Dr Tommy Wood: Why Brain Health Needs a Systems-Based Approach
Dr Tommy Wood brain health research shows that we now know more than ever about protecting the brain, yet many people still feel overwhelmed by disconnected advice.
A headline about blood sugar here. A podcast on omega-3 there. A post about sleep, a study on exercise, a warning about stress.
Useful, yes. But also fragmented.
What Dr Tommy Wood brain health research offers is something more valuable than another isolated tip. He brings a framework.
As Head of Research at Food for the Brain, Associate Professor of Pediatrics and Neuroscience at the University of Washington, and author of the forthcoming book The Stimulated Mind, Tommy brings something rare to this field. He helps connect the dots. His work focuses on how brain health is shaped across the lifespan and why protecting cognitive function means thinking in systems, not silos.
Dr Tommy Wood Brain Health Framework
One of the reasons brain health can feel confusing is that it is often presented as a list: A long list of risk factors. Nutrients to take, habits to adopt, or a long list of things to avoid.
But the brain does not work like a checklist: it works as a living, dynamic system. It responds to what it is supplied with, how it is used, and whether it has the conditions it needs to recover and adapt.
That is the core idea behind a systems-based approach to brain health.
Instead of asking “What is the one thing that protects the brain?”, it asks three bigger questions:
Does the brain receive enough oxygen, nutrients and stable energy to function well?
How well is it being stimulated to stay active, adaptable and resilient?
Are the foundations for repair and recovery in place, such as good sleep, stress regulation and metabolic health?
When you look at brain health this way, something important changes.
Many people understandably hope for a “magic bullet”. One supplement. One diet. One breakthrough drug that protects the brain.
But science tells a different (more hopeful) story. Cognitive resilience is shaped by the interaction between many systems in the body. Blood flow, nutrient status, sleep, movement, learning, stress and social connection all influence how the brain functions and adapts.
The encouraging part is that this gives us many entry points for change. You do not have to get everything perfect, and small improvements across several areas can work together to create meaningful protection for the brain over time.
That is why a systems-based approach is not more complicated. In practice, it is far more empowering.
Why this matters for prevention?
One of the most important insights in Tommy’s work is that cognitive decline does not happen in isolation.
The brain changes in response to how we live. Blood flow, nutrient status, movement, learning, sleep, stress and social connection all shape how the brain ages and how resilient it remains.
This is also why Tommy’s forthcoming book, The Stimulated Mind, focuses on the interaction between stimulation, sleep and nutrient supply as key drivers of lifelong brain health.
This perspective is closely aligned with the mission of Food for the Brain. For years we have been communicating that dementia risk is not fixed. By understanding and addressing modifiable factors across the lifespan, it is possible to protect your mind and keep the brain healthier for longer.
Tommy’s leadership as Head of Research helps bring greater scientific clarity to this systems-based approach to prevention.
Watch: A systems-based approach to cognitive function
If you want to hear Tommy explain this approach in more depth, his lecture from the Upgrade Your Brain Conference is one of the clearest introductions we have shared.
Watch the lecture below.
What Tommy offers is not another list of things to do. It is a framework. A way to understand why so many different factors matter and how they fit together.
Learn More About Dr Tommy Wood Brain Health Research
If this approach resonates with you, Tommy will be going deeper in our upcoming webinar, How to Keep Your Brain Young.
In this session he will explore the science of cognitive resilience and share practical ways to stimulate the brain, support long-term brain health and reduce lifetime dementia risk.
Food for the Brain will host the webinar on 19th March 2026 at 6 pm GMT.
Tommy’s new book, The Stimulated Mind, is also available to pre-order now. In it, he explores how the brain develops, adapts, and stays resilient across the lifespan, and why everyday factors such as movement, learning, sleep, nutrition, and social connection play such an important role in shaping long-term brain health.
Pre-order your copy today before the book releases on 26th March 2026.
Final thought
For many people, the challenge with brain health is not a lack of information. It is knowing where to start.
When advice comes as scattered tips, nutrients, tests, and lifestyle changes, it can feel difficult to turn good science into clear action.
What Tommy’s work offers is a framework: a way of understanding how the different pieces of brain health fit together and why small changes across several areas can have a powerful cumulative effect.
At Food for the Brain, this systems-based approach sits at the heart of COGNITION, our brain upgrade programme.
COGNITION helps you understand your personal risk factors, learn the most important steps to protect your brain, and put them into practice with guidance and support.
The programme has recently been upgraded and is now available globally for just £5 per month or £50 a year, making it accessible to anyone who wants to take their brain health seriously.
If Tommy’s lecture resonates with you, COGNITION is the natural next step.
Because protecting your brain is not about doing everything perfectly.
It is about understanding the system and taking the next right step.
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
The Biggest Myths About Alzheimer’s – And What the Science Actually Shows
Alzheimer’s disease is one of the most feared diagnosis of modern life. And where there is fear, myths flourish. Many of the biggest myths about Alzheimer’s have become widely accepted beliefs. We are told it is purely genetic, that it is an inevitable part of ageing, and that the main hope lies in new drugs targeting amyloid in the brain.
The science tells a far more complex and, importantly, far more hopeful story.
Myth #1 in the biggest myths about Alzheimer’s: ‘It’s all in your genes’
When Alzheimer’s runs in families, it is natural to assume destiny is fixed. Both your grandmothers had it, so you assume you will too.
Yet fewer than 1% of cases are caused by rare deterministic mutations in APP, PSEN1 or PSEN2 genes that lead to early-onset familial Alzheimer’s disease [1].
The vast majority of Alzheimer’s cases are late-onset and multifactorial. That means risk is shaped by multiple influences across a lifetime.
What about APOE4?
Celebrities like Chris Hemsworth have put the APOE4 gene on the map and into the public sphere and it is the strongest common genetic risk factor for late-onset Alzheimer’s. Having one copy increases risk; two copies increase it further [2]. But it does not determine outcome, as many APOE4 carriers never develop dementia. Many people with Alzheimer’s do not carry APOE4.
Genes influence vulnerability but they do not dictate your future.
APOE4 affects lipid transport, inflammatory signalling and neuronal repair. These processes are influenced by metabolic health, vascular function, nutrient status, sleep, stress physiology and lifestyle.
One of the most important things to remember is that gene expression is not static, as genes respond to the environment they are in.
The most important question is not necessarily ‘How do I check my genes?’ The question is ‘What environment are your genes operating in?’ Because you cannot change your genes but you can influence how they function and are expressed.
Myth #2 in the biggest myths about Alzheimer’s: ‘Nothing can be done’
This is the most damaging myth of all.
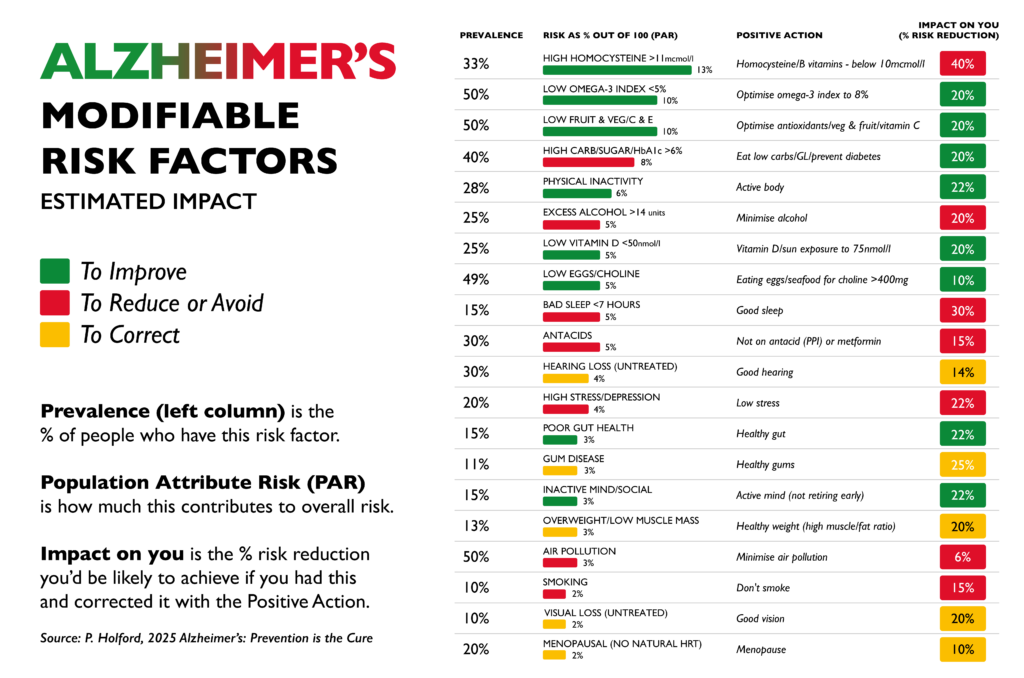
The 2020 Lancet Commission concluded that around 40% of dementia cases worldwide are attributable to modifiable risk factors [3]. The 2024 update increased that estimate to approximately 45% [4].
Nearly half of all cases.
And this is mainstream consensus. (Read more about the Alzheimer’s Prevention Expert Group’s APEG response to this recent Lancet report here).
The identified risk factors include hypertension, diabetes, obesity, physical inactivity, smoking, depression, hearing loss and social isolation. Importantly, Alzheimer’s risk is not fixed, it develops gradually over decades.
However, many researchers (ourselves included) believe even 45% may underestimate the true preventable proportion.
