptilian brain located on the brain stem, which programmes basic survival needs. Then there’s the mammalian brain, with more cognitive and emotive functions (think dog), then the neo-cortex, associated with higher cognition. But, while elephants have larger brains they have smaller neo-cortexes. It’s the neo-cortex that starts to grow in our hominid ancestors.
An indication of an advancing intelligence could be supposed from the earliest evidence of ancient rock art, as well as use of complex tools and adornments. The earliest rock art is found in South Africa, dating back 77,000 years ago, and in Western Europe about 37,000 years ago, and possibly in Australasia (Sulawesi) around that time.
The richest concentration of ancient rock art over 6,000 years ago, however, is found in sub-Saharan Africa, the Nile Valley and Red Sea hills, then a green belt with vast lakes, rivers and wetlands, hence abundant marine foods, which lasted until about 3,500 years ago when much of Egypt is becoming a desert. Whether the drying up of the Sahara was linked to the Younger Dryas (see below), a change in the Earth’s tilt or over grazing is a subject of debate.[i]
Meanwhile, groups of our early ancestors who had left Africa, living in Europe as far west as Ireland, north as Scandinavia, East as China and Australia, were also struck by cataclysmic weather changes. In Europe the Magdalenian culture, with advanced stonework, exists from 17,000 years ago, coinciding with the end of the Ice Age, until 12,000 years ago, coinciding with the Younger Dryas, a period of extreme cooling which lasted for circa 1,000 years, possibly triggered by a meteor shower[i]. One theory has ancestors migrating south, towards warmer climates with available water, possibly carrying with them the sticky grains they had previously gathered, and may have planted them in moist soil as a means to survive, thus giving birth to the agricultural age whereby mankind moves away from a hunter gatherer lifestyle towards an agricultural lifestyle. This also makes sense as these two pockets of humanity, in Mesopotamia (now Iraq), between the Tigris and Euphrates river, and Egypt, becoming more densely populated with the need for stored food, supplied by grains and domesticating animals. This stable food supply would have allowed expansion of these populations. (There is another evolutionary hotspot in Asia and China[i].)
Early Enlightenment
The likely existence of an ‘enlightened’ culture, Atlantis, is eluded to in the writings of Plato, possibly existing around the fertile region of the then much smaller Black Sea, which is thought to have flooded across the Bosphorus peninsular when the Mediterranean sea levels rose to a critical mass, dated back to around 7,000 years ago. This may also be the origin of the Flood myth, which occurs in ancient Sumerian lore dating back 5,000 years and later Hebrew lore.
Thus we have this triangle between the Black Sea to the North, Egypt to the South, and Mesopotamia to the East, all with evidence of evolved culture, including monotheism. The Sumerian culture appears over 6,000 years ago in the fertile crescent of Mesopotamia. Later, circa 2,500 years ago, we have the enlightened Zoroastra in Mesopotamia forming the Parsi culture in what is now Iran. Also,The Aryan-(Dru)Vedic culture, sometimes located east of the Black sea, migrated into the Indus valley in northern India as the main influence of the now Hindu culture, and the start of the Greek culture, considered to be the origin of our Western culture. The earliest hint of a Druidic culture dates back to this time. One stream of ancient druidic lore talks of a cataclysmic event, stones pouring from the sky, raising the possibility that early stone structures and barrows were built effectively as ‘bomb shelters’.[i] While the meaning of the word ‘dru’ is associated with oak (those who meet by the oak) and truth, it also may also mean worshippers of the red Sun (du rua). Sun and fire worship is shared by the early Egyptians (Ra), (dru)vedic culture (Agni and Surya), Zoroastrian culture(Mithra) and even Sumerian culture (Utu). The use of fire started much earlier, with it’s discovery a million years ago, and widespread use from 500,000 years ago, which expanded humanity’s ability to derive energy from previously indigestible carbohydrates, as evidenced in the DNA with the emergence of multiple variations in carbohydrate- digesting amylase enzymes. This is also linked to an expansion in brain size.[ii]
Is Homo Sapiens devolving?
