This is the question we get asked all the time from our community.
Normally if they go to the doctor they may get referred to a memory clinic for a Cognitive Function Test. Some get invited to take part in drug trials and there are basically two kinds of drugs under investigation – anti-amyloid and anti-p-tau. If you’re tempted to participate in any test, we would suggest finding out which type is being tested. So far the anti-amyloid treatments have not delivered any significant clinical benefit and lots of adverse effects including deaths. Anti p-tau drugs have not yet been proven to work. However, p-tau accumulation, making neurofibrillary tangles, is a function of high homocysteine which is lowered with B vitamins (see below). We know this already. So why not test and lower homocysteine with B vitamins?
Some people get prescribed cholinesterase inhibitor drugs, designed to stop the breakdown of acetylcholine. These include rivastigmine, donepezil (Aricept) and galantamine. They are marginally effective, but the effect runs out after 2 years (see why below and other approaches).
—
The first steps:
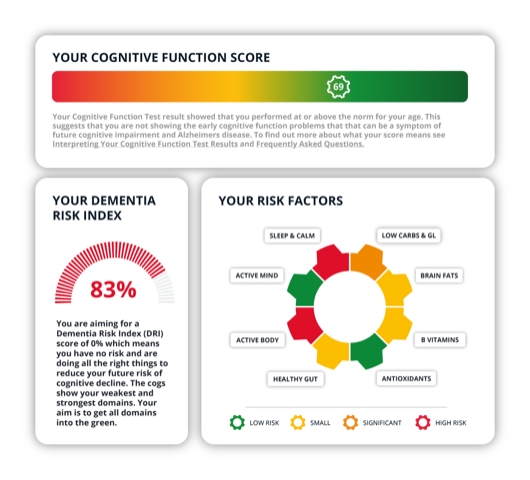
The first step, with help, is to do the Cognitive Function Test here (which they may struggle with), followed by a questionnaire.
Even if they can’t complete the Cognitive Function Test, do encourage them to continue and complete the questionnaire because this will show where the weak areas that need attention are. An example test result is below.
Ideally, they should then sign up as a FRIEND to get access to COGNITION and a focused brain upgrade but if they are too far progressed to receive and respond to emails, then here are some quick wins.
—
At home tests to run & what to do with the results
First, have them do the DRIfT home test to measure HBA1c, homocysteine, omega-3 index and vitamin D. If you know their HbA1c and vitamin D already then you can test these individually (see all test options here).
From a raised HbA1c we’d know if sugar balance is a problem, in which case 2 tablespoons (60g) of C8 oil is likely to help, as well as eating low carbs and avoiding sugar as much as possible (and limit alcohol). The C8 oil helps the brain make ketones which is an alternative fuel source for brain cells and fills the ‘energy gap’ created by poor glucose delivery, a function of insulin resistance.
If Homocysteine is above 10mcmol/l. we’d know they need homocysteine lowering B vitamins (including supplementing vitamin B12 500mcg – see here)
If Vitamin D is below 75nmol/l they need to supplement – probably 1,000 to 3,000ius a day or 10,000-20,000ius a week. Click here to read more about what’s needed depending on their level.
—
How to support neuronal membranes
Neuronal membranes, which is what breaks down in dementia, are made from phospholipids binding to omega-3, which require B vitamins to drive a process called methylation.
If this process is not working efficiently, homocysteine goes up.
A critical phospholipid is Phosphatidyl Choline (PC), bound to omega-3 DHA (known as PC-DHA, which predicts dementia if low). The cholinesterase inhibitor drugs try to protect this but why not supplement phosphatidyl choline, which is very rich in lecithin capsules or granules? Two high PC lecithin capsules, plus at least 500 mg of omega-3 DHA, plus homocysteine-lowering B vitamin complexes cover all bases. See here for more information on supplements.
A diet low in sugar and carbs, with lots of oily fish, regular exercise and as much social and intellectual stimulation as possible along with good sleep, all make a big difference and we guide you through that in COGNITION for £5 a month or £50 a year. Access COGNITION by joining as a FRIEND here.
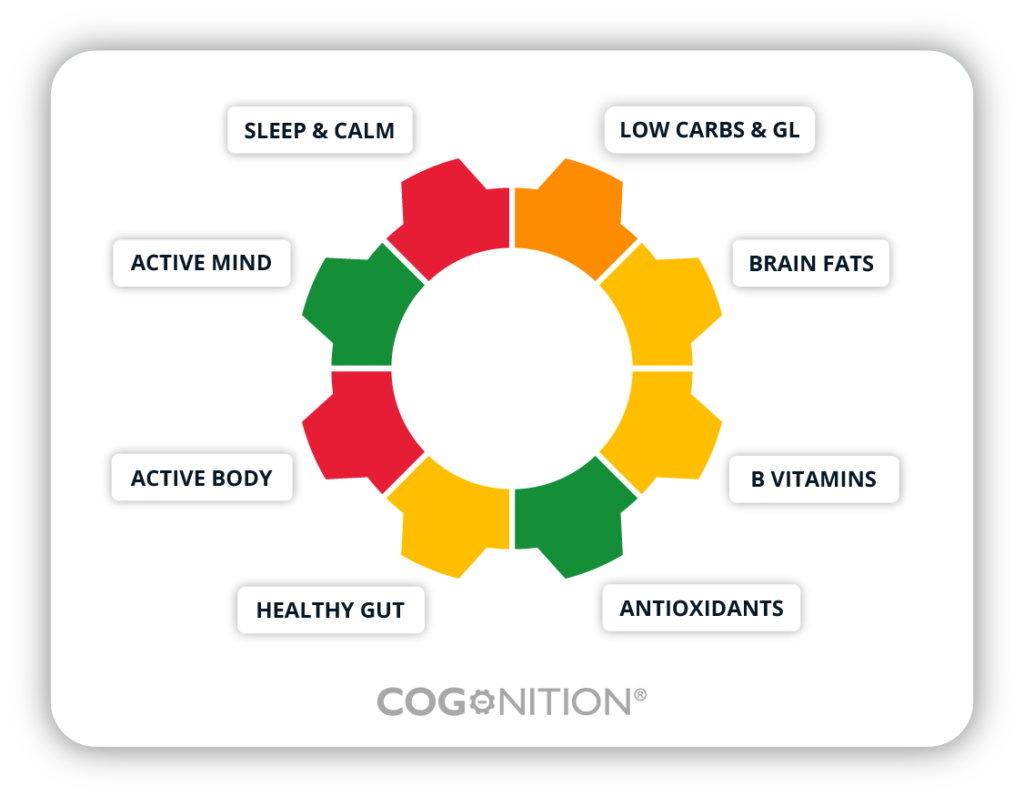
Once the Cognitive Function Test is complete, you will get a personalised result showing the areas that are ‘in the green’ and the areas you need to focus on (bear in mind that if dementia is already diagnosed, there will probably be a lot of red and amber colours).
All tests ordered and completed contribute to our charitable work and independent research and are a part of our Citizen Science mission!
—
Thank you for reading!
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
Attention-Deficit Hyperactivity Disorder (ADHD) is not just an issue to address with our children. Many adults are finding themselves diagnosed with this brain disorder and conventional medicinal support is limited.
Why are we struggling to focus and concentrate OR focus on one specific task at a cost to our health, relationships and other essential life activities (known as hyperfocus)?
We can see how this, if not managed, can be problematic for children and the impact it can have on their learning and confidence but what if you are an adult who has recently realised that your brain works and struggles differently to those around you? (If you are interested in supporting your child’s brain then join our Smart Kids & Teens programme here.)
The incidence of neurodevelopmental disorders like Attention-Deficit Hyperactivity Disorder (ADHD) and Autism Spectrum Disorder (ASD) has surged in recent years and both are classified as neurodivergent conditions (along with other conditions like learning disabilities, attention-deficit and anxiety disorders, obsessive-compulsive disorder and Tourette’s syndrome).
In the UK and the USA, the rise in diagnoses has been significant, prompting questions about underlying causes and potential solutions. While there may be a familial aspect, we know ‘it is not in the genes’. So, why are we facing this attention deficit disaster?
—
The Attention Deficit Disaster in Adults
ADHD is not confined to childhood; many adults continue to experience its symptoms, which can significantly impact their personal and professional lives. Also, many parents discover this about themselves as they go through the process of getting their child diagnosed.
Common symptoms of adult ADHD include:
Inattention: difficulty sustaining attention during tasks, making careless mistakes, not listening when spoken to directly, and being easily distracted (1,2).
Hyperfocus: paradoxically, some adults with ADHD can become intensely focused on tasks they find stimulating or rewarding, often to the exclusion of other activities (3).
Disorganisation: chronic issues with organising tasks and activities, often leading to missed deadlines and forgotten appointments (4).
Time Management Problems: struggling to manage time effectively, leading to procrastination and difficulty completing tasks (5).
Impulsivity: making hasty decisions without considering the long-term consequences, interrupting others, and difficulty waiting for their turn (6).
Emotional Dysregulation: experiencing intense emotions, such as frustration or anger, and difficulty managing stress (7,8).
—
It looks different for men and women…
ADHD can present differently in men and women, which often leads to underdiagnosis or misdiagnosis in women. Here are some key differences:
Inattention vs. Hyperactivity: women are more likely to exhibit inattentive symptoms, such as disorganisation, forgetfulness, and difficulty focusing. In contrast, men often display more hyperactive and impulsive behaviours, like restlessness and acting without thinking (9,10).