A large UK Biobank analysis published in the journal Nature Human Behaviour modelled a broader range of modifiable factors and estimated that up to around 73% of dementia cases could be attributable to modifiable influences [8]. Professor David Smith of Oxford University, co-author of that study, member of our Scientific Advisory Board, and lead investigator of the VITACOG trial, has suggested this may still be conservative, as certain blood biomarkers were not included in the modelling.
Whether the true figure is closer to 45% or 73%, the direction of evidence is consistent.
A large proportion of dementia and Alzheimer’s is preventable and you can modify your risk with simple changes.
Why biology supports prevention
Alzheimer’s develops through interacting processes such as impaired glucose metabolism, vascular dysfunction, inflammation and elevated homocysteine.
In the VITACOG trial, homocysteine-lowering B vitamins significantly slowed whole-brain atrophy in people with mild cognitive impairment [6]. The benefit was strongest in those with adequate omega-3 status [7].
That is structural brain change.
(When compared to anti-amyloid drug trials, which show modest slowing of decline in already symptomatic patients, VITACOG demonstrated slowing of brain shrinkage itself in an at-risk group.)
Once significant neuronal loss has occurred, reversal is unlikely, but years before diagnosis, measurable risk is accumulating and that is where prevention has its power.
Myth #3 in the biggest myths about Alzheimer’s: ‘It has a single cause‘
The reductionist model searches for one target and one solution.
Alzheimer’s reflects the interaction of multiple biological systems:
Glucose regulation
Vascular health
Lipid transport
Inflammation
Oxidative stress
Methylation
Sleep and stress regulation
Hormonal balance
People arrive at cognitive decline through different combinations of biological drivers. For some, insulin resistance may be central. For others, vascular stiffness and hypertension. In others, chronic inflammation and elevated homocysteine may play a key role. The destination may look similar, but the route is not.
This systems view explains why targeting one downstream marker, such as amyloid, yields modest slowing. Correcting multiple upstream drivers is biologically more plausible for meaningful long-term risk reduction.
Watch the video below to learn how Food for the Brain uses a systems-based approach.
Myth #4 in the biggest myths about Alzheimer’s: ‘It’s inevitable with ageing’
Age increases risk. However, that is only part of the story.
There are many individuals in their 80s and 90s with preserved cognition. The difference often lies in lifelong vascular, metabolic and lifestyle patterns, also known as patterns for prevention.
It is clear from what you have read so far that this is not an inevitable part of getting older. With the right knowledge and habits, it is something most people can avoid.
And that is why Food for the Brain exists, because not enough people know this and not enough people know what action they need to take to protect their brain.
A More Accurate Framework
Ageing is not the enemy. It is a privilege denied to many.
The goal is not to avoid growing older. It is to protect the brain as we do.
Alzheimer’s is not a single event. It reflects decades of interacting biological stress: metabolic strain, vascular change, inflammation and nutrient imbalance. These processes build slowly and often silently.
By the time symptoms appear, significant damage has already occurred.
The science is clear that a substantial proportion of dementia risk is modifiable [6,10]. That does not mean guarantees. It means opportunity.
You cannot change your genes and you cannot stop the passage of time.
Yet, you can influence how your brain responds to both.
Our six-month brain upgrade programme provides structured guidance, accountability and expert support to help you translate knowledge into meaningful and lasting change.
Prevention is possible. It begins with measurement, and it progresses with action.
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
Why do women make up nearly two thirds of those diagnosed with Alzheimer’s?
The answer may start long before symptoms appear, in the decade when hormones begin to change. The years before and after menopause mark one of the most significant neurological transitions of a woman’s life – a pivotal period for female brain health.
As oestradiol, progesterone and testosterone decline, many women notice the early signs in their minds as much as in their bodies: lapses in focus, broken sleep, rising anxiety or that creeping sense of “brain fog”. Research now shows this is not coincidence. The same hormones that shape reproduction also shape the brain.
The Brain’s Own Hormones
Oestradiol, the most biologically active form of oestrogen, is produced mainly in the ovaries but is also synthesised within the brain itself (1). Progesterone and testosterone are made in smaller amounts in the adrenal glands and neural tissue. Together they act as neurosteroids, influencing how neurons use energy, communicate and defend themselves against stress (2).
Oestradiol enhances mitochondrial energy production and antioxidant defence (1). Progesterone promotes the formation of new synapses and supports calm, restorative sleep through its interaction with GABA receptors (3). Testosterone, though present at lower levels in women, contributes to motivation, memory and cognitive flexibility (4).
When ovarian production falls at menopause, the brain’s own capacity to make these neurosteroids form a foundational part of female brain health, shaping how the brain ages long before symptoms appear.
When Hormones Fall: The Brain’s Energy Shift
Brain imaging studies show menopause triggers a measurable shift in how the brain uses fuel. Mosconi and colleagues found that women in the menopause transition had lower glucose metabolism and reduced grey matter volume in key memory regions, changes similar to those seen in early Alzheimer’s disease (5).
Ovarian hormones regulate how the brain processes glucose, generates mitochondrial energy and clears amyloid beta, all of which are vital for long-term cognitive resilience (1, 2, 6).
Early Hormone Loss and Its Impact on Female Brain Health
Women who experience early menopause before 45 or oophorectomy (surgical removal of ovaries) have a significantly higher lifetime risk of dementia. In a large cohort study, women who had both ovaries removed before menopause had nearly double the risk of later cognitive impairment or dementia (7).
This appears linked to the duration of hormone deprivation. The longer the brain is without oestradiol and progesterone, the greater the risk of reduced metabolic activity, inflammation and synaptic loss (1, 7). Early initiation of body identical hormone therapy after surgery can potentially mitigate much of this risk (8).
Hormone Therapy and the Critical Window
Evidence now supports a critical window. Hormone therapy offers the greatest benefit when started near menopause onset. In the KEEPS-Cog randomised trial, women who began transdermal oestradiol with micronised progesterone within three years of menopause showed improved verbal memory and mood compared with placebo (9).
Starting therapy a decade or more after menopause appears to offer little benefit and may even increase risk in some cases (10).
Neuroimaging data from the UK Biobank support this pattern. Women using hormone therapy showed fewer white matter hyperintensities, a marker of small vessel brain injury, compared with non-users. The effect was strongest among early starters and long-term users. Late initiation offered minimal or no protection (11).
Nutrition and Biomarkers That Interact With Hormones
Even with optimal hormone therapy, brain health depends on metabolic balance and nutrients. Several nutrient-linked biomarkers have independent and synergistic effects on cognition and are essential pillars of female brain health:
Homocysteine. Elevated levels double dementia risk. Supplementing B vitamins lowers homocysteine and slows brain atrophy (12, 13).
Omega-3 Index. Higher omega-3 levels are associated with slower cognitive decline and better memory (14).
Vitamin D. Low vitamin D is associated with tripled dementia risk and poorer sleep quality (15).
HbA1c. Elevated long-term glucose increases the risk of both vascular and Alzheimer’s dementia (16).
Want to know what your levels are? Join our citizen science movement and order your DRIfT at home blood test kit here.
These markers not only predict cognitive ageing but also shape the environment in which hormones protect the brain, influencing how well oestradiol and progesterone can do their job.
Sleep and Its Role in Female Brain Health
Sleep is the brain’s repair cycle. During deep sleep the glymphatic system clears metabolic waste, including amyloid beta. Adults sleeping fewer than six hours a night have a 30 to 40 percent higher risk of cognitive decline or Alzheimer’s disease (17).
Adequate sleep supports progesterone balance, lowers cortisol and strengthens emotional regulation. It is a natural complement to both hormonal and nutritional support. (Read our recent sleep series here and here for more info.)
Key Takeaways
Oestradiol, progesterone and testosterone act as neurosteroids produced in both the ovaries and the brain, directly influencing mood, metabolism and memory.
Early menopause or oophorectomy raises dementia risk due to prolonged hormone deprivation. Early, body-identical hormone replacement may mitigate this.
Hormone therapy timing matters. Benefits are strongest when started soon after menopause.
Stress, sleep loss and nutrient deficiencies accelerate brain ageing by disrupting methylation, fuelling inflammation and weakening the metabolic pathways that allow hormones to protect the brain.
Supporting metabolic and nutritional health enhances the brain’s capacity to thrive through hormonal change.
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
References:
Brinton RD. Estrogen regulation of glucose metabolism and mitochondrial function. Prog Brain Res. 2010;182:121-43.
This night-time molecule is also one of the brain’s most powerful protectors – your night-time antioxidant – working while you rest, to defend neurons, restore energy and preserve clear thinking. Melatonin helps your brain clean up daily oxidative damage, regulate mood, and protect memory networks from ageing.
When levels drop – through stress, light exposure, age or caffeine – you don’t just lose sleep; you lose part of your brain’s natural repair system.
The Brain’s Nightly Repair Shift
Every night, while you rest, your brain goes to work. Waste is cleared away, cells are repaired, and antioxidants are replenished.
At the heart of this clean-up crew is melatonin, made in the pineal gland and the master conductor of your brain’s nocturnal activity.
It doesn’t just promote sleep; it powers the production of glutathione, the body and brain’s chief antioxidant and cellular shield. When melatonin levels fall, oxidative stress rises – accelerating neuronal ageing and the build-up of damaging amyloid and tau proteins (1, 2). Why? Melatonin normally switches on the brain’s own antioxidant defences, recycling glutathione and neutralising free radicals inside mitochondria. Without enough melatonin, these reactive molecules (like amyloid and tau proteins) accumulate, inflaming brain tissue and allowing toxic proteins to clump together.