Globally, there is an increase in mental illness which is fast becoming the biggest health threat, according to the World Health Organisation. There is also evidence that our brain size has reduced by 10 per cent, from 1.45kg 10,000 years ago[1] to an average now of 1.35kg, coinciding with a more land-based food supply. According to Scandinavian research, our IQ is also falling by 7 per cent a generation. Global rates of depression and dementia, suicide and stress-related disorders of anxiety and insomnia are escalating. One in six children in the UK are classified with ‘special educational needs’ (SEN). Suicide, globally, has become the most cause of violent deaths, ahead of all wars and murders. In the UK 790 people a day, nine double decker buses worth, are diagnosed with dementia. Global incidence will top 100 million this decade, already costing over 1% of GDP.
On the assumption that our brains still require at least the same supply of nutrients that our semi-aquatic ancestors were able to eat during the period of maximum brain evolution – although one could argue that the digital age has put more stress on our brain function, hence we might even need more nutrients – and the fact that we are simply not achieving anything like the same intake of the brain’s essential fats, phospholipids and micronutrients, is it any wonder that mental health is in sharp decline? With a growing population and declining available seafood, coupled with contamination with heavy metals, PCBs and micro-plastic particles, matters are likely to get much worse.
High sugar intake, in animals, has been shown to lead to shrinking of the brain’s hippocampal region. This is where the nucleus accumbens, the seat of the brain’s dopamine-based ‘reward’ system, stimulated by sugar, caffeine and tech addiction, (especially that based on variable rewards such as the ‘like’ button) resides. Marketeers have learnt how to create addiction to their products by stimulating the reward system, selling short-term pleasure, the dopamine-based feeling, in the guise of happiness. The happy hour, the happy meal, happiness in a bottle etc. Over-stimulation of the reward system ultimately leads to dopamine depletion and brain cell death, coupled with a decline in serotonin, the tryptamine associated with happiness, connection, love, empathy and other essential qualities of a harmonious society – and the very qualities that make us human.
We are therefore witnessing the devolution of the brain, the decline and fall of mental health and harmonious society, a situation that is likely to get worse as population expands, unless we rapidly find a way to optimally nourish the brain.
Building Healthy Brains
The emphasis in human nutrition has, for too long, been on the body. With more protein, meat and dairy products, we have grown taller, but not smarter. As director of the Institute of Brain Chemistry at the Chelsea and Westminster Hospital, Professor Michael Crawford has been able to accurate predict which pregnant women are most likely to have pre-term babies, with an increased risk of cognitive delay or impairment. This is based on determining the supply, by analysing the pregnant woman’s blood, of DHA. In its absence levels of a surrogate fat, oleic acid, rises to fulfil the requirement of the neonatal brain, when DHA is in short supply. It is, however, an inadequate substitute and thus cognitive development is impaired. Babies born of mothers with low blood DHA levels, compared to those supplementing DHA, have smaller brains.[2]
According to Crawford, with a growing population and shrinking fish supply, we must develop marine agriculture on a massive scale to survive and protect the brain. In the same way that man moved from hunter gatherer on the land to peasant farmer, we too must move from hunter gatherer in the oceans to marine farmer. In Japan he has been instrumental to the creation of artificial reefs in the estuaries to attract back the marine food web, from mussels to crustaceans, and fish, as well as farming seaweed on a massive scale. By processing seaweed it is possible to create DHA, the critical brain fat that is crucially lacking in a plant-based diet. As Crawford says “We now face a world in which sources of DHA – our fish stocks – are threatened. That has crucial consequences for our species. Without plentiful DHA, we face a future of increased mental illness and intellectual deterioration. We need to face up to that urgently.”
At the other end of the lifecycle, more and more older people are slipping into dementia, which is a preventable but not reversible condition. At the University of Oxford, Professor David Smith has shown that inadequate omega-3 fats (DHA and EPA) and B vitamins, especially vitamin B12, are the principle drivers of cognitive decline. Yet, by providing these nutrients to those with pre-dementia, further memory decline and brain shrinkage can be arrested. B12 is only found in animal foods and is especially rich in seafood. A plant-based diet alone does not provide sufficient DHA, B12 or phospholipids require for optimal brain development.