Emotional Symptoms: women with ADHD may experience higher levels of emotional dysregulation, including mood swings, anxiety, and depression. Men are more likely to exhibit externalising behaviours, such as aggression and conduct problems (11,12).
Coping Mechanisms: women tend to develop coping strategies that mask their symptoms, such as becoming perfectionists or overworking to compensate for their inattentiveness. This can delay diagnosis and treatment (13).
Social Consequences: women with ADHD often face significant social consequences, including challenges in maintaining relationships and social isolation. Men, however, may struggle more with academic and behavioural issues in school settings (14,15).
—
Start at the very beginning of brain development…
The adult brain begins at conception, making maternal nutrition crucial.
As well as avoiding alcohol and smoking during pregnancy we know from a study of 11,875 pregnant women there is a clear relationship between the amount of seafood consumed by a pregnant woman and their child’s development. The less seafood consumed, the worse the child’s social behaviour, fine motor skills, communication and social development, and verbal IQ. (16)
In addition, a lack of vitamin A during pregnancy, another nutrient rich in seafood, can affect brain development and lead to long-term or even permanent impairment in the learning process, memory formation, and cognitive function. (17)
Plus, there is folic acid. A mother’s folate intake predicts the child’s performance in cognitive tests at the age of nine to ten (18) and the higher a baby’s B-vitamin status, the higher their cognitive function at the age of 25. (19) Supplementing mothers-to-be with folic acid (400mcg/day) during the second and third trimesters of pregnancy is associated with better cognition in their children at the age of three and better word reasoning and IQ (verbal and performance) at seven.(20)
Nothing can be built properly in the brain without healthy methylation and methylation requires folate (which is reflected by a low homocysteine level). Raised homocysteine is a well-known predictor of miscarriage and pregnancy problems, which is why we recommend that no woman attempts pregnancy until her homocysteine level is below 7 mcmol/l.
While we have learned that a homocysteine level above 11 means increased brain shrinkage, even a homocysteine level of above 9 during pregnancy predicts more problems, specifically withdrawn behaviour, anxiety, depression, social problems and aggressive behaviour in the child at the age of six. (21)
So looking back at your childhood development might help you to understand your adult brain. How well nourished was it? Did you get adequate folate, vitamin A and consume seafoods as a child?
Our hope is some of the deficit in brain function can be recovered by providing all brain-dependent nutrients at an optimal level and see what happens.
What would happen if you started to eat more fish and seafood? Here is some of the science:
Lower DHA concentrations are associated with poorer reading ability, poorer memory, oppositional behaviour and emotional instability. (22)
Several studies have shown increased aggression in those with low omega-3 DHA and EPA, and giving more omega-3 reduces aggression.(23)
Improved IQ and sleep quality: a study of 541 Chinese schoolchildren found that fish consumption predicted sleep quality and that those who ate the most fish had the highest IQ – 4.8 points higher than those who ate none. Improved sleep quality, linked to fish intake, was correlated with IQ. (24)
—
Other Essential Nutrients for Brain Health
The brain needs nourishing, especially in childhood as it is growing and developing rapidly, but also as adults.
Here are some of the essential nutrients you may want to focus on to optimise your brain:
Vitamin A: can affect brain development and lead to long-term or even permanent impairment in the learning process, memory formation, and cognitive function. (17)
Vitamin D: low vitamin D levels in childhood are related to behaviour problems in adolescence (25) and are significantly linked to a higher risk of dementia and cognitive decline. (26, 27, 28)
Chromium, copper, zinc, and magnesium: children with ADHD tend to have lower levels of zinc, chromium, and magnesium, with some having low levels of copper (29). One study found a higher copper to zinc ratio in neurodivergent children compared to neurotypical children, predicting the degree of ADHD (30). Zinc supplementation has been shown to improve memory and attention spans in ADHD (31). Additionally, magnesium deficiency is common in ADHD, and supplementation has been linked to reduced hyperactivity (32). Deficiencies in these minerals can contribute to symptoms of ADHD and other neurodevelopmental disorders.
So are we Neurodivergent or Neurodeficient?
In the chart below are the most common characteristics in those with autistic spectrum disorder by the US Center for Disease Control and Prevention
I’ve added a column for the nutrients, when deficient, that have been shown to induce these symptoms.
Omega-3 DHA, Hcy/B vitamins, dysglycemia (sugar), vitamin C
Lack of fear or more fear than expected
Omega-3 DHA, Hcy/B vitamins, dysglycemia (sugar), vitamin C
Hcy stands for homocysteine which is the best indicator of lack of methylating B vitamins
—
—
Ending your sweet tooth…
It’s not just about specific nutrients, the amount of sugar you consume has a big impact on your brain health.
Too many carbs and ultra-processed foods are bad for anyone at any age, as is too much sugar. They are linked to children’s mental health issues relating to symptoms of ADHD (33) and autism and adult anxiety and depression, (34) and strongly linked to increased risk of age-related cognitive decline, dementia and Alzheimer’s.
Going back to childhood, even the glycemic load of a mother’s diet predicts a massive four-fold risk of anxiety in toddlers, with five times more impulsivity in boys, and four times as many sleeping problems, while girls have 15 times the likelihood of anxiety in those in the top third for glycemic load. (35)
So while you probably already know it, reducing sugar is imperative to your brain health.
—
Gut health & food intolerances
Dr Alessio Fasano, who is both Professor of Paediatrics at Harvard Medical School and Professor of Nutrition at Harvard’s Chan School of Public Health, thinks something is going wrong in the gut, with many ASD children reporting gut problems, including diarrhoea, constipation, belching and excessive flatulence and dysbiosis indicated by an abnormal pattern of gut bacteria. (36)
Professor Fasano’s research finds that neurodivergent guts show high levels of zonulin, which can lead to leaky gut. (37) The gluten in wheat makes the zonulin levels go up.
Opioid-like wheat and milk proteins have been found in the urine samples of those with ASD, making these foods especially ‘addictive’. This was the discovery of researchers at the Autism Research Unit at the University of Sunderland, headed by Paul Shattock, now known as ESPA Research. They developed successful strategies for helping children with autism known as the Sunderland Protocol. (38)
—
The four drivers of ADHD
Optimum nutrition has a big role to play in helping ameliorate negative symptoms of neurodivergence.
Multi-nutrient trials have shown improvements in irritability, hyperactivity and self-harm in children with ADHD.(39) Raised homocysteine and low B12 or folate are associated with greater risk of developing ASD and worse symptoms, (40) creating methylation abnormalities that could explain many of the symptoms. (41) Supplementing homocysteine-lowering B vitamins makes symptoms better. (42)
So to summarise conditions like ADHD may be made worse or contributed to by:
A high-GL diet, with too much sugar
A lack of essential omega-3 fats
A lack of critical nutrients such as B vitamins, zinc and magnesium
Unidentified food intolerances (read more about how food intolerance can impact the brain here)
—
What you can do
For adults managing ADHD, a holistic approach that incorporates dietary changes and supplementation can be highly effective. Here are some strategies:
Feed your brain! The food you eat provides the ‘raw material’ for your brain and body. Focus on a diet rich in whole foods, including 3-5 portions of oily fish a week, nuts, seeds, leafy greens, and vegetables, to ensure adequate intake of essential nutrients.
Add in key nutrients. Consider supplementing with B-vitamins, zinc, magnesium, copper, chromium, and other essential nutrients to address deficiencies and support optimal brain function. Find out more about recommended supplements and dose requirements here
Test don’t guess. Test your vitamin D, omega-3, and sugar levels, along with your homocysteine, to get accurate data on what you need to focus on or supplement with.Find out more about the accurate, at-home tests here
Mindful Eating. Pay attention to food intolerances and adopt a low-glycemic load (low sugar) diet to stabilise blood sugar levels and improve cognitive function.
Complete the Cognitive Function test below to get personalised information on your area of risk and what you can do to mitigate them and upgrade your brain over the next 6 months..
Reclaim your brain so that your neurodivergence can serve and support you, and no longer create additional struggle in your life.
Thank you for reading!
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
References
1 Barkley RA. Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. New York: Guilford Press; 2010.
2 Kooij JJS, Bejerot S, Blackwell A, et al. European consensus statement on diagnosis and treatment of adult ADHD: The European Network Adult ADHD. BMC Psychiatry. 2010;10(1):67.
3 Asherson P, et al. Attention deficit hyperactivity disorder in adults: A review of the literature. Nat Rev Neurol. 2012;8(2):93-104.
4 Brown TE. Attention Deficit Disorder: The Unfocused Mind in Children and Adults. New Haven: Yale University Press; 2005.
5 Faraone SV, Biederman J, Mick E. The age-dependent decline of ADHD: A meta-analysis of follow-up studies. Psychol Med. 2006;36(2):159-165.
6 Willcutt EG, et al. Validity of DSM-IV attention deficit/hyperactivity disorder symptom dimensions and subtypes. J Abnorm Psychol. 2012;121(4):991.
7 Shaw P, et al. Emotion dysregulation in attention deficit hyperactivity disorder. Am J Psychiatry. 2014;171(3):276-293.