In studies (2), restoring melatonin reduced oxidative damage and slowed amyloid formation – a reminder that good sleep truly is brain repair in action.
Here’s the catch: melatonin only comes out when it’s dark.
Even modest evening light – the glow of your phone, TV, bedside lamp or standby light – can switch off its release (7).
That’s because the light-sensitive cells in your eyes, send a “daytime” signal to the brain’s master clock in the suprachiasmatic nucleus (a tiny region in the hypothalamus that controls your body’s sleep-wake rhythm) instantly halting melatonin production.
In clinical studies, exposure to ordinary indoor light before bedtime suppressed melatonin by up to 85 per cent and shortened its duration by several hours (7).
That’s why your late-night scroll or TV binge can leave you foggy and flat the next morning.
To support melatonin, you want to create a dark place to sleep. No lights on, heavy curtains, no street lamps. Using eye masks and utilising blue-light blocking glasses, software or filters can also be helpful if you know you are going to be on screens in the evening. You can even get special bulbs for bedside lamps or special lighting solutions for the bathroom for nighttime toilet trips.
Light is a powerful data input into the brain – so be mindful and protect yourself where practical and possible.
Age, Stress And Hormones Flatten The Rhythm
As time goes by, your natural melatonin rhythm starts to fade – by mid-life, your night-time levels can fall by half (3).
It’s one of many reasons why people can start waking up at night, struggle to drift off, or feel less refreshed after sleep.
For women, the hormonal rollercoaster of perimenopause makes things even trickier: falling oestrogen and progesterone throw the body clock off balance, making deep sleep harder just when the brain needs it most (5). (Learn more about how to support women’s hormones and brain health here.)
Melatonin levels don’t just impact sleep; studies show that lower melatonin is linked with poorer memory, mood dips and faster cognitive ageing (4). While melatonin is impacted by ageing, the good news is that it can be supported and restored.
Coffee vs. Melatonin – When Caffeine Steals Your Sleep Hormone
Caffeine doesn’t just keep you awake – it directly interferes with melatonin’s nightly rise. Even a single espresso six hours before bed can delay melatonin release by up to 40 minutes and reduce total melatonin production by as much as 20% (9). (And don’t forget black and green tea and most energy drinks contain caffeine too.)
That’s because caffeine blocks adenosine receptors – the same system that tells the pineal gland it’s time for darkness and rest. When that signal is muted, the body’s internal clock (the suprachiasmatic nucleus) misreads the time and keeps you in ‘day-mode’ far longer than intended.
Avoid coffee (and other caffeine sources) after 12 p.m., especially if you have sleep or mood issues.
Choose herbal or decaf alternatives after lunch. If you’re sensitive, even morning caffeine can blunt night-time melatonin, so experiment with caffeine-free days and observe your sleep quality.
Melatonin and Mitochondria: Your Inner Night-Time Antioxidant Factory
Here’s where melatonin gets even more fascinating. It isn’t just released from the pineal gland at night, your brain cells actually produce it inside their mitochondria, the tiny engines that create energy (ATP) and power every thought and memory (8).
This is clever biology: the very place where energy is made – and where most oxidative stress occurs – also makes its own night-time antioxidant. Melatonin acts locally in the cell, mopping up the free radicals created as mitochondria burn fuel through the day, keeping these fragile energy factories running smoothly (1).
It doesn’t function only as a sleep hormone, made only in the pineal gland – it’s also made throughout your brain (and body’s) energy-producing mitochondria, where it acts as a built-in night-time antioxidant to protect them from damage.
This local production is what keeps your neurons energised and resilient – and why good, deep sleep is essential for restoring brain power and mental clarity. (And why disrupted or shallow sleep can leave you foggy the next morning!)Want more insight into how to support your brain through quality sleep? Join our next live webinar with our expert Sleep Scientist here.
How To Restore Your Natural Rhythm
While short-term melatonin supplements (0.5–3 mg) can improve sleep onset and quality in older adults (6) and can be bought in North America or prescribed in the UK, the goal is to rebuild the body’s own rhythm:
Dark evenings, bright mornings – dim lights, avoid screens, use blue-light blocking technology, glasses and filters an hour before bed; get natural light soon after waking.
Avoid caffeine after 12 pm or if sleep is a real struggle – remove altogether, and see how it impacts your sleep.
Tryptophan-rich foods – turkey, oats, eggs and sunflower seeds support serotonin-to-melatonin conversion (with B6 and magnesium).
Keep bedrooms cool and quiet – a small temperature drop signals melatonin release.
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
Reference:
Reiter RJ et al. Melatonin as an antioxidant: under promises but over delivers. J Pineal Res. 2016;61(3):253–78.
Cardinali DP et al. Melatonin reduces oxidative damage and amyloid pathology in Alzheimer transgenic mice. J Pineal Res. 2013;55(4):427–37.
Waldhauser F et al. Age-related changes in melatonin levels. J Clin Endocrinol Metab. 1988;66(3):648–52.
Wu YH et al. Sleep, melatonin and the aging brain. J Pineal Res. 2005;38(3):145–52.
Baker FC, Driver HS. Circadian rhythms, sleep and the menstrual cycle in women. Sleep Med. 2007;8(6):613–22.
Ferracioli-Oda E et al. Meta-analysis: efficacy of melatonin for primary sleep disorders. PLoS One. 2013;8(5):e63773.
Gooley JJ et al. Exposure to room light before bedtime suppresses melatonin onset and shortens its duration. J Clin Endocrinol Metab. 2011;96(3):E463–72.
Suofu Y et al. Mitochondrial synthesis of melatonin enhances neuroprotection. Proc Natl Acad Sci USA. 2017;114(32):E7997–8006.
Burke TM et al. Caffeine effects on the circadian melatonin rhythm: a controlled trial. J Clin Sleep Med. 2015;11(8):893–900.
Your body is continually renewing itself by producing new cells. When it comes to protecting and enhancing your brain health, especially as you age, the quality of these new cells becomes increasingly important. A key factor in this cellular renewal process is the health of your telomeres – the protective caps at the ends of your chromosomes. A recent report has reinforced the strong link between telomere length and brain health, with shorter telomeres now recognised as early indicators of cognitive decline and increased dementia risk.
The process of making a new cell in your body starts by copying the map of how to build that cell, which is contained in a package of DNA strands, called a chromosome. The chromosome divides in two, giving a new set of instructions to the new cell. At the end of the chromosome is something called a telomere, which is a bit like the hard tip at the end of a shoelace. This becomes shorter with each cell division, until it is too short and the DNA is no longer protected. This triggers rapid ageing because cells stop dividing and, therefore, stop being replaced. Meanwhile, there is an enzyme, called telomerase, which can lengthen the telomere. The more telomerase activity, the slower the ageing process. For example, there is one bacterium called Tetrahymena thermophila, that has superactive telomerase so its telomeres never shorten – and it can live indefinitely.
Telomeres and Brain Ageing: The New Frontier
A recent report highlighted that shortened telomeres are not just markers of biological ageing, but also significant predictors of neurodegenerative diseases such as Alzheimer’s and other forms of dementia. According to the report, individuals with the shortest telomeres were at greater risk of developing age-related brain diseases, underscoring the urgency of protecting telomere integrity as part of a comprehensive dementia prevention strategy.
This aligns perfectly with our 6-month COGNITION brain upgrade programme, which targets eight nutrition and lifestyle domains known to support brain health, including sleep, stress, diet, and nutrient status – each of which has been shown to influence telomere length. In fact, many of the nutrients and behaviours proven to protect telomeres, such as vitamin D, omega-3 fatty acids, anti-inflammatory diets, and methylation support through B vitamins, are key focus areas within our COGNITION framework.
So, what does the research say about how we can lengthen our telomeres and protect our future?
Reduce your stress
Chronic stress, such as caring for someone with dementia, has been shown to reduce telomerase activity and shorten telomeres. Childhood trauma, depression, and even cynicism (1) also have a negative impact. On the other hand, practices like meditation have been shown to support longer telomeres (2).
Prioritise sleep
Quality sleep is linked to longer telomeres (3). For healthy ageing and longevity around seven hours per night appears optimal.
Get moving
Physical activity is another powerful protector of telomeres. Even individuals with PTSD who engaged in regular exercise were found to avoid the usual telomere shortening. (4)
Avoid smoking and maintain a healthy weight
Both smoking and obesity are linked to shortened telomeres.
Increase omega-3 and vitamin D
Studies show that higher intakes of omega-3 fish oils are associated with longer telomeres. A 2013 study found that DHA and EPA reduced telomere shortening (5). Other research links higher vitamin D levels with longer telomeres ( 6, 7). Both nutrients are abundant in oily fish.
Lower homocysteine levels
Homocysteine is a neurotoxic amino acid. Higher levels of B12 and folate, and lower homocysteine levels, are associated with longer telomeres (8, 9). A Singaporean study confirmed that elevated homocysteine levels predicts shorter telomeres (10).
This would seem to indicate that testing your homocysteine level is one of the smartest things you can do for your long-term brain health. That’s why we include it in our DRIFT 5-in-1 blood test here. This accurate at-home test measures five crucial biomarkers for assessing dementia risk and cognitive resilience.