Therefore, it is vital that the needs for optimal brain function are put at the top of the health agenda to prevent the decline of our mental health and potentially the fall of Homo Sapiens. Without our fully functioning brains humanity will neither have the insight nor cooperation to face and resolve the challenges we face with a growing population, reducing food supply, increasing pollution, climate changes and ever-increasing energy demands.
Food for the Brain is a non-for-profit educational and research charity that offers a freeCognitive Function Testand assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing theCognitive Function Testyou are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices.
This study explored stress & food preferences. 232 Flemish students completed a food frequency questionnaire and psychological tests to measure stress levels, during exam period, to determine effects of stress on food choices as part of a longitudinal study.
Results
Diet quality of the students was observed to deteriorate during the exam period in response to stress, with preferences for high fat and sugar foods increased. The study indicated that chronic stress alters food preferences to high fat and high sugar foods. However, the data was from food frequency questionnaires and self reported measures of stress levels. These methods are vulnerable to self reporting biases. Further research which monitors diet whilst taking serum samples of cortisol and other stress-related markers are required to explore these findings further.
Michels, N., Man, T., Vinck, B., & Verbeyst, L. (2020). Dietary changes and its psychosocial moderators during the university examination period. European journal of nutrition, 59(1), 273–286.
This study investigate bilingualism & cognition. The study was a meta analysis of studies. Inclusion criteria was studies investigating bilingualism in the elderly with relation to Alzheimer’s disease risk. 6 prospective cohort studies were selected and 8 retrospective studies were selected. Of the 14 studies, only 2 had a monolingual control group. 14 studies selected for analysis. Study indicated that bilingualism may be protective against memory decline in older adults.
Results:
Meta analysis indicates that one exception, the studies support the idea that bilingualism reduces risk of memory decline. . However, only a small sample of studies included, although selected studies generally of a good sample size (>500). Only two of the studies included participants with Alzheimer’s disease diagnosis. Moreover, only two studies had a control group. Further, two of the studies included only Hispanic subjects, which may have impacted results.
A notable limitation of the meta analysis is that it did not include any statistical analysis methods (i.e p value) and this is a significant limitation. Further large scale research is required to explore effects of bilingualism on cognition, and whether bilingualism may be protective against cognitive decline.
This study investigated bilingualism & cognition. Study included 28 older adult participants – 14 monolingual participants and 14 bilingual participants (who had been bilingual since before age 11). All participants were subjected to a fMRI and had no diagnosed mental health conditions.
Results indicated:
Bilingual participants performed better on tasks and had better working memory (p<0.01) and better connectivity (p=0.002), compared with the monolingual group (p=0.17)
Results observed for other types of memory were not significant
Study size was small. Further large scale warranted. Study did not specify regarding bilingualism, as to whether participants spoke more than 2 languages, or whether certain type and complexity of language afford greater protection (i.e romance languages, Germanic languages etc.). Further research merited to explore effects of bilingualism on other types of memory.
Grady, C. L., Luk, G., Craik, F. I., and Bialystok, E. (2015). Brain network activity in monolingual and bilingual older adults. Neuropsychologia 66, 170–181. doi: 10.1016/j.neuropsychologia.2014.10.042
In this study memory change over 6 years was assessed using a large scale sample (16, 638 elderly individuals born <1948) from Health and Retirement Study. Growth curve models were analysed with reference to memory recall of a 10 word list and levels of social integration (i.e with family, volunteering, marital status).
Results indicated:
Socialisation demonstrated as a predictor of slower memory decline (p<.01).