8 Surman CB, et al. Emotional dysregulation in adult ADHD and response to atomoxetine. J Atten Disord. 2011;15(5):354-368.
9 Quinn PO, Madhoo M. A review of attention-deficit/hyperactivity disorder in women and girls: Uncovering this hidden diagnosis. Prim Care Companion CNS Disord. 2014;16(3):PCC.13r01596.
10. Williamson D, Johnston C. Gender differences in adults with attention-deficit/hyperactivity disorder: A narrative review. Clin Psychol Rev. 2015;40:15-27.
11.Loo SK, et al. Cognition in girls with attention-deficit/hyperactivity disorder: Executive functions, emotion regulation, and comorbidity. J Am Acad Child Adolesc Psychiatry. 2008;47(3):262-274.
12 Babinski DE, et al. A meta-analysis of neuropsychological functioning in posttraumatic stress disorder. Arch Clin Neuropsychol. 2015;30(8):724-743.
13 Skogli EW, et al. Emotional lability in children and adolescents with attention deficit/hyperactivity disorder (ADHD): Clinical correlates and familial prevalence. J Affect Disord. 2013;145(2):241-249.
14 Grevet EH, et al. Gender differences in prevalence of symptoms of attention deficit and hyperactivity disorder in adults. Rev Bras Psiquiatr. 2005;27(1):21-24.
15 Solanto MV, et al. The prevalence of sluggish cognitive tempo in psychiatric outpatients with ADHD, anxiety, and mood disorders. J Atten Disord. 2017;21(8):666-674.
16 Hibbeln JR, Davis JM,] Steer C, Emmett P, Rogers I, Williams C, Golding J. Maternal seafood consumption in pregnancy and neurodevelopmental outcomes in childhood (ALSPAC study): an observational cohort study. Lancet. 2007 Feb 17;369(9561):578-85. doi: 10.1016/S0140-6736(07)60277-3. PMID: 17307104.
17 Z.Liu Behav Neurol. 2021 Dec 7;2021:5417497
18 Veena SR, Krishnaveni GV, Srinivasan K, Wills AK, Muthayya S, Kurpad AV, Yajnik CS, Fall CH. Higher maternal plasma folate but not vitamin B-12 concentrations during pregnancy are associated with better cognitive function scores in 9- to 10- year-old children in South India. J Nutr. 2010 May;140(5):1014-22. doi: 10.3945/jn.109.118075. Epub 2010 Mar 24. PMID: 20335637; PMCID: PMC3672847.
19. Qin B, Xun P, Jacobs DR Jr, Zhu N, Daviglus ML, Reis JP, Steffen LM, Van Horn L, Sidney S, He K. Intake of niacin, folate, vitamin B-6, and vitamin B-12 through young adulthood and cognitive function in midlife: the Coronary Artery Risk Development in Young Adults (CARDIA) study. Am J Clin Nutr. 2017 Oct;106(4):1032-1040. doi: 10.3945/ajcn.117.157834. Epub 2017 Aug 2. PMID: 28768650; PMCID: PMC5611785.
20 McNulty H, Rollins M, Cassidy T, Caffrey A, Marshall B, Dornan J, McLaughlin M, McNulty BA, Ward M, Strain JJ, Molloy AM, Lees-Murdock DJ, Walsh CP, Pentieva K. Effect of continued folic acid supplementation beyond the first trimester of pregnancy on cognitive performance in the child: a follow-up study from a randomized controlled trial (FASSTT Offspring Trial). BMC Med. 2019 Oct 31;17(1):196. doi: 10.1186/s12916-019-1432-4. PMID: 31672132; PMCID: PMC6823954.
21 Roigé-Castellví J, Murphy M, Fernández-Ballart J, Canals J. Moderately elevated preconception fasting plasma total homocysteine is a risk factor for psychological problems in childhood. Public Health Nutr. 2019 Jun;22(9):1615-1623. doi: 10.1017/S1368980018003610. Epub 2019 Jan 14. PMID: 30636652; PMCID: PMC10261079.
22 Montgomery P, Burton JR, Sewell RP, Spreckelsen TF, Richardson AJ. Low blood long chain omega-3 fatty acids in UK children are associated with poor cognitive performance and behavior: a cross-sectional analysis from the DOLAB study. PLoS One. 2013 Jun 24;8(6):e66697. doi: 10.1371/journal.pone.0066697. Erratum in: PLoS One. 2013;8(9). doi:10.1371/annotation/26c6b13f-b83a-4a3f-978a-c09d8ccf1ae2. PMID: 23826114; PMCID: PMC3691187.
23 Raine A, Ang RP, Choy O, Hibbeln JR, Ho RM, Lim CG, Lim-Ashworth NSJ, Ling S, Liu JCJ, Ooi YP, Tan YR, Fung DSS. Omega-3 (ω-3) and social skills interventions for reactive aggression and childhood externalizing behavior problems: a randomized, stratified, double-blind, placebo-controlled, factorial trial. Psychol Med. 2019 Jan;49(2):335-344. doi: 10.1017/S0033291718000983. Epub 2018 May 10. PMID: 29743128; see also Choy O, Raine A. Omega-3 Supplementation as a Dietary Intervention to Reduce Aggressive and Antisocial Behavior. Curr Psychiatry Rep. 2018 Apr 5;20(5):32. doi: 10.1007/s11920-018-0894-y. PMID: 29623453; see also Gow RV, Hibbeln JR. Omega-3 fatty acid and nutrient deficits in adverse neurodevelopment and childhood behaviors. Child Adolesc Psychiatr Clin N Am. 2014 Jul;23(3):555-90. doi: 10.1016/j.chc.2014.02.002. Epub 2014 May 27. PMID: 24975625; PMCID: PMC4175558.
24 Liu, J., Cui, Y., Li, L. et al. The mediating role of sleep in the fish consumption – cognitive functioning relationship: a cohort study. Sci Rep7, 17961 (2017). https://doi.org/10.1038/s41598-017-17520-w
25 Sonia L Robinson, Constanza Marín, Henry Oliveros, Mercedes Mora-Plazas, Betsy Lozoff, Eduardo Villamor, Vitamin D Deficiency in Middle Childhood Is Related to Behavior Problems in Adolescence, The Journal of Nutrition, Volume 150, Issue 1, 2020, pp.140–148, ISSN 0022-3166, https://doi.org/10.1093/jn/nxz185.
26 Jayedi A, Rashidy-Pour A, Shab-Bidar S. Vitamin D status and risk of dementia and Alzheimer’s disease: A dose-response meta-analysis. Nutr Neurosci. 2019 Nov;22(11):750-9. doi: 10.1080/1028415X.2018.1436639.
27 Chai B, Gao F, Wu R, Dong T, Gu C, Lin Q, et al. Vitamin D deficiency as a risk factor for dementia and Alzheimer’s disease: an updated meta-analysis. BMC Neurol. 2019 Nov 13;19(1):284. doi: 10.1186/s12883-019-1500-6.
28 Melo van Lent D, Egert S, Wolfsgruber S, Kleineidam L, Weinhold L, Wagner-Thelen H, et al. Low Serum Vitamin D Status Is Associated with Incident Alzheimer’s Dementia in the Oldest Old. Nutrients. 2023;15(1):61. https://doi.org/10.3390/nu15010061
29 Skalny AV, Mazaletskaya AL, Ajsuvakova OP, Bjørklund G, Skalnaya MG, Chao JC, Chernova LN, Shakieva RA, Kopylov PY, Skalny AA, Tinkov AA. Serum zinc, copper, zinc-to-copper ratio, and other essential elements and minerals in children with attention deficit/hyperactivity disorder (ADHD). J Trace Elem Med Biol. 2020 Mar;58:126445. doi: 10.1016/j.jtemb.2019.126445. PMID: 31869738.
31 Hemamy M, Pahlavani N, Amanollahi A, Islam SMS, McVicar J, Askari G, Malekahmadi M. The effect of vitamin D and magnesium supplementation on the mental health status of attention-deficit hyperactive children: a randomized controlled trial. BMC Pediatr. 2021 Apr 17;21(1):178. doi: 10.1186/s12887-021-02631-1. Erratum in: BMC Pediatr. 2021 May 12;21(1):230. PMID: 33865361; PMCID: PMC8052751.
32 B. Starobrat-Hermelin and T. Kozielec, ‘The effects of magnesium physiological supplementation on hyperactivity in children with attention deficit hyperactivity disorder (ADHD): Positive response to magnesium oral loading test’, Magnes Res, Vol 10(2), 1997, pp. 149-56
33 Farsad-Naeimi A, Asjodi F, Omidian M, Askari M, Nouri M, Pizarro AB, Daneshzad E. Sugar consumption, sugar sweetened beverages and Attention Deficit Hyperactivity Disorder: A systematic review and meta-analysis. Complement Ther Med. 2020 Sep;53:102512. doi: 10.1016/j.ctim.2020.102512. Epub 2020 Aug 16. PMID: 33066852.
34 Haghighatdoost F, Azadbakht L, Keshteli AH, Feinle-Bisset C, Daghaghzadeh H, Afshar H, Feizi A, Esmaillzadeh A, Adibi P. Glycemic index, glycemic load, and common psychological disorders. Am J Clin Nutr. 2016 Jan;103(1):201-9. doi: 10.3945/ajcn.114.105445. Epub 2015 Nov 25. PMID: 26607943.