Eat anti-inflammatory foods
A 2015 study found that individuals who consumed more anti-inflammatory foods had longer telomeres (11). Another study showed that greater vegetable intake is associated with longer telomeres (12). Even multivitamin use, which typically includes B12 and folate, has been linked to longer telomeres (13). (Find out advice on supplementation here).
If you want more personalised guidance on how to protect your brain – and your future health – Become a FRIEND today and get access to your personalised 6-month brain upgrade programme COGNITION®.
Join us in building a future where cognitive decline is not inevitable but preventable.
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
In 1965, UK paediatrician Dr Richard Smithells discovered that children with low folate were at significantly higher risk of neural tube defects, then commonly referred to as spina bifida.
It took more than 25 yearsfor his research to be taken seriously.
It wasn’t until the late 1980s that the Medical Research Council agreed to fund a study, the results of which were published in 1990. In 1991 the UK government told all women who were pregnant or planning pregnancy, to supplement 400 mcg of folic acid.
Folic acid reduces risk by supporting the process of methylation, which can be assessed through homocysteine levels. The process of methylation is vital for neuronal development and it depends not only on folate, but also on vitamins B6 and B12. Nine in ten obese women in the EU fail to achieve basic guidelines for folic acid supplementation in early and pre-pregnancy which would help to prevent such tragic neurodevelopmental problems (1).
—
Accelerated Brain Shrinkage & Methylation
More than half of all children, and probably their parents, are deficient in B12. Accelerated brain shrinkage occurs below 500 pg/ml, as established by Professor David Smith’s research at Oxford University more than a decade ago. This is why several countries, such as Japan, set the ‘normal’ range for serum B12 as being above 500 pg/ml. Despite clear evidence to the contrary over the past decade, both UK and US health authorities have failed to correct the wrongful reference range for vitamin B12, set at less than half this, namely 180pg/ml (2).
A recent study of 3,000 EU children reported that the median level was 347 pg/ml and one third were below 200 pg/ml (3). This means that at least half of the children had levels associated with accelerated brain atrophy. This deficiency is especially prevalent in vegan children.
Poor methylation, identified by raised homocysteine, isn’t just an established risk factor or biomarker for neural tube defects. It is also a biomarker for autism, poor cognition in children, epilepsy, congenital heart defects, reduced birth weight and size, pregnancy complications, miscarriages, bipolar disorder, depression and schizophrenia (4). Methylation is required to ‘marry’ omega-3 DHA to phospholipids such as phosphatidylcholine, to form neuronal membranes essential for brain communication. Without healthy, fully functional neuronal membranes, cognition becomes ‘disconnected’.
The Bristol Avon study of 11,875 pregnant women showed a clear relationship between the amount of seafood consumed by a pregnant woman and their child’s development. The less seafood consumed, the worse the child’s social behaviour, fine motor skills, communication, social development, and verbal IQ (5).
At the Chelsea and Westminster campus of Imperial College London, Professor Michael Crawford’s team at the Institute of Brain Chemistry and Human Nutrition, has identified which mothers are likely to have neurodevelopmentally impaired infants based on their blood level of a type of oleic acid, which is produced as a substitute when insufficient omega-3 DHA is available to build the foetal brain (6). DHA is not only critical for brain development, but also essential for optimal visual function.
Insufficient choline, a primary constituent of phospholipids, during pregnancy is strongly linked to poor cognition. Women given choline in the last trimester have infants with faster speed of processing information and memory between four and thirteen months of age (7). The protective intake, 400mg per day, has also been shown to cut the risk of cognitive decline, dementia and Alzheimer’s by about 20% (8). So, lack of folate, B12, omega-3 fats and possibly choline are all extremely common and all strongly linked to many aspects of neurodivergence, including autism.
—
How Much is ‘in the Genes’?
The culturally ‘acceptable’ view is that neurodivergence can’t be ‘treated’ – that the challenging symptoms experienced by those classified as neurodivergent or autistic (for example, cognitive and communication problems, anxiety and depression) can never be improved, despite clear evidence to the contrary. It is believed by some that autism, since it sometimes occurs within families, might be largely ‘in the genes’, as it was for Alzheimer’s. But families share environments, including habits from diet, smoking and drinking. We now know that genes cause less than one in a hundred cases of Alzheimer’s (9). Also, the gene hypothesis cannot adequately explain the dramatic rise in autism diagnoses in recent decades nor does it accept the simple fact that genes can only exert their effects across our biology – which is directly affected by nutrition.
That is not to say that genes don’t play a part in neurodivergence. There are several known genetic polymorphisms that do increase risk of neurodivergence such as a key methylation gene polymorphism, MTHFR677TT, which means that a person is less good at methylation, and needs more B vitamins. If present in the mother or child it almost doubles the risk of autism. A recent meta-analysis concludes, “For those mothers and children who are generally susceptible to autism, prenatal folate and vitamin B12 may reduce the risk that children suffer from autism.” (10) This is the same gene polymorphism that increases risk of Alzheimer’s disease.
Associate Professor Murphy’s research in Spain found that those women who had a homocysteine level above 9 mcmol/l, which is not uncommon (ideal is below 7), strongly predicted neurodivergent problems in their children at 4 months and again at 6 years of age, including an increased risk of autism, with children more likely to suffer from anxiety, depression, social problems and aggressive behaviour (11).
—
Personalised Assessment Is Needed
Neurodivergence, including conditions such as autism, is a broad and evolving concept, which currently encompasses so many children. There are many potential contributors including gut-brain problems, neuro-inflammation, nutritional deficiencies, toxic excesses, microbe infections including mould, food and other allergies, smartphone overuse, psychological and social issues, as well as genes. Every child needs a full assessment of these potential contributory factors. Individual assessment is required, with nutrition being one of the key factors to address.
As Dr Rona Tutt, OBE, past President of the National Association of Head Teachers, an expert in special needs and on the board of Trustees says:
“People come in assorted shapes and sizes with brains that are unique. A significant minority who are neurodivergent, need to be recognised, valued and supported, so they can maximise their strengths and overcome their challenges. We need to understand what is driving this increase in neurodivergence and how to best support and optimise a child’s potential.”
—
We Cannot Repeat Our Past Mistakes
Our goal in launching COGNITION for Smart Kids & Teens is to empower children and their parents to be the best they can be. Children are our future, yet the current system is already struggling, with one in six children identified as having special educational needs. We can no longer ignore the clear and growing body of evidence linking neurodivergence to widespread deficiencies in B vitamins and omega-3 fats – key drivers of impaired methylation. Addressing these foundational nutritional gaps must be the starting point for effective intervention. Ignoring or opposing this imperative is no different from what happened to Dr Smithell’s research on folic acid and neural tube defects. Initially, they said it wasn’t true and wasn’t important. Twenty five years later, to the cost of many thousands of children, it was finally recognised as both true and very important.
I hope we do not have to wait as long for the role of nutrition in neurodivergence to be taken seriously.
What we are campaigning for is widespread social awareness, along with governmental acceptance. The purpose of COGNITION for Smart Kids & Teens is to give parents a direct way to assess their children and identify simple and doable ways to help them reach their full potential for health and happiness.
Visitfoodforthebrain.org/smartkids to find out more about the campaign, which launches on April 24th with both a conference for health professionals and a public webinar for parents. This coincides with the launch of the free on-line COGNITION for Smart Kids and Teens – an assessment with personalised advice on how to help children reach their full potential.
—
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
2 https://researchbriefings.files.parliament.uk/documents/POST-PN-0612/POST-PN-0612.pdf; see also Russell G, Stapley S, Newlove-Delgado T, Salmon A, White R, Warren F, Pearson A, Ford T. Time trends in autism diagnosis over 20 years: a UK population-based cohort study. J Child Psychol Psychiatry. 2022 Jun;63(6):674-682. doi: 10.1111/jcpp.13505
5 D’Adamo C et al., Reversal of Autism Symptoms among Dizygotic Twins through a Personalized Lifestyle and Environmental Modification Approach: A Case Report and Review of the Literature. J Pers Med. 2024 Jun 15;14(6):641. doi: 10.3390/jpm14060641
6 Survey conducted in collaboration with the charity Thinking Autism. The full survey results will be shown at the Smart Kids conference, April 24th 20025.
9 Roigé-Castellví J, Murphy M, Fernández-Ballart J, Canals J. Moderately elevated preconception fasting plasma total homocysteine is a risk factor for psychological problems in childhood. Public Health Nutr. 2019 Jun;22(9):1615-1623. doi: 10.1017/S1368980018003610; see also Murphy MM, Fernandez-Ballart JD, Molloy AM, Canals J. Moderately elevated maternal homocysteine at preconception is inversely associated with cognitive performance in children 4 months and 6 years after birth. Matern Child Nutr 2017;13,e12289 . doi: 10.1111/mcn.12289
10 Hasler M, Fideli ÜS, Susi A, Hisle-Gorman E. Examining the relationship between autism spectrum disorder and neural tube defects. Congenit Anom (Kyoto). 2023 Jul;63(4):100-108. doi: 10.1111/cga.12516. Epub 2023 Apr 18. PMID: 37073427.11 Smith AD, Refsum H. Homocysteine – from disease biomarker to disease prevention. J Intern Med. 2021 Oct;290(4):826-854. doi: 10.1111/joim.13279
Neurodivergence refers to differences in mental or neurological function from what is considered typical. This concept encompasses conditions such as autism spectrum disorder (ASD), ADHD, Tourette’s syndrome, dyspraxia, synaesthesia, dyscalculia, Down syndrome, epilepsy, and chronic mental health conditions like bipolar disorder, OCD, borderline personality disorder, anxiety, and depression. The overlap of traits in ASD and ADHD has led to the term AuDHD, recognising their frequent co-occurrence [1].