In individuals with vascular disease, socialisation observed to be protective buffer ( (p< 0.05)
Memory amongst least socialised deteriorated at twice the rate of other participants, with association greatest amongst those with <12 years of education (p<0.07)
The study indicates that socialisation and levels of education may be protective factors for memory decline. The study also suggests that socialisation may reduce risk for memory decline in individuals with vascular diseases. The study did not use a robust means of measuring memory capability, such as MMSE. Results for socialisation as a predictor of slower memory decline not statistically significant. However, socialisation in individuals with vascular disease as a protective factor was observed to be statistically significant. More research required as to the mechanisms of how socialisation reduces risk of memory decline in vascular disease. Findings for education as a protective factor were observed to be statistically significant. More research required into to what level of education is most protective against memory decline.
Ertel, K. A., Glymour, M. M., & Berkman, L. F. (2008). Effects of social integration on preserving memory function in a nationally representative US elderly population. American journal of public health, 98(7), 1215–1220.
This study explored fasting & cognitive performance. It identified that biological ageing is a process which is accelerated and exacerbated by excessive calories and a sedentary lifestyle. Further, these factors combined may increase the risk of developing neurodegenerative diseases. This systematic review explored the role of different types of IF (intermittent fasting) on cognitive function, with specific focus on BDNF (brain derived neurotrophic factor) as a marker. Reduction of levels of BDNF has been associated with cognitive decline and increased risk of Alzheimer’s disease. Moreover, reductions in BDNF may result in a reduction in synaptic plasticity, memory and learning.
The study accepted and appraised 82 papers. Key findings were:
IF modulated BDNF supporting synaptic maturation and function
Primary evidence demonstrates pro-cognitive and neuroprotective effects of IF and BDNF
Sex specific differences were observed in response to IF
IF was suggested to be supportive for brain health and sustaining cognitive performance into old age, although it was identified further research is required into this area
Seidler, K., & Barrow, M. (2021). Intermittent fasting and cognitive performance – Targeting BDNF as potential strategy to optimise brain health. Frontiers in neuroendocrinology, 65, 100971. Advance online publication. https://doi.org/10.1016/j.yfrne.2021.100971
A sample of 2,034 individuals (age >55) in Singapore were studied to explore the link between fish consumption and depression. The study was conducted as part of the Singapore Longitudinal Aging Studies (SLAS) project and results were adjusted for all other possible factors such as smoking, exercise, diabetes etc.
Individuals consuming fish three times per week were observed to report lower depressive symptoms, compared with those who did not consume fish.
Wu D., Feng L., Gao Q., Li J.L., Rajendran K.S., Wong J.C., Kua E.H., Ng T.P. Association between fish intake and depressive symptoms among community-living older Chinese adults in Singapore: A cross-sectional study. J. Nutr. Health Aging. 2016;20:404–407.exercise, diabetes etc
This study looked at the correlation between nutritional status of older adults and health. Correlation was observed between quality of nutritional status and depressive symptoms. Elderly individuals who perceived that they had poorer health, were also observed to be at higher risk of depression.
Jung, S. E., Bishop, A. J., Kim, M., Hermann, J., Kim, G., & Lawrence, J. (2017). Nutritional Status of Rural Older Adults Is Linked to Physical and Emotional Health. Journal of the Academy of Nutrition and Dietetics, 117(6)
Results suggest that higher adherence to the Mediterranean, DASH, or MIND diets is associated with less cognitive decline ans well as a lower risk of Alzheimer’s Disease (AD). Evidence for an association with dementia was inconsistent.
The MIND diet may be more protective against cognitive decline and AD than the Mediterranean and DASH diets, based on observational studies. However, more evidence on the MIND diet is required to draw a firm conclusion. Furthermore, the Mediterranean diet seems more protective against AD than the DASH diet.
Based on the studies included in the review, olive oil consumption seems to be an important component underlying these associations.
The Mediterranean, Dietary Approaches to Stop Hypertension (DASH), and Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diets Are Associated with Less Cognitive Decline and a Lower Risk of Alzheimer’s Disease – A Review. van den Brink, A.C., Brouwer-Brolsma, E.M., Berendsen, A.A.M. et al. (2019). Advanced Nutrition.10(6), pp1040-1065