35 Alick CL, Maguire RL, Murphy SK, Fuemmeler BF, Hoyo C, House JS. Periconceptional Maternal Diet Characterized by High Glycemic Loading Is Associated with Offspring Behavior in NEST. Nutrients. 2021 Sep 13;13(9):3180. doi: 10.3390/nu13093180. PMID: 34579057; PMCID: PMC8469715.
36 Needham BD, Adame MD, Serena G, Rose DR, Preston GM, Conrad MC, Campbell AS, Donabedian DH, Fasano A, Ashwood P, Mazmanian SK. Plasma and Fecal Metabolite Profiles in Autism Spectrum Disorder. Biol Psychiatry. 2021 Mar 1;89(5):451-462. doi: 10.1016/j.biopsych.2020.09.025. Epub 2020 Oct 10. PMID: 33342544; PMCID: PMC7867605.
37 Asbjornsdottir, Birna, et al. “Zonulin-dependent intestinal permeability in children diagnosed with mental disorders: a systematic review and meta-analysis.” Nutrients 12.7 (2020): 1982.
39 Mehl-Madrona L. Journal of Alternative and Complementary Medicine 2017 , 23(7), 526–533.
40 Li B, Xu Y, Pang D, Zhao Q, Zhang L, Li M, Li W, Duan G, Zhu C. Interrelation between homocysteine metabolism and the development of autism spectrum disorder in children. Front Mol Neurosci. 2022 Aug 15;15:947513. doi: 10.3389/fnmol.2022.947513. PMID: 36046711; PMCID: PMC9421079.
41 Antonio Belardo, Federica Gevi, Lello Zolla, The concomitant lower concentrations of vitamins B6, B9 and B12 may cause methylation deficiency in autistic children, The Journal of Nutritional Biochemistry, Volume 70, 2019, Pages 38-46, ISSN 0955-2863, https://doi.org/10.1016/j.jnutbio.2019.04.004; see also James SJ, Melnyk S, Fuchs G, Reid T, Jernigan S, Pavliv O, Hubanks A, Gaylor DW. Efficacy of methylcobalamin and folinic acid treatment on glutathione redox status in children with autism. Am J Clin Nutr. 2009 Jan;89(1):425-30. doi: 10.3945/ajcn.2008.26615. Epub 2008 Dec 3. PMID: 19056591; PMCID: PMC2647708.
42 Rossignol DA, Frye RE. The Effectiveness of Cobalamin (B12) Treatment for Autism Spectrum Disorder: A Systematic Review and Meta-Analysis. J Pers Med. 2021 Aug 11;11(8):784. doi: 10.3390/jpm11080784. PMID: 34442428; PMCID: PMC8400809; see also ref xx below; Adams JB, Audhya T, Geis E, Gehn E, Fimbres V, Pollard EL, Mitchell J, Ingram J, Hellmers R, Laake D, Matthews JS, Li K, Naviaux JC, Naviaux RK, Adams RL, Coleman DM, Quig DW. Comprehensive Nutritional and Dietary Intervention for Autism Spectrum Disorder-A Randomized, Controlled 12-Month Trial. Nutrients. 2018 Mar 17;10(3):369. doi: 10.3390/nu10030369. PMID: 29562612; PMCID: PMC5872787; see also James SJ, Melnyk S, Fuchs G, Reid T, Jernigan S, Pavliv O, Hubanks A, Gaylor DW. Efficacy of methylcobalamin and folinic acid treatment on glutathione redox status in children with autism. Am J Clin Nutr. 2009 Jan;89(1):425-30. doi: 10.3945/ajcn.2008.26615. Epub 2008 Dec 3. PMID: 19056591; PMCID: PMC2647708.
Written by Jerome Burne, see the original article at the Daily Mail here. Find out about Jerome here.
It is over 20 years since I discovered in my fifties that I have a copy of the gene, ApoE4, that’s been linked to a raised risk of Alzheimer’s.
—
It is over 20 years since I discovered in my fifties that I have a copy of the gene, ApoE4,that’s been linked to a raised risk of Alzheimer’s.
It’s the same gene that the actor Chris Hemsworth carries, although he has two copies, one from each of his parents – he learned this in 2022 after having tests for a documentary series he was making about longevity.
Now comes news of a major study that’s found that almost everyone who has two copies of this gene goes on to develop early signs of Alzheimer’s – researchers at the Sant Pau Research Institute in Barcelona looked at data from 10,000 people and 3,000 brain donors and found that the majority of those with two copies showed signs of Alzheimer’s by the time they reached the age of 55. The researchers estimate that around 2 percent of people have this gene profile.
My ApoE4 gene was identified when I was writing about the gene tests then just becoming publicly available, and as a health journalist I took one. It was an alarming discovery, since not only do I have no family history of Alzheimer’s, but back then there was nothing to be done about it, and for a while, common moments such as forgetting why I was peering into the fridge or a cupboard felt like a sinister warning.
But I quickly persuaded myself that any brain malfunction wouldn’t begin for years.
Anyway, a cure might come along any time and as a health journalist I could keep up with the latest research.
Yet for years there was little to be hopeful about – the few drugs that were available didn’t make a difference to the disease progression.
Small bits of cutting-edge research I came across here and there convinced me to try various lifestyle approaches (more on the specifics later), but the expectation has long been that once you’re heading into the medical territory that is Alzheimer’s, you need heavyweight pharmaceuticals.
But the cheering, and very surprising news, is that nutritional and lifestyle advice, with some additions and tweaks, is the very latest thing in Alzheimer’s prevention, with several UK charities and academic centres – including Imperial College, London, Exeter University, and Alzheimer’s Research UK – now actively investigating lifestyle.
What’s driving this dramatic U-turn is the failure of the drug industry to come up with effective and safe products. Even the newer ‘wonder’ drugs such as donanemab and lecanemab, which can delay the worsening of the disease by around a third in patients, can have serious side-effects – around a quarter of those who take them suffer bleeding or swelling in the brain, and some patients have experienced brain shrinkage.
These drugs work by clearing the brain of amyloid plaques – the sticky protein deposits thought to cause symptoms by disrupting communication between brain cells.
The problems with the latest drugs are detailed in a new book by leading neurologist Professor Karl Herrup, of Philadelphia University. In ‘How not to study a disease: The story of Alzheimer’s’ he writes: ‘In our rush to find a cure we have gone down a blind alley. For decades we have focused more on salesmanship than scholarship. The amyloid cascade hypothesis has become a steamroller, intent on crushing any alternative models.’
One problem is that having the plaque doesn’t necessarily mean you will have Alzheimer’s and not having it doesn’t mean you won’t.
As Professor Herrup points out, ‘we need to rebalance this amyloid hypothesis about the cause of Alzheimer’s to include other worthy ideas about its nature, such as those indicated by the links with diabetes and blood vessel damage and the insights gained from approaches involving diet, nutrition, and lifestyle’.
What’s so radical about the nutritional and lifestyle approach is that it doesn’t target a single cause but aims to improve the health of many of the body’s systems – such as metabolism (how energy is used), the immune system and the vast colony of bacteria and other microbes (the microbiome) in your guts, that have a two-way connection with the brain. Keeping them all healthy can do the same for the brain.
And it means we can all take steps to protect themselves, which is what I’ve tried to do.
I spoke to Tommy Woods, an Assistant Professor of neuroscience and paediatrics at the University of Washington, who is a principal investigator for the research charity, the Food for the Brain Foundation, which is looking at dementia amongst other brain disorders. The charity offers a free online test to both measure your cognitive function but also a questionnaire that works out your dementia risk. I did the test and it showed me exactly what, in my diet and lifestyle, was driving my risk.
He told me: ‘I first came across the idea of multiple approaches to health and fitness when I worked with athletes as a performance consultant. Many of the systems that affected their cognitive and physical abilities were the same as the ones we concentrate on at the charity with much older people.’
Robert Lustig, who is professor emeritus and an international expert on metabolism, based at the University of California San Francisco, explains why both blood sugar levels and insulin need to be kept at a low level to protect the brain.
Insulin’s job is to help the body use blood sugar (glucose) as fuel to clear it away into storage as fat. Professor Lustig, who is also advising the Food for Brain Foundation, says high levels of glucose – from a high carb diet – lead to higher levels of insulin. ‘Fairly soon, however, your system stops responding to insulin – known as insulin resistance – which is bad news because insulin delivers the glucose needed for energy in the brain and muscles.’
This is the kind of information that convinced me over the years to make changes to my diet.
The standard advice to have plenty of carbs and pick the low-fat option was reversed, and I started following a ketogenic diet that involves eating much more fat, mostly saturated and is very low in carbs.
The fat gets turned into small packets of energy, known as ketones, that can power brain cells.
I also started stepping up gym visits from a couple of times a week, to three or four. Exercise improves blood circulation which is needed to clear waste products from the brain.
I started paying attention to my microbiome – the colony of microbes that lives in the gut. This involved eating more fibrous vegetables, as well as making and drinking kefir – a fermented drink that delivers probiotics to the guts, every day.
And I started taking B vitamins.
A decade after my gene was spotted, a randomised trial at Oxford University, run by Professor Emeritus David Smith, showed that B vitamins were essential for clearing a toxic compound called homocysteine from blood.