The term ‘neurodiversity’ refers to the natural variations in how human brains function, emphasising that every individual is unique [2]. While some neurodivergent individuals face challenges in communication, information processing, and social integration, others exhibit remarkable creativity and intelligence. The former president of the National Association of Head Teachers, Dr Rona Tutt, highlights that neurodevelopmental disorders often co-occur, challenging outdated beliefs that conditions exist in isolation [3].
—
The Environmental Influence on Neurodivergence
While genetics may contribute to neurodivergence, environmental factors play a significant role. The rise in neurodevelopmental diagnoses cannot be solely attributed to better awareness and diagnosis . Factors such as air pollution, processed food consumption, chemical exposure, and modern technology use are increasingly considered potential contributors [3]. Many characteristics of neurodivergence appear within families, often assumed to be genetic. However, shared environmental influences—nutritional deficiencies, exposure to toxins, and psychosocial stressors—may drive this heritability rather than genes alone [3].
The increase in neurodevelopmental diagnoses is particularly striking in children. In the US, one in six children is classified as neurodivergent, and autism diagnoses have risen fourfold in two decades [1]. A practical measure of this shift is the number of children classified as having special educational needs (SEN). These classifications are often made reluctantly by parents and educators, underscoring the genuine increase in neurodivergence rather than mere overdiagnosis.
—
The Role of Nutrition in Brain Development
Nutrition plays a crucial role in cognitive development and mental health. Dr Carl Pfeiffer, a pioneering physician, identified zinc deficiency and pyroluria as biological imbalances linked to sensory overload and neurodevelopmental difficulties [4].
Nutrient deficiencies can contribute to key symptoms of ASD and ADHD. The following table is adapted from data provided by the US Centers for Disease Control and Prevention (CDC) on common ASD characteristics and their potential nutritional correlations. Research has linked the following deficiencies to common neurodivergent traits:
Omega-3 DHA, Hcy/B vitamins, dysglycemia (sugar), vitamin C
Lack of fear or more fear than expected
Omega-3 DHA, Hcy/B vitamins, dysglycemia (sugar), vitamin C
—
The Critical Window of Pregnancy and Early Childhood
The foundation of brain health is laid during pregnancy. By birth, 70% of brain cells are already formed, making prenatal and early childhood nutrition crucial [5]. Deficiencies during this period can have long-term consequences.
For example, studies have shown:
Low seafood consumption during pregnancy is linked to poorer social behaviour, fine motor skills, and verbal IQ in children [6].
Vitamin A deficiency affects brain development, leading to cognitive impairment [7].
Low maternal folate intake is associated with poorer cognitive outcomes in children [8].
Higher B-vitamin levels in infancy predict better cognitive function in adulthood [5].
Supplementing with folic acid (400mcg/day) during pregnancy improves cognitive outcomes at ages three and seven [5].
Elevated homocysteine levels during pregnancy are linked to higher risks of anxiety, depression, and social difficulties in children [9].
Optimising Brain Health Through Diet
Given the strong link between nutrition and brain function, proactive dietary changes can support neurodevelopment and alleviate symptoms of neurodivergence. Key recommendations include:
Avoid alcohol and smoking, especially during pregnancy and breastfeeding.
Limit or avoid foods with added sugar and follow a low-GL diet.
Avoid artificial colourings and flavour additives, such as MSG.
Optimise omega-3 intake from seafood and eggs, and supplement with omega-3 DHA and EPA.
Ensure adequate vitamin A and D intake, with sufficient sun exposure to support vitamin D levels.
Support healthy methylation with B vitamins, especially vitamin B12 for vegans and those on a predominantly plant-based diet.
Check for food intolerances, including gluten, if digestive symptoms are present.
It is also important to note that the DRIfT test can be administered to any child over the age of two. Also note you can do the DRIfT test on any child over 2 years old. Find out more about the DRIfT test here
The Future of Neurodivergence: Prevention and Support
While some neurodevelopmental conditions may not be entirely preventable, improving prenatal and childhood nutrition can help reduce risks and alleviate symptoms. The rising prevalence of neurodivergence suggests an urgent need to address environmental and dietary factors [10]. Rather than normalising suboptimal brain development, prioritising nutrition and early intervention can improve outcomes for neurodivergent individuals.
By fostering a deeper understanding of how environmental and nutritional factors influence neurodivergence, we can better support individuals in reaching their full potential while reducing unnecessary suffering.
—
Join us in our Smart Kids Campaign!
How to get involved:
Attend the Optimising Neurodivergence Webinar – happening on 24th April at 6:30 PM – sign up here
Register for the Smart Kids Conference – an all-day event for health professionals and practitioners on 24th April, 2025. – sign up here
Donate to the Smart Kids Programme – help support neurodivergent children – find out more here
—
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
3. Tutt, R. Neurodiversity insights. Trustee and Scientific Advisor, Food for the Brain.
4. Pfeiffer, C. Nutritional insights. Pfeiffer Treatment Center.
5. McNulty, H., et al. (2019). Effect of continued folic acid supplementation beyond the first trimester of pregnancy on cognitive performance in the child: a follow-up study from a randomized controlled trial (FASSTT Offspring Trial). BMC Medicine, 17(1), 196. doi:10.1186/s12916-019-1432-4.
6. Hibbeln, J.R., et al. (2007). Maternal seafood consumption in pregnancy and neurodevelopmental outcomes in childhood (ALSPAC study). Lancet, 369(9561), 578–585. doi:10.1016/S0140-6736(07)60277-3.
7. Liu, Z. (2021). The Impact of Vitamin A on Cognitive Functions. Behavioral Neurology, 2021:5417497. doi:10.1155/2021/5417497.
8. Veena, S.R., et al. (2010). Higher maternal plasma folate but not vitamin B-12 concentrations during pregnancy are associated with better cognitive function scores in 9- to 10-year-old children in South India. Journal of Nutrition, 140(5), 1014–1022. doi:10.3945/jn.109.118075.
9. Roigé-Castellví, J., Murphy, M., Fernández-Ballart, J., & Canals, J. (2019). Moderately elevated preconception fasting plasma total homocysteine is a risk factor for psychological problems in childhood. Public Health Nutrition, 22(9), 1615–1623. doi:10.1017/S1368980018003610.
10. Kranz, S., Jones, N.R.V., & Monsivais, P. (2017). Intake Levels of Fish in the UK Paediatric Population. Nutrients, 9(4), 392. doi:10.3390/nu9040392.
Written by Dr Victoria Sampson BDS MFDS RCS Ed Pg Dip
Did you know that similar to your gut, the mouth has its own microbiome?
Not only that, it is in fact, the second most diverse microbiome after the gut and houses approximately 700 different species of bacteria that make up 2 billion bacteria!
Unlike its relatives the gut, skin and vaginal microbiomes, the oral microbiome unfortunately has remained in the shadows, with very few even knowing they have one. What people also may not know, is how important their oral microbiome is for not only their oral health, but also their general health. When the oral microbiome is imbalanced and there are more bad bacteria than good, problems occur. In the mouth, these problems can show as tooth decay, gum disease, ulcers and bad breath to name a few. For the rest of the body, an imbalanced oral microbiome can contribute to systemic diseases such as neurological diseases, metabolic diseases, cardiovascular diseases and the list goes on.
—
Why is Alzheimer’s a leading cause of mortality
In the last twenty years we have witnessed an unexplainable rise in the diagnosis of neurological conditions and a decline in brain function in our population. Alzheimer’s Disease is a disease that is currently a leading cause of mortality and morbidity globally (1). It presents as one of the greatest medical challenges that we face this century due to its increasing prevalence worldwide and as yet, no effective treatment developed for it.
Furthermore, the cause of Alzheimer’s is believed to be multifactorial and a combination of genetic, environmental and lifestyle factors. Whilst some of the risk factors for Alzheimer’s cannot be altered such as our genetic makeup, the link between Alzheimer’s and oral health has gained significant traction. Not only can it be altered (and easily), but it also can be tested in a painless and easy way through saliva collection.
—
Inflammation: Why The Mouth is a Gateway to the Brain
One of the primary ways in which oral health affects brain function is through low grade chronic inflammation.
The oral microbiome is a delicate and beautiful balance of good and bad bacteria. If more bad bacteria are able to proliferate in the mouth, this balance can shift into what we call dysbiosis (or an imbalanced oral microbiome). Things that may cause our microbiome to shift into imbalance are things like poor oral hygiene, smoking, diet, medications we take, dry mouth and mouth breathing to name a few. Once the oral microbiome shifts into dysbiosis, this can increase our risk of local diseases such as decay and gum disease, but more importantly causes the release of inflammatory markers from the mouth to the brain.
These inflammatory markers can enter the bloodstream and cross the blood-brain barrier; a protective shield that typically prevents harmful substances from reaching the brain. Once inflammation spreads to the brain, it can contribute to the development of neurological disorders. Chronic inflammation has been linked to cognitive decline and neurodegenerative diseases such as Alzheimer’s disease, as it can damage brain cells and interfere with brain function (2).
Oral Bacteria and Brain Health
Another significant link between the mouth and the brain involves the direct effects of oral bacteria. Researchers have found that bacteria from the mouth can travel to the brain, particularly in cases of poor oral health or severe gum disease. These bacteria can enter the bloodstream through infected gums or the roots of decayed teeth, and eventually reach the brain, where they can contribute to the formation of harmful plaques.