Homocysteine comes from the breakdown of proteins, and can damage cells. High levels often found in the brains of Alzheimer’s patients.
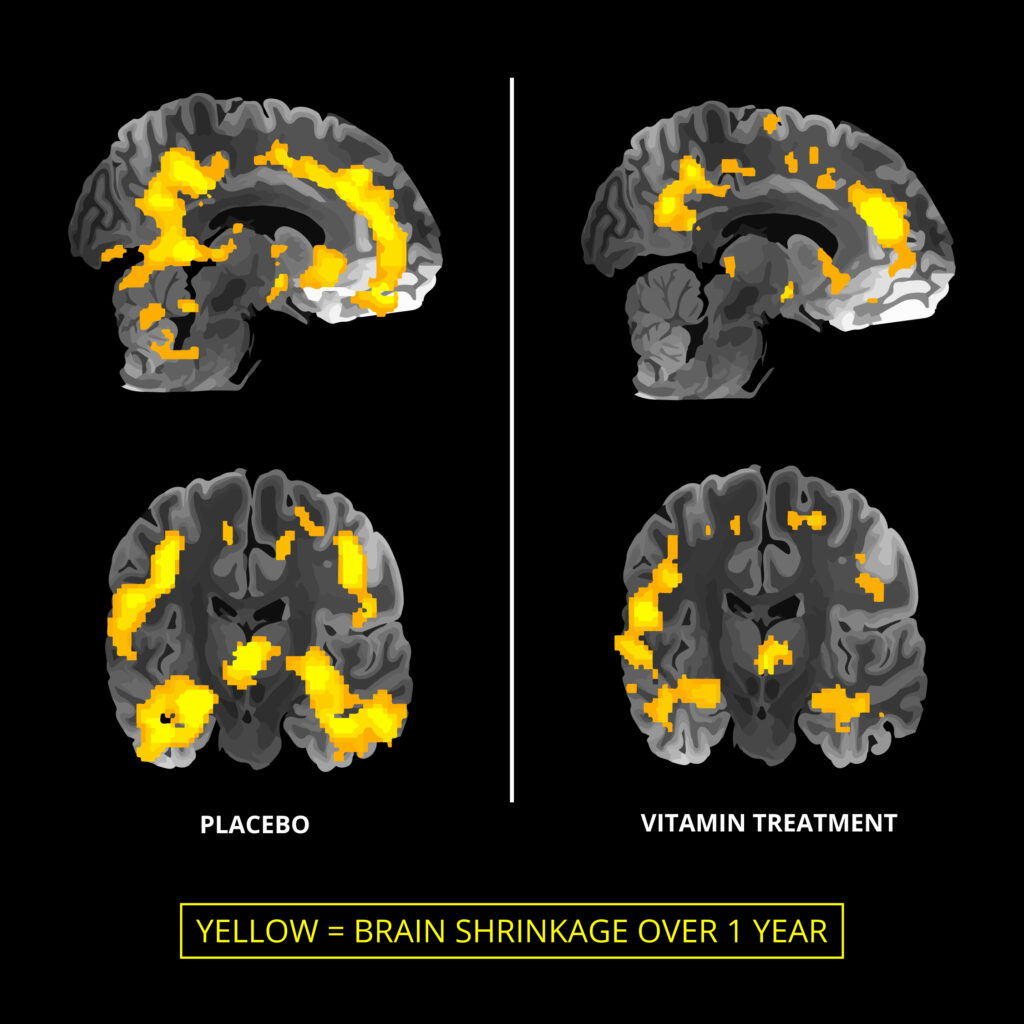
In the Oxford study, which involved over 200 people with mild cognitive impairment (MCI) – where memory and clear thinking are impaired – half were given a daily high dose of a B vitamin, the rest a placebo. A proportion of each group had a brain scan at the beginning end of the two-year trial.
The results, published in the journal PLOS One in September 2010, were impressive: those in the vitamin group not only had reduced homocysteine levels but brain shrinkage – the sign brain cell death – was half that of those in the placebo group.
Rather than being welcomed, however, the trial set off a long running academic battle. Alzheimer’s charities, including one that contributed funding, ignored it.
Another study which found no benefit from B vitamins was published four years later, but it didn’t convince me. While the participants in the Oxford trial had mild cognitive impairment, those in the later trials did not. So I kept taking the tablets.
One senior academic who has picked up on this research is Professor Peter Garrard, a specialist in neurodegenerative diseases such as Alzheimer’s, at St George’s Hospital in London.
When his mother Sheila started losing words and describing things in roundabout ways at the age of 78, he put her on a daily dose of high strength B vitamins.
‘It was very encouraging that despite having had a brain scan that showed significant cell damage, she didn’t get any worse and then gradually started doing a lot better,’ says Professor Garrard. Sheila died at the age of 89. ‘We’ll never know how long she would have lived without the vitamins, but it must have made a difference that she stayed very fit and active.’
Professor Garrard told me that he’d been impressed by the B vitamin research done at Oxford and regarded claims that the vitamins had no benefit inaccurate. ‘I check all my patient’s homocysteine levels and give them B vitamins if they are over the healthy level,’ he says.
Evidence for the benefit of B vitamins continued to mount, including in 2020, a review published by Professor Jin-Tai Yu from Fudan University in Shanghai, China’s leading Alzheimer’s prevention expert. Published in Journal of Neurology, Neurosurgery and Psychiatry, this analysed the results of 153 randomised trials and concluded that: ‘Homocysteine-lowering treatment seems the most promising intervention for Alzheimer’s disease prevention. ’ (The homocysteine-lowering treatment reviewed involved using folic acid (B9), vitamin B12 and vitamin B6).
As for me, I’m sanguine about the latest research about the ApoE4 gene: I’m currently feeling fit and well, thanks to a programme that seems a sensible way to stave off physical decline in general, and neurological decline in particular.
For more information and to reduce your risk you can:
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
Vitamin D: Your Brain’s Ally against Alzheimer’s and Dementia
Few people realise that vitamin D acts more like a brain fat than a vitamin – and your risk of cognitive decline can soar by up to 19 times if your levels are low. Often known as the sunshine vitamin, it is in fact a vital brain nutrient: helping neurons communicate, calming inflammation and defending against oxidative stress – all crucial for protecting memory, mood and long-term cognitive health. This highlights the important connection between vitamin D and dementia.
When vitamin D levels drop, the effects on the brain are striking.
Studies show that people with low vitamin D are far more likely to experience cognitive decline and dementia, while those with optimal levels have up to four times lower risk of developing Alzheimer’s disease. In older adults, falling vitamin D often mirrors worsening memory – yet the simple act of supplementing can reduce risk by a third. (That is why we offer our DRIfT at-home blood tests so you can know your levels are optimal and protect your brain.)
Read on to discover why optimising your vitamin D intake – and measuring it alongside other key brain biomarkers – could be one of the most powerful steps you can take to future-proof your brain.
Vitamin D and Dementia
Low vitamin D levels are significantly linked to a higher risk of dementia and cognitive decline. [1,2,3] One notable study carried out in France highlights an astonishing finding: older women with vitamin D deficiency were approximately 19 times more likely to develop dementia within seven years compared to those without vitamin D deficiency. [4] This research backs up several previous studies, including one that tracked 1,658 elderly adults for over five and a half years [5], concluding:
“Vitamin D deficiency is associated with a substantially increased risk of all-cause dementia and Alzheimer’s disease.”
Vitamin D Study: Our New Research
With more than 50 million people around the world affected by dementia, a figure forecast to triple by 2050, [6]) research into prevention is something that Food for the Brain takes seriously. Our Research Team is currently undertaking an independent study, commissioned by Dr William Grant, led by Tommy Wood, Assistant Professor at the University of Washington, Seattle, and supported by Simona Brucoli, data statistician. This research aims to contribute to the growing knowledge of the importance of Vitamin D in preserving brain health and staving off cognitive decline. More on this later in the year!
Understanding the Impact of Vitamin D on Overall Health
The impact of Vitamin D deficiency is a significant one, with links to not only dementia but also conditions such as osteoporosis, cardiovascular disease, cancer, stroke, diabetes, schizophrenia, psychosis, and autism [7], as well as behavioural problems in adolescents [8] and children with ADHD (9). Read more on how deficiency in Vitamin D impacts our overall health in our article here.
How to Sustain Optimal Vitamin D Levels
Of course, we can get vitamin D from our diet: oily fish, including salmon, mackerel, sardines, egg yolks, red meat, and liver, are all excellent sources. However, our bodies struggle to produce and maintain optimal vitamin D levels as we age, even with a good diet.
Our reliance on the sun, our natural provider of Vitamin D, is also compromised, especially in the Northern Hemisphere, as we begin to emerge from the long winter months and not, as yet, fully into the bright embrace of summer. It’s no wonder that our bodies are left vulnerable to notable decreases in vitamin D.
What Exactly is Vitamin D Deficiency?
Deficiency is defined as serum 25(OH)D concentrations of less than 50 nmol/L. Our vitamin D expert, Dr William Grant, says:
“All the evidence regarding cardio-metabolic diseases, cancer, diabetes, infectious diseases, and pregnancy outcomes shows that you need a blood level of vitamin D above 75 nmol/L to be healthy, and the same is proving true for the brain.”