A notable example is the bacterium Porphyromonas gingivalis, commonly found in patients with chronic gum disease. Studies have detected this bacterium in the brains of patients with Alzheimer’s disease, and it has been suggested that the bacteria’s presence may contribute to the development of amyloid plaques—a hallmark of Alzheimer’s. A 2019 study published in Science Advances (3). showed that P. gingivalis not only reaches the brain but also releases toxins known as gingipains, which can damage brain cells and accelerate cognitive decline. Another study in Taiwan performed a retrospective cohort study on 18,672 citizens and found that having gum disease for over ten years was associated with a 70% increase in the risk of developing Alzheimer’s disease (4).
If you’re still not convinced, a study published in the journal of Alzheimer’s Disease (5) further illustrated that there is a direct correlation between periodontal disease and Alzheimer’s Disease. The research looked at 6000 participants spanned over multiple age groups and followed them for up to 26 years. They performed dental examinations for gum disease as well as testing for bacteria and antibodies. The bacteria that seemed to be elevated in patients who went on to suffer Alzheimer’s disease was again, Porphyromonas gingivalis.
This discovery has sparked interest in the potential role of oral bacteria in neurodegenerative diseases. Although more research is needed to establish a definitive cause-and-effect relationship, the evidence suggests that maintaining good oral hygiene could play an important role in preventing or slowing the progression of conditions like Alzheimer’s disease. It also opens the door to saliva testing to test for bacteria such as Porphyromonas gingivalis in the microbiome and eradicating this before it can cause problems.
—
Stroke and Oral Health
The connection between oral health and the brain is also evident in the relationship between gum disease and stroke. Stroke occurs when blood flow to the brain is interrupted, leading to brain cell death and potentially severe neurological impairment. Gum disease is associated with an increased risk of stroke due to the systemic inflammation it causes and the potential for oral bacteria to contribute to the formation of blood clots.
A 2018 study published in the journal Stroke, (6 Sen, 2018) found that individuals with severe gum disease were at a higher risk of ischemic stroke, which occurs when a blood clot blocks an artery supplying blood to the brain. The study suggested that the chronic inflammation caused by gum disease may contribute to the formation of clots, which can travel to the brain and cause a stroke.
Moreover, researchers have found that treating gum disease can reduce markers of inflammation in the body, potentially lowering the risk of stroke. This highlights the importance of oral health not only for preventing gum disease but also for reducing the risk of serious neurological events like stroke.
—
The Mouth and Brain are Deeply Connected
The connection between the mouth and the brain is a reminder that the body’s systems are deeply interconnected. Poor oral health, particularly in the form of gum disease and oral infections, can have far-reaching effects on brain function and overall neurological health. Inflammation and the spread of harmful oral bacteria are two key mechanisms by which oral health can influence conditions such as Alzheimer’s disease and stroke.
As research continues to shed light on this important connection, it becomes increasingly clear that maintaining good oral hygiene is essential not only for a healthy mouth but also for a healthy brain.
For individuals looking to protect their cognitive function and reduce the risk of neurological diseases here are a few tips:
Complete the Cognitive Function Test here today so you can get a personalised plan on how to improve your overall cognition.
All the above alongside a balanced diet and regular exercise.
—
If you want to learn more about the Oral Microbiome then make sure you join us for the Oral-Gut-Brain Connection Webinar with Victoria Sampson. Find out more here.
Thank you for reading!
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
REFERENCES
Vos T. Estimating the global mortality from Alzheimer’s disease and other dementias: A new method and results from the Global Burden of Disease study 2019. J Alzheimers Assoc. 2020.
Kamer, A. R. (2020). Inflammation and Alzheimer’s disease: Possible role of periodontal diseases. Alzheimer’s & Dementia.
Dominy S, et al. Porphyromonas gingivalis in Alzheimer’s disease brains: Evidence for disease causation and treatment with small-molecule inhibitors. Sci Adv. 2019.
Chang-Kai C, et al. Association between chronic periodontitis and the risk of Alzheimer’s disease: a retrospective, population-based, matched-cohort study. Alzheimers Res Ther. 2017.
Beydoun M, et al. Clinical and bacterial markers of periodontitis and their association with incident all-cause and Alzheimer’s disease dementia in a large national survey. J Alzheimers Dis. 2020;57–172.
Sen E. Periodontal Disease, Regular Dental Care Use, and Incident Ischemic Stroke. Stroke. 2018.
Folic Acid and Methylation Myths: Facts, Fallacies and What the Evidence Suggests
If you have spent any time reading about folic acid, methylfolate, MTHFR or methylation, you have probably come away with more questions than answers. One article claims folic acid is essential. Another insists it is harmful. Some suggest everyone should switch to methylfolate, while others argue the difference barely matters. It is no surprise that so many people end up confused.
The reality is more interesting than either extreme. Much of the debate comes from taking a small piece of biology and stretching it into sweeping conclusions that the evidence does not support. Genes, nutrients and metabolism do interact in fascinating ways, but they rarely fit into simple “good versus bad” stories.
Much of the discussion around folic acid, methylfolate, MTHFR and homocysteine has become increasingly polarised. This article examines several common misconceptions and reviews what the current evidence actually shows.
If you are new to the topic, start with our guide to methylation and homocysteine first. This article is designed as a deeper companion that challenges common misconceptions and adds context to the finer details.
Why Homocysteine Matters in the Folic Acid Debate?
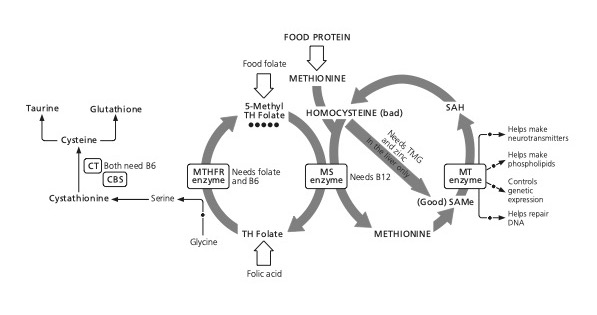
Homocysteine is an intermediary sulphur-containing amino acid generated during methionine metabolism. Under physiological conditions, it is either remethylated to methionine or irreversibly metabolised through the transsulphuration pathway. These reactions depend on an adequate supply of folate, vitamin B12, vitamin B6 and other methylation cofactors.
Because homocysteine reflects the functional efficiency of one-carbon metabolism, it is widely used as a functional biomarker of methylation capacity and folate status. Much of the debate surrounding folic acid, methylfolate and MTHFR variants centres on their effects on these metabolic pathways and, consequently, on homocysteine concentrations. Homocysteine should therefore be interpreted within the broader context of one-carbon metabolism, nutritional status and individual genetic variation, rather than as an isolated biomarker.
—
Methionine and methylation cycle
Fallacy 1: Folic Acid Doesn’t Work
One of the most persistent misconceptions in nutritional medicine is that folic acid is ineffective and that only methylfolate should be used. This is not supported by the evidence. Folic acid has consistently been shown to lower homocysteine, both on its own and in combination with vitamins B6 and B12. In studies I have reviewed, the beneficial effect on homocysteine is seen regardless of whether an individual carries the common MTHFR C677T polymorphism.
This does not mean that folic acid is always the optimal choice. Folic acid must first be converted into its biologically active form through a series of enzymatic steps. Variations in genes encoding these enzymes, particularly DHFR and, to a lesser extent, MTHFR, can reduce the efficiency of this process in some individuals. However, reduced enzyme activity should not be confused with an inability to utilise folic acid. For most people, particularly those of European ancestry, folic acid remains an effective way to support methylation and lower elevated homocysteine.
There is good evidence that methylfolate raises red blood cell folate more efficiently and lowers homocysteine more effectively than folic acid. In some studies, methylfolate has reduced homocysteine by around 40 to 50% more than an equivalent dose of folic acid. This makes methylfolate a sensible choice where available, particularly for individuals with reduced DHFR activity or those who respond poorly to folic acid.
The important distinction is that saying methylfolate may be superior is not the same as saying folic acid does not work. The scientific evidence does not support that conclusion. For the majority of people, folic acid effectively supports one-carbon metabolism and lowers homocysteine, while methylfolate may provide additional benefit in specific clinical or genetic circumstances.
Fallacy 2: Everyone Needs Methylfolate
Methylfolate is the biologically active form of folate and bypasses the enzymatic steps required to convert folic acid into its active form. As a result, it has been shown to raise red blood cell folate more effectively and lower homocysteine more than equivalent doses of folic acid. This has led some practitioners to recommend methylfolate in preference to folic acid for everyone.
However, the evidence does not support such a universal approach. For most people, folic acid is effectively converted into methylfolate and successfully supports methylation. Numerous intervention studies have shown that folic acid, particularly when combined with vitamins B6 and B12, lowers homocysteine regardless of MTHFR C677T genotype.
There are, however, circumstances in which methylfolate may offer advantages. Individuals with reduced activity of the DHFR enzyme, which is responsible for the first step in folic acid metabolism, may be less able to convert folic acid efficiently. This genetic variation is relatively uncommon in European populations but considerably more prevalent in some Asian populations. In these individuals, methylfolate or folinic acid may represent a more appropriate choice.