This optimal level is impossible to achieve without supplementation in the winter. I recommend every adult and teenager supplements themselves with at least 1000 to 3000iu per day from October to March in line with a recent review by 35 vitamin D researchers. [10] The degree of obesity [11], darker skin colour [12] and living further North [13] increases need.
Supplementation: a Shield Against Risk?
According to recent research, turning to vitamin D supplements could reduce the risk of dementia. Researchers at the University of Calgary’s Hotchkiss Brain Institute in Canada and the University of Exeter in the UK explored the relationship between vitamin D supplementation and dementia in 12,388 participants with a mean age of 71. They were dementia-free when they signed up. Of the group, 37 percent (4,637) took vitamin D supplements. In the study, the team found that taking vitamin D was associated with living dementia-free for longer, and they also found 40 percent fewer dementia diagnoses in the group who took supplements. [10]
But How Do You Know if You’re Getting Enough Vitamin D?
The answer lies in taking a proactive step: testing your vitamin D levels.
Here at Food for the Brain, we don’t believe in guesswork. We champion the idea that we are all the architects of our own brain health and well-being. In the spirit of Citizen Scientists, we offer our accurate at-home blood tests so you can feel confident that you are protecting your mood, memory and future. Order your blood test here – available globally.
Awareness is the first step toward meaningful change. Discovering your vitamin D level is more than just informative; it’s a critical step toward optimising your cognitive and physical health.
Take Action: Protect and Future-Proof Your Brain
Share the knowledge.
Encourage your family and friends to check their brain health and vitamin D levels too – prevention starts with awareness.
Check your brain health for free.
Take our quick, scientifically validated Cognitive Function Test to see how your brain is performing right now. It’s free, is validated and gives you a personalised Dementia Risk Index and tailored advice.
Know your vitamin D and brain biomarker status.
Order our DRIfT 5-in-1 at-home blood test to measure the five key markers that matter most — Vitamin D, Homocysteine, HbA1c, Glutathione and Omega-3. Your results come with clear guidance on how to optimise each one.
Boost your vitamin D naturally.
Spend 15–20 minutes outdoors daily if you are in summer or live near the equator (without sunscreen on arms or legs, when the sun is high). Avoid peak sun times.
Eat oily fish twice a week – salmon, mackerel, sardines or trout.
Add egg yolks, mushrooms, and fortified dairy alternatives to your meals.
Supplement between 1,000–3,000 iu daily from October to March (and year-round if you have darker skin or live in northern latitudes). Find out more about supplementshere
Thank you for reading!
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
References
Jayedi A, Rashidy-Pour A, Shab-Bidar S. Vitamin D status and risk of dementia and Alzheimer’s disease: A dose-response meta-analysis. Nutr Neurosci. 2019 Nov;22(11):750-9. doi: 10.1080/1028415X.2018.1436639.
Chai B, Gao F, Wu R, Dong T, Gu C, Lin Q, et al. Vitamin D deficiency as a risk factor for dementia and Alzheimer’s disease: an updated meta-analysis. BMC Neurol. 2019 Nov 13;19(1):284. doi: 10.1186/s12883-019-1500-6.
Melo van Lent D, Egert S, Wolfsgruber S, Kleineidam L, Weinhold L, Wagner-Thelen H, et al. Low Serum Vitamin D Status Is Associated with Incident Alzheimer’s Dementia in the Oldest Old. Nutrients. 2023;15(1):61. https://doi.org/10.3390/nu15010061
Annweiler C, Rolland Y, Schott AM, Blain H, Vellas B, Beauchet O. Serum vitamin D deficiency as a predictor of incident non-Alzheimer dementias: a 7-year longitudinal study. Dement Geriatr Cogn Disord. 2011;32(4):273-8. doi: 10.1159/000334944.
Littlejohns TJ, Henley WE, Lang IA, Annweiler C, Beauchet O, Chaves PH, et al. Vitamin D and the risk of dementia and Alzheimer’s disease. Neurology. 2014 Sep 2;83(10):920-8. doi: 10.1212/WNL.0000000000000755.
Gauthier S, Rosa-Neto P, Morais JA, Webster C. World Alzheimer Report 2021: Journey Through the Diagnosis of Dementia. Alzheimer’s Disease International; 2021.
Anjum I, Jaffery SS, Fayyaz M, Samoo Z, Anjum S. The Role of Vitamin D in Brain Health: A Mini Literature Review. Cureus. 2018 Jul 10;10(7):e2960. doi: 10.7759/cureus.2960.
Robinson SL, Marín C, Oliveros H, Mora-Plazas M, Lozoff B, Villamor E. Vitamin D Deficiency in Middle Childhood Is Related to Behavior Problems in Adolescence. J Nutr. 2020;150(1):140-8. https://doi.org/10.1093/jn/nxz185.
Hemamy M, Pahlavani N, Amanollahi A, Islam SMS, McVicar J, Askari G, et al. The effect of vitamin D and magnesium supplementation on the mental health status of attention-deficit hyperactive children: a randomized controlled trial. BMC Pediatr. 2021 Apr 17;21(1):178. doi: 10.1186/s12887-021-02631-1.
Ghahremani M, Smith EE, Chen HY, Creese B, Goodarzi Z, Ismail Z. Vitamin D supplementation and incident dementia: Effects of sex, APOE, and baseline cognitive status. Alzheimers Dement (Amst). 2023 Mar 1;15(1):e12404. doi: 10.1002/dad2.12404. PMID: 36874594; PMCID: PMC9976297.
Ekwaru JP et al The importance of body weight for the dose response relationship of oral vitamin D supplementation and serum 25-hydroxyvitamin D in healthy volunteers. PLoS One. 2014 Nov 5;9(11):e111265. doi: 10.1371/journal.pone.0111265. PMID: 25372709; PMCID: PMC4220998.
Ames BN, Grant WB, Willett WC. Does the High Prevalence of Vitamin D Deficiency in African Americans Contribute to Health Disparities? Nutrients. 2021 Feb 3;13(2):499. doi: 10.3390/nu13020499. PMID: 33546262; PMCID: PMC7913332.
Engelsen O. The relationship between ultraviolet radiation exposure and vitamin D status. Nutrients. 2010 May;2(5):482-95. doi: 10.3390/nu2050482. Epub 2010 May 4. PMID: 22254036; PMCID: PMC3257661.
We often get asked if supplements are necessary, usually in relation to some expert or opinion leader saying they are a waste of money or have no evidence of effect.
Anyone actively discouraging supplementation of vitamin B, C, D or omega-3, or claiming there is no scientific evidence to support their use, are both scientifically inaccurate and, perhaps inadvertently, driving more people towards dementia and Alzheimer’s by increasing their risk of cognitive decline.
—
Here is why
B vitamin supplements – Two in five people over 60 in the UK and more than half in the US have raised homocysteine levels and accelerated brain shrinkage as a result and need to supplement high dose B12 (500mcg) to reduce the rate of brain shrinkage. This may be due to poor absorption and is not achievable by diet alone. Find out more about this here.
—
Omega-3 fish oil supplements – Those with higher omega-3 intake, both from food and supplements, have substantially reduced risk from UK BioBank data. Those with higher omega-3 index levels, which we test at Food for the Brain, have more brain mass, and even healthy, young people supplementing omega-3 have cognitive improvements. You can see the published scientific evidence for this here.
Vitamin D supplements– Those who have higher vitamin D levels or supplement vitamin D also have substantially reduced risk of cognitive decline. Find out more here but also we’ll be publishing a full report on vitamin D and dementia in the next two weeks.
—
Vitamin C and E supplements – according to the most comprehensive review of studies relating to Alzheimer’s prevention ‘‘either a high vitamin E or C intake showed a trend of attenuating risk by about 26 per cent’, making these nutrients ‘grade 1’ top level prevention’. Inadequate vitamin C status in otherwise healthy young adults is related to a low level of mental vitality. In a randomised controlled trial vitamin C supplementation effectively increased work motivation and attentional focus and contributed to better performance on cognitive tasks requiring sustained attention. These brain-friendly effects of vitamin C relate to the supplementation of 1 gram or more a day. See the scientific aevidence for antioxidants here.
In addition to exploring the links to the evidence above, these articles further explain the role of B vitamins, Omega-3, Vitamin D, Vitamin C, E and other antioxidants.
At Food for the Brain, where prevention is better than cure, we report the science, based on the research, which tells us the opposite.
—
Thank you for reading!
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
In 2000 I wrote a book, The H Factor, with a byline ‘the biggest health breakthrough of the century’. It was the year 2000 so there wasn’t so much competition! However, it is now 2024 and this statement is even more true now than then.
Not glucose, not cholesterol, not even a gene test.
“The commonest associations are with cardiovascular diseases and diseases of the central nervous system (eg. your brain and nerves), but a large number of developmental and age-related conditions are also associated.” Says Professor Helga Refsum who, more than any other, put homocysteine on the map.
Those conditions that affect the brain include age-related cognitive decline to Alzheimer’s; depression to anxiety; bipolar to schizophrenia; and migraines to macular degeneration. Macular degeneration affects the eyes, not the brain but the eyes are the outwards extension of the brain – literally the visual interface between the world and your brain. Hearing loss is another disease predicted by raised blood (plasma) homocysteine. Then there are strokes affecting the blood’s circulation in your brain. Children with autism have higher levels. It also predicts problems in pregnancy. (Read more about this here)
“Five diseases can at least in part be prevented by lowering total homocysteine: neural tube defects, impaired childhood cognition, macular degeneration, primary stroke, and cognitive impairment (which means dementia and Alzheimer’s) in the elderly,” conservatively conclude Professors Refsum and David Smith, our ‘homocysteine and B vitamin’ expert on our Scientific Advisory Board.
—
The brain health imperative…
Two studies illustrate the predictive power of homocysteine; one showed that 2/3rd of heart attacks and strokes in older people could be predicted, not by cholesterol, but by homocysteine (1). The other is that you can predict a child’s school grades by knowing their homocysteine level, according to a study in a Swedish school, averaging a child’s school grades and comparing them to both homocysteine and B vitamin status (2).
But there are two other reasons why knowing your homocysteine level is a brain health imperative.
The first is that you can’t ‘see’ it or predict it just by knowing a person’s diet or lifestyle.
The second is that it is easily lowered with B vitamins.
More important than your APOE4 status
A lot of people want to know if they have the ApoE4 gene. Statistically, it increases your risk of developing Alzheimer’s by about 5 per cent. While you can mitigate its effects by improving your diet and lifestyle you can’t change the fact that you’ve got it.
The extent to which a raised homocysteine level (above 11mcmol/l) increases your risk of cognitive decline is illustrated by two studies. One shows that having a high level raises risk by 10 times (3). Another shows double the rate of brain shrinkage between those in the top quarter of homocysteine versus the bottom quarter (4). Different studies show different ‘predictive power’ but it is certainly more important than your ApoE4 status.
The other reason it is important to know your level is illustrated by the story of a mother and daughter who attended one of my lectures. Hearing about the strong link to strokes, which the mother had had, the daughter said “Mum, I really think you should have the test.” In fact they both did. The mother’s result was a healthy 6 mcmol/l while the daughter’s was extremely raised, above 20 mcmol/l. She had chronic fatigue. A month later, having taken a homocysteine-lowering supplement, her level was normal – and her chronic fatigue had gone.
—
Homocysteine is not just about what you eat
So, you can’t just assume your level is OK.
In fact, about half of those over 65 (my age) have a raised homocysteine level. Why? This is not an easy answer because there are many ‘lifestyle’ associations – from smoking to stress. Vegans who don’t supplement vitamin B12 would also be at risk. Since vitamin B6, folate and B12 are key to lowering homocysteine one’s intake of these nutrients, eg. from foods such as greens, beans and fish, is also very relevant but…it isn’t just a dietary marker.
The big unknown is that some people, especially as they age, absorb vitamin B12 poorly. This requires stomach secretions. Some people inherit this deficit and are diagnosed with pernicious anaemia, others acquire it with age. Either way, the net result is only ‘clinically’ shown by measuring homocysteine.
Homocysteine is called a ‘functional’ test because it indicates whether or not a person can do ‘methylation’. Methylation is a vital second-by-second chemical balancing act that the body and brain use to micro-adjust everything from making insulin, serotonin, and adrenalin or turning gene expression up or down, to repairing DNA and detoxifying all sorts of things in the liver, from histamine to mercury. Knowing your B12, folate or B6 status isn’t as good as knowing if you are or aren’t a healthy ‘methylator’. Homocysteine is the gold standard test for this.
An analogy here is a single-pin prick glucose test will only show you if, in that moment, your blood sugar level is too high. However, HbA1c (glycosylated haemoglobin) shows you both whether your blood sugar levels are damaging cells and gives you an ‘average’ of 3 month’s worth of glucose levels. Thus, we also call HbA1c a ‘functional’ test.
Knowing your levels of these is so important which is why we have created DRIfT (Dementia Risk Index functional Test) so that you know exactly where you are at and how to reduce your risk of not just dementia but over 100 other diseases.
This is one of the most important brain health tests you can do (and thankfully due to new technology you can do it accurately and easily with a simple pinprick at-home test)
Buy the DRIfT 4 in 1 test to check your homocysteine, Vitamin D, HbA1c (sugar) and Omega-3 status and for the biggest savings.
Remember every test kit you order will not only help you upgrade your brain it will also help us in our vital research – you will become a part of our ‘Citizen Science’ team and be donating to our wider charitable work and research. Thank you!
Thank you for reading!
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
1 W. de Ruijter, et al., ‘Use of Framingham risk score and new biomarkers to predict cardiovascular mortality in older people: Population based observational cohort study’, British Medical Journal, 2009 Jan;338:a3083
2 https://pubmed.ncbi.nlm.nih.gov/21746721/
3 10.3389/fnagi.2022.868777
4 Smith AD, Smith SM, de Jager CA, Whitbread P, Johnston C, Agacinski G, Oulhaj A, Bradley KM, Jacoby R, Refsum H. Homocysteine-lowering by B vitamins slows the rate of accelerated brain atrophy in mild cognitive impairment: a randomized controlled trial. PLoS One. 2010 Sep 8;5(9):e12244. doi: 10.1371/journal.pone.0012244. PMID: 20838622; PMCID: PMC2935890.
Parkinson’s affects 120,000 people in the UK, both young and old.
—
Parkinson’s affects 120,000 people in the UK, both young and old.
A recent review from the NCBI in the US (1) on Parkinson’s disease begins with the following:
‘Parkinson’s disease (PD) is a common neurodegenerative disease for which there is no treatment modifying the course of the disorder and no reliable biomarkers for early diagnosis. (2) In just 26 years, the number of PD patients around the world has more than doubled. (3) A relatively conservative prediction model shows that it is expected that there will be 12 million PD patients in the world by 2050.’
Thus, early detection and timely intervention of PD appear to be particularly important.
Thanks to the pioneering work of Dr Geoffrey Leader and Lucille Leader, a doctor and nutritionist living in London, we now know that the right nutritional intervention can effectively support the symptoms of Parkinson’s disease.
—
Parkinson’s and Dopamine
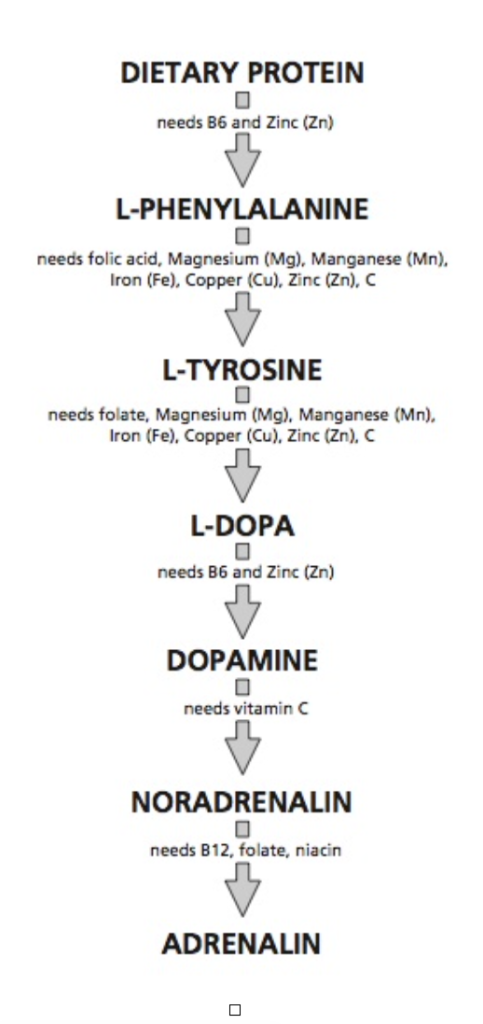
Dopamine is a neurotransmitter (chemical messenger) found within the brain. It has a variety of influences on brain function including playing a role in regulation. (Fig 1) [4]
Figure 1
There is little doubt that dopamine deficiency is the major cause of the symptoms of Parkinson’s, and most drug therapy aims to improve the body’s ability to make dopamine from L-dopa. But, why do some people develop this impaired ability to make this key neurotransmitter?
There are many answers to this question.
In some cases the neurons that produce dopamine don’t work properly, sometimes because they lack the raw materials, or the enzymes that turn on the building blocks, amino acids. (Amino acids are commonly known as the building blocks of protein. There are 20 standard amino acids from which almost all proteins are made.) The neurons can die off or be damaged, for example by oxidants, or by environmental toxins such as pesticides and herbicides.
Interestingly, researchers at the University of Miami have found levels of these chemicals to be higher in the brains of Parkinson’s sufferers.[5] The incidence of Parkinson’s is notably higher in rural areas where a lot of crop spraying takes place, and some pesticide combinations have shown a clear geographical correlation with incidences of the disease.[6,7]
Deficiency of nutrients such as folate which is critical during pregnancy for the development of a baby’s brain and nerves and also essential for brain and nerve function, play a part, making these dopamine-producing brain cells more susceptible to damage.[8]
—
The Homocysteine Connection
The balance of neurotransmitters, including dopamine, is controlled to a large extent by the process of methylation. (Methylation is what occurs when the body takes one substance and turns it into another, so that it can be detoxified and excreted from the liver.)