The decision should therefore be based on an individual’s nutritional status, genetic background and clinical response rather than the assumption that everyone requires methylfolate. While methylfolate is generally the preferred supplemental form because it bypasses the activation pathway, it is incorrect to conclude that folic acid has no place in clinical practice.
Fallacy 3: MTHFR Means You Can’t Process Folic Acid
One of the most widespread misconceptions is that carrying an MTHFR C677T or TT polymorphism means you cannot process folic acid. This is an oversimplification of how one-carbon metabolism works. The MTHFR enzyme is responsible for converting tetrahydrofolate into 5-methyltetrahydrofolate (5-MTHF), and reduced enzyme activity may influence methylation efficiency, particularly if riboflavin (vitamin B2) status is suboptimal.
The MTHFR C677T polymorphism is common, affecting around 24% of the population overall, although prevalence varies considerably between ethnic groups. Individuals with this variant may have higher homocysteine levels and an increased risk of certain conditions, particularly when B vitamin status is inadequate. However, this does not mean they are unable to utilise folic acid.
Intervention studies consistently show that supplementation with folic acid, particularly alongside vitamins B6 and B12, lowers homocysteine regardless of MTHFR genotype. In other words, people with the C677T or TT polymorphism still respond to folic acid. Ensuring adequate riboflavin status may further support MTHFR enzyme activity in those with these variants.
The presence of an MTHFR polymorphism should therefore be viewed as one factor influencing methylation efficiency rather than evidence that folic acid is ineffective. It may influence the choice of folate supplement in some individuals, but it does not justify the conclusion that everyone with an MTHFR variant is unable to process folic acid.
Fallacy 4: Unmetabolised Folic Acid Is Always Harmful
Another common claim is that the presence of unmetabolised folic acid (UMFA) in the bloodstream is inherently harmful. The reality is more nuanced. UMFA can accumulate when folic acid intake exceeds the body’s capacity to convert it into biologically active folate, particularly in individuals with reduced activity of the dihydrofolate reductase (DHFR) enzyme, which catalyses the first step in folic acid metabolism.
The concern is that unmetabolised folic acid may compete with naturally occurring folate for enzyme binding sites, potentially impairing normal folate-dependent metabolism. This has led to suggestions that excessive folic acid supplementation could, under certain circumstances, induce a functional folate deficiency. However, the likelihood of this depends on both the amount of folic acid consumed and an individual’s genetic capacity to metabolise it.
Reduced DHFR activity is relatively uncommon in European populations but considerably more prevalent in some Asian populations. Individuals with reduced DHFR activity are more likely to accumulate UMFA and may therefore benefit from using methylfolate or folinic acid instead of folic acid. By contrast, there is little evidence that modest intakes of folic acid, such as those typically found in multivitamin supplements, represent a significant concern for most people.
Another area of ongoing research is the relationship between folate and cancer. Folates are essential for DNA synthesis and cell division, meaning they support the growth of healthy cells but may also accelerate the growth of existing pre-cancerous or cancerous cells. While adequate folate intake appears protective before malignant change occurs, excessive folic acid exposure, particularly in susceptible individuals with reduced DHFR activity, may not always be desirable. This remains an area of active investigation rather than settled science.
The practical conclusion is not that folic acid is harmful, but that the form and dose of folate should be matched to the individual. Methylfolate provides the biologically active form without requiring DHFR conversion and may therefore be preferable where reduced enzyme activity is suspected. Nevertheless, the current evidence does not support the conclusion that the presence of unmetabolised folic acid is inherently harmful in everyone.
Fallacy 5: Homocysteine Should Always Be as Low as Possible
Raised homocysteine is associated with an increased risk of numerous chronic diseases and, in most circumstances, lowering an elevated level is beneficial. However, it does not necessarily follow that the lowest possible homocysteine concentration is always the optimal goal.
Homocysteine is not simply a waste product. It is an intermediate metabolite within one-carbon metabolism and also serves as the precursor for glutathione synthesis through the transsulphuration pathway. This pathway depends on the enzyme cystathionine β-synthase (CBS), together with adequate vitamin B6 status. Theoretically, if homocysteine concentrations become extremely low, substrate availability for glutathione synthesis could also be reduced.
In practice, homocysteine concentrations below 4 µmol/L are uncommon, and evidence that very low levels are harmful is limited. Where both homocysteine and glutathione are unusually low, it may indicate impaired folate metabolism or reduced activity of enzymes involved in one-carbon metabolism, such as DHFR or MTHFR, rather than representing an ideal metabolic state.
The key point is that homocysteine should not be interpreted in isolation. It is a functional biomarker that reflects the efficiency of interconnected metabolic pathways and should be considered alongside glutathione status, B vitamin sufficiency and the wider clinical picture. The objective is not to achieve the lowest possible homocysteine concentration, but to support efficient methylation and healthy one-carbon metabolism.
Fallacy 6: More Folate Is Always Better
While maintaining adequate folate status is essential for healthy one-carbon metabolism, more folate is not necessarily better. As with many nutrients, both the form and the dose matter, and the optimal approach depends on an individual’s nutritional status, genetic background and clinical circumstances.
Adequate folate intake supports DNA synthesis, methylation and normal cell division, and sufficient folate status before the development of pre-cancerous changes appears to reduce disease risk. However, once pre-cancerous lesions are established, high circulating folate concentrations, particularly from excessive folic acid supplementation, may accelerate the growth of rapidly dividing cells. This distinction is important and helps explain why the relationship between folate and cancer is more complex than simple claims of benefit or harm.
Individuals with reduced DHFR activity are also more likely to accumulate unmetabolised folic acid when consuming high supplemental doses. In these circumstances, using methylfolate or folinic acid may be a more appropriate strategy than simply increasing folic acid intake. Conversely, for most people, modest amounts of folic acid remain an effective and safe way to support methylation and maintain healthy homocysteine metabolism.
The evidence therefore supports an individualised approach rather than a universal recommendation. The aim should be to achieve adequate folate status using the most appropriate form and dose for the individual, guided wherever possible by biomarkers such as homocysteine and the wider clinical picture, rather than assuming that increasing folate intake indefinitely will produce greater health benefits.
What This Means in Practice
The evidence does not support absolute positions on folic acid or methylfolate. Folic acid remains an effective way to support one-carbon metabolism and lower homocysteine in most people, while methylfolate may offer advantages for some individuals, particularly those with reduced DHFR activity or a poor response to folic acid.
Similarly, the presence of an MTHFR polymorphism should not be interpreted as meaning that folic acid is ineffective or that methylfolate is essential for everyone. Nutritional status, enzyme activity and clinical context are all important considerations when selecting the most appropriate form of folate.
Rather than relying on assumptions or genetic results alone, a more evidence-based approach is to assess functional biomarkers such as homocysteine and interpret these alongside the wider clinical picture. This enables nutritional interventions to be tailored to the individual rather than based on generalisations.
If you’d like to understand the science behind one-carbon metabolism in more detail, explore our Methylation and Homocysteine guide, which explains how methylation works, why homocysteine is such an important biomarker, and how nutrients support these interconnected pathways.
If you don’t know your homocysteine level, consider taking a homocysteine blood test. Homocysteine is one of the most informative functional biomarkers of methylation and brain health, and measuring it provides a practical starting point for understanding your individual nutritional status.
If your homocysteine level is elevated, our evidence-based guide to Lowering Homocysteine explains the role of diet, B vitamins, methylfolate and lifestyle interventions, helping you translate these scientific principles into practical action. ou can also explore our Homocysteine Lowering B Vitamins supplement guide for practical support in putting these strategies into action.
Where appropriate, further investigation, such as testing glutathione status or DHFR genetic variants, may help explain why some individuals respond differently to folic acid and identify when alternative forms of folate may be beneficial.
For those who would like to dig even deeper, these papers are most relevant:
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
Your Glutathione Index Defines How Your Cells Are Ageing
Nutritional therapists have been measuring red cell glutathione and supplementing glutathione or its precursor N-Acetyl-Cysteine (NAC) for decades. But it’s really hard, and expensive, to measure accurately. Until now.
So how does the Glutathione Index work?
All of life is a balance between antioxidants and oxidants. That is why we, an oxygen based lifeform, have a finite life. Inside your cells glutathione (GSH) is working every second to stop harmful oxidants from ageing you. The result is spent or oxidised glutathione (GSSG). Our new test – a world first – measures the ratio between fully loaded glutathione (GSH) and oxidised glutathione (GSSG). The Glutathione index (GSH/GSSG) shows you how much antioxidant potential you have and how many metabolic fires you’ve extinguished. This ratio is the difference between mental health and mental illness.
Why does knowing this single marker help with Alzheimer’s, diabetes, schizophrenia, severe autism, depression & more?
Why Does Knowing This Single Marker Help With Alzheimer’s, Diabetes, Schizophrenia, Severe Autism, Depression and More?
The Science
NAC has plenty of evidence to support its use as a promoter of glutathione and mental health, thus reducing the brain’s oxidative stress. The latest 2022 review states:
“N-acetyl-L-cysteine (NAC) is a compound of increasing interest in the treatment of psychiatric disorders. Primarily through its antioxidant, anti-inflammatory, and glutamate modulation activity, NAC has been investigated in the treatment of neurodevelopmental disorders, schizophrenia spectrum disorders, bipolar-related disorders, depressive disorders, anxiety disorders, obsessive compulsive-related disorders, substance-use disorders, neurocognitive disorders, and chronic pain. Currently NAC has the most evidence of having a beneficial effect as an adjuvant agent in the negative symptoms of schizophrenia, severe autism, depression, and obsessive compulsive and related disorders.” (1)
Glutathione and Schizophrenia
Quoting Lorraine Wilder (whose MSc in schizophrenia we funded) “Glutathione (GSH) is an important antioxidant and free radical scavenger that has been found to be decreased in the brains of people with schizophrenia [2, 3]. Although oral GSH supplementation has poor bioavailability [4], N-Acetyl Cysteine (NAC) has been shown to successfully raise plasma glutathione levels in those with schizophrenia [5]”.