Most people with Parkinson’s have raised homocysteine levels. [9] Homocysteine is an amino acid found in the blood. Elevated levels of homocysteine have been associated with narrowing and hardening of the arteries and an increased level indicates disrupted methylation patterns. The latest review [10] states that “Homocysteine is linked with the occurrence and progression of Parkinson’s. This review briefly discussed the structure of Hcy, the metabolism of Hcy, and the mechanism of HHcy in PD. There are many disputes about the relationship between HHcy and PD which remain to be investigated. It also remains to be examined whether homocysteine is a causative agent or marker of damage.” Additionally,treatment with L-dopa medication tends to raise homocysteine levels.[11]
Either way, testing for homocysteine and supplementing homocysteine-lowering nutrients accordingly would be a recommendation. Buy your test kit here.
—
Parkinsons & Nutrition
In addition to faulty methylation, sometimes there is a problem in how the body detoxifies, a job primarily done by the liver, leaving neurons unprotected.[12] Then there are other factors such as prolonged stress and the likelihood of genetic predispositions. Geoffrey and Lucille Leader figured that each of these pieces of the jigsaw puzzle could be made a lot better if sufferers followed a targeted optimum nutrition programme. They started to test patients with Parkinson’s disease and found that literally 100 percent of them had nutritional deficiencies based on tests that measure what is going on within cells. They also found that many were deficient in stomach acid and digestive enzymes. Digestive enzymes break down carbohydrates, fats and proteins into their smallest components, allowing them to be absorbed by the body. Examples of deficient digestive enzymes might look like poor digestion, and increased intestinal permeability, leading to faulty absorption of nutrients.
Intestinal permeability is easily tested by drinking a solution that shouldn’t pass through the gut wall, and then measuring urinary levels. Using such a test, people with Parkinson’s disease may often show an increase in gut permeability or evidence of malabsorption. While there is no conclusive evidence yet that Parkinson’s disease is caused by nutrient deficiencies, the Leaders have found that correcting these deficiencies often helps.
—
Brain Toxins, Oxidants and the Liver
All this faulty digestion and absorption places extra stress on the liver, the detoxification capital of the body. Since the brain’s neurons can’t protect themselves from toxins, they depend on the liver. A simple example of this is alcohol – once you drink more than your liver can detoxify, you get drunk, which is what happens when brain cells are exposed to this toxin. In excess, you lose muscular control and movements, including speech, slow down.
Problems with liver detoxification are often a hallmark of Parkinson’s patients.
One of the liver’s best detox allies are the sulphur-containing amino acids, which have the ability to mop up undesirable toxins in a process called sulphation. Researchers have reported faulty sulphation in patients with Parkinson’s, which can be helped by supplementing cysteine, methionine and molybdenum. These can help rid the body of protein breakdown products, strengthen teeth and may help reduce the risk of tooth decay [13] .
Avoiding wine, coffee, certain cheeses and chocolate, all known inhibitors of sulphation [12] and eating foods rich in glucosinolates, such as broccoli, brussel sprouts, cabbage, cauliflower and kale, also help the liver to detoxify.
The greatest toxins of all are oxidants, or ‘free-radicals’. Giving antioxidants helps to prevent free radical damage to brain cells and slows the progression of the disease.
In a 7-year pilot study, 21 patients with early Parkinson’s were given 3,000mg of vitamin C and 3,200iu of vitamin E daily. The need for drug therapy was delayed up to two to three years compared to those who did not receive the antioxidants.[14]
Along with its negative effect on neurons, Parkinson’s also damages function in the mitochondria, which are the energy factories in our cells where energy conversion takes place. One of the most critical antioxidants for protecting mitochondria is coenzyme Q10 (CoQ10). The older you are, the more likely you are to be deficient.
These nutrients are some but by no means all of the allies that can support liver function, thereby preventing brain damage from toxins.. Dr Jeffrey Bland from Gig Harbor, Washington, an expert in liver detoxification, has also found tremendous improvement by supporting liver function with nutritional supplementation, increasing the effectiveness of drugs, reducing symptoms and boosting energy levels in those suffering from the early stages of Parkinson’s in studies.[15]
As detoxification may be compromised in Parkinson’s Disease, as is demonstrated by tests and clinical experience, personal clinical experience demonstrates that it is best to clean up the diet very gradually and recommend nutrients which support detoxification pathways.
—
Personalised Nutrition Works Best
The Leaders have found the best approach involves a tailor-made nutritional programme of diet and supplements and have found that this may often reduce symptoms and make drugs more effective, thus optimising dosage.
They recommend appropriate supplements based on patients’ biochemical individuality, including vitamins, minerals, essential fats, amino acids, antioxidants, phospholipids and brain-friendly herbs, providing that there are no contraindications for the administration of any herbs or nutrients for daily use, or in preparation or recovery from surgery.
As with so many mental health problems, controlling blood sugar and checking and correcting food allergies or intolerances can make a big difference. The most common allergy-provoking foods are the gluten grains (especially wheat, but also rye, oats, barley and spelt) and dairy products. Managing stress is also important because we respond to stress by producing the stress hormones noradrenalin and adrenalin, which are made from dopamine. This is why the symptoms of Parkinson’s often get worse when the sufferer is stressed.
—
Working with Medication: What to Eat
The right diet is very important in tackling every piece of the jigsaw of Parkinson’s. Movement problems can get worse when dense proteins are eaten too close to the times of taking L-dopa medication.[16] This is because L-dopa competes with the amino acids for absorption at the receptor sites in the intestine and at the blood-brain barrier, so less gets through.
To make best use of the L-dopa, protein-rich foods containing the other amino acids should not be eaten at the same time as taking L-dopa medication, according to the following guidelines:
L-dopa medication and diet – what to eat when*
L-dopa is affected by protein-containing foods which contain significant amounts of the amino acids: tyrosine, phenylalanine, valine, leucine, isoleucine, tryptophan, methionine and histidine. Foods which contain these amino acids include eggs, fish, meat, poultry, dairy produce (not butter), pulses, green peas, spinach, sago, soy, couscous, bulgar, coconut, avocado, asparagus and gluten-containing grains (oats, rye, wheat, barley, spelt).
Take L-dopa medication. Wait ONE HOUR or until the drug takes effect before eating any of the foods listed above.
After eating any of the foods listed above, wait TWO HOURS, if possible, before taking L-dopa medication again if it is needed.
*This dietary protocol has been developed and proven helpful by Dr Geoffrey and Lucille Leader and is reproduced with their kind permission. (Their book, Parkinson’s Disease Optimising ON-OFF Periods during L-dopa Therapy www.denorpress.com) provides all the monitoring forms for patients and medical professions in order to assess more precise timing and dosage of administration – diet and metabolic pathways also presented.
Some people are more susceptible to this dose-dependent side-effect than others, and few react at a dose of 10mg, which is commonly given for Parkinson’s.[15]
While being careful to avoid these foods around medication, it is important to get enough protein from foods at other times. Good whole proteins include fish and eggs. Many people choose to have their meal containing concentrated protein at night. This is because they do not need as much help with movement control at night as during the day when their L-dopa medication is necessary to see them through all their activities. Some people leave out L-dopa completely after the protein meal. Otherwise, it is best to follow the time protocol for taking L-dopa with a protein-rich meal, as above.
It is also important to have a well-balanced diet throughout the day including fruits and vegetables, gluten-free wholegrains and plenty of fluids. A common problem in Parkinson’s is constipation. Having a diet rich in fruits and vegetables and drinking plenty of water throughout the day makes a big difference, as can a few prunes, figs or dried apricots between meals with water. There are also special fibres, such as glucomannan, which help relieve constipation.
What to do:
Attend our ‘Optimising Parkinson’s’ Webinar – sign up here
See a nutritional therapist or doctor who can assess you for nutritional deficiencies, digestive problems and liver function.
Pursue a tailor-made nutritional strategy, including a specific diet regime that maximises the effects of any medication.
Avoid environmental toxins and eat organic when possible.
Thank you for reading!
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
2 Surguchov A. In: Peplow PV, Martinez B, Gennarelli TA, eds. Neurodegenerative Diseases Biomarkers: Towards Translating Research to ClinicalPractice. Springer US; 2022:155-180.
3 GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990–2016: a systematic anal- ysis for the global burden of disease study 2016. Lancet Neurol. 2019;18:459-480. doi:10.1016/S1474-4422(18)30499-X
4 V.L. Davidson and D.B. Sittman, Biochemistry: The National Medical Series for Independent Study, Harawl Publishing (1994), pp.477-8
5. L. Fleming et al., ‘Parkinsons’ disease and brain levels of organochlorine pesticides’, Ann Neurol, Vol 36(1), 1994, pp.100-3
6. M. Thiruchevlvam et al., ‘The Nigrostriatal Dopaminergic System as a preferential target of repeated exposures to combined paraquat and maneb: implications for Parkinson’s Disease’, Journal of Neuroscience, Vol 20(24), 2000, pp.9207-14 and J. Corell et al., ‘The risk of Parkinson’s disease with exposure to pesticides, farming, well water and rural living’, Neurology, Vol 67, 1998, pp.1210-18
7. L. Leader, Parkinson’s Disease – The Way Forward, Denor Press (2000), p.77
8. W. Duan et al., ‘Dietary folate deficiency and elevated homocysteine levels endanger dopaminergic neurons in models of Parkinson’s Disease’, J Neurochemistry, vol 80, 2002, pp.101-10
9. Zhou L. Homocysteine and Parkinson’s disease. CNS Neurosci Ther. 2024 Feb;30(2):e14420. doi: 10.1111/cns.14420. Epub