Clinical Evidence and Case Studies
In a case study of a 24 year old woman with chronic and worsening paranoid-type schizophrenia that was generally unresponsive to anti-psychotic treatment, the addition of NAC supplementation improved the patient’s symptomatology in seven days. In addition to the schizophrenia-specific symptoms, improvements were observed in spontaneity, social skills and family relations by both the patient and family members. A randomised placebo-controlled trial (RCT) including 42 participants with schizophrenia, who were experiencing an acute phase of symptomatology, were randomly assigned to receive up to 2 g/d of NAC plus up to 6 mg/d of risperidone for 8 weeks as an adjunct intervention. Significant negative symptoms were found in the active treatment group compared to controls but not in positive or general psychopathology [6].
Larger Trials and Longer-Term Findings
Furthermore, a larger RCT of 140 participants observed significant improvements on global symptomatology and general and negative symptoms of schizophrenia in the NAC supplementation (2 g/d; in addition to anti-psychotic medication) group in comparison to the placebo group over a 24-week period, but not positive symptoms [7]. Notably, after a 4-week washout period these beneficial effects diminished, with the exception of clinical severity scores.
Expert Perspective on Brain Oxidative Stress
According to Dr Chris Palmer, assistant professor at HarvaWhy the Glutathione Index Is the Best Indicator of Brain Oxidative Stress rd Medical School:
“Glutathione (GSH), the brain’s primary antioxidant, plays a crucial role in maintaining redox balance. Magnetic resonance studies have provided mixed results regarding GSH levels in schizophrenia patients, with some studies indicating decreased levels in chronic schizophrenia, while others found no significant differences. However, these inconsistencies may be due to variations in disease chronicity, age, and symptom severity among study participants. The findings from these studies suggest several potential therapeutic targets for schizophrenia. Addressing mitochondrial dysfunction, redox imbalance, and impaired energy metabolism could lead to more effective treatments. For instance, N-acetylcysteine (NAC), a precursor to GSH, has shown promise in increasing brain GSH levels and improving symptoms in first episode psychosis patients.”
Why the Glutathione Index Is the Best Indicator of Brain Oxidative Stress
The GSH/GSSG ratio reflects the activity of the enzyme glutathione reductase which is responsible for the transformation of GSSG (used, oxidised) to GSH (the reduced or fully loaded form that acts as a radical scavenger).
—
Glutathione Reductase and Dementia
Reductions in glutathione reductase (GR) enzyme levels in patients with dementia are well established. GR levels alone are therefore a fairly good biomarker of dementia. But the mere presence of the enzyme does not guarantee its high activity. GR needs to consume NADP molecules to function properly. The advantage of our test is, therefore, that it shows changes in GR activity not only due to higher/lower GR gene activity but also due to the absence of the reaction cofactor NADP.
Impaired Glutathione Recycling in Dementia
As shown by Irene Martinez de Toda et al 2019 (8) data, patients with dementia have a reduction in both the enzymes (GR and GP) that recycle glutathione. Thus, in general, it can be said that the glutathione metabolism (recycling) loop in those with dementia ‘spins’ much slower than in healthy patients. As a result, dementia patients have a lower potential to dynamically fight free radicals and will have a worse Glutathione Index.
What Happens When Recycling Slows Down
In patients, the enzyme GR, which is responsible for recycling spent/oxidised glutathione back to fully loaded, slows down, which leads to the accumulation of oxidised glutathione (GSSG) and the depletion and inability to produce GSH.
Thus, the concentration of GSH decreases while that of GSSG increases. Hence the Glutathione Index gets worse / is lower.
Improving your Glutathione Index
The older a person is the lower their Glutathione Index is likely to be (see figure below)
Improving your Glutathione index is important as higher levels predict better cognitive function according to our preliminary research. (see figure).
Our own laboratory’s study of 8 people given a supplement containing lipoid acid and N-acetyl-Cysteine (NAC) supplements, the precursor for glutathione, show improvement in both the Glutathione Index and Glutazthione. (see figure below)
Studies giving Ubiquinol, the active form of CoQ, also show an improvement in both the Glutathione Index
Developing the Glutathione Index Test
This is why we have created the Glutathione Index test alongside analytic chemist, Dr Konrad Kowalski. “This ratio, the Glutathione Index, is a biomarker for many diseases, including both type 1 and 2 diabetes, liver cirrhosis, multiple sclerosis and Alzheimer’s disease.” says Dr Kowalski, “As a result of having good data, our scientists are currently reviewing the reference ranges to be even more accurate. Having a way to measure brain ageing with a home test kit from a pin prick of blood, means we can realistically see what the impact of specific diet changes and antioxidant supplements might be.”
We now know that a desirable level is above 800. Below 500 is an indicator that you need to increase your intake of antioxidants from food and/or supplements, and/or reduce your intake of oxidants from smoking, pollution or fried food.
So will you join us and become a part of our Anti-Age Your Brain Campaign? We need Citizen Scientists to order and complete the test so you can start to protect your brain from ageing and so we can research what the ‘perfect number’ is.
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
References
1. Bradlow RCJ, Berk M, Kalivas PW, Back SE, Kanaan RA. The Potential of N-Acetyl-L-Cysteine (NAC) in the Treatment of Psychiatric Disorders. CNS Drugs. 2022 May;36(5):451-482. doi: 10.1007/s40263-022-00907-3. Epub 2022 Mar 22. Erratum in: CNS Drugs. 2022 Apr 28;: PMID: 35316513; PMCID: PMC9095537.
2 Yao JK, Leonard S, Reddy R: Altered glutathione redox state in schizophrenia. Dis Markers 2006, 22(1):83–93.
3 Gawryluk JW, Wang J-F, Andreazza AC, Shao L, Young LT: Decreased levels of glutathione, the major brain antioxidant, in post-mortem prefrontal cortex from patients with psychiatric disorders. Int J Neuropsychopharmacol 2011, 14(01):123–130.
4 Witschi A, Reddy S, Stofer B, Lauterburg B: The systemic availability of oral glutathione. Eur J Clin Pharmacol 1992, 43(6):667–669.
5. Lavoie S, Murray MM, Deppen P, Knyazeva MG, Berk M, Boulat O, Bovet P, Bush AI, Conus P, Copolov D, Fornari E, Meuli R, Solida A, Vianin P, Cuénod M, Buclin T, Do KQ:Glutathione precursor, N-acetyl-cysteine, improves mismatch negativity in schizophrenia patients. Neuropsychopharmacology 2008, 33(9):2187–2199.
6. Farokhnia M, Azarkolah A, Adinehfar F, Khodaie-Ardakani M-R, Hosseini S-M-R, Yekehtaz H, Tabrizi M, Rezaei F, Salehi B, Sadeghi S-M-H, Moghadam M, Gharibi F, Mirshafiee O:, Akhondzadeh S: N-acetylcysteine as an adjunct to risperidone for treatment of negative symptoms in patients with chronic schizophrenia: a randomized, double-blind, placebo-controlled study. Clin Neuropharmacol 2013, 36(6):185–192.
7. Berk M, Copolov D, Dean O, Lu K, Jeavons S, Schapkaitz I, Anderson-Hunt M, Judd F, Katz F, Katz P, Ording-Jespersen S, Little J, Conus P, Cuenod M, Do KQ, Busha AI: N-acetyl cysteine as a glutathione precursor for schizophrenia—a double-blind, randomized, placebo-controlled trial. Biol Psychiatry 2008, 64(5):361–368.
8. Martínez de Toda I, Vida C, Sanz San Miguel L, De la Fuente M. Function, Oxidative, and Inflammatory Stress Parameters in Immune Cells as Predictive Markers of Lifespan throughout Aging. Oxid Med Cell Longev. 2019 Jun 2;2019:4574276. doi: 10.1155/2019/4574276. PMID: 31281577; PMCID: PMC6589234.
9.Tian G, Sawashita J, Kubo H, Nishio SY, Hashimoto S, Suzuki N, Yoshimura H, Tsuruoka M, Wang Y, Liu Y, Luo H, Xu Z, Mori M, Kitano M, Hosoe K, Takeda T, Usami S, Higuchi K. Ubiquinol-10 supplementation activates mitochondria functions to decelerate senescence in senescence-accelerated mice. Antioxid Redox Signal. 2014 Jun 1;20(16):2606-20. doi: 10.1089/ars.2013.5406. Epub 2013 Dec 14. PMID: 24124769; PMCID: PMC4025630.] and glutathione in people with metabolic syndrome
10.Raygan F, Rezavandi Z, Dadkhah Tehrani S, Farrokhian A, Asemi Z. The effects of coenzyme Q10 administration on glucose homeostasis parameters, lipid profiles, biomarkers of inflammation and oxidative stress in patients with metabolic syndrome. Eur J Nutr. 2016 Dec;55(8):2357-2364. doi: 10.1007/s00394-015-1042-7. Epub 2015 Sep 18. PMID: 26385228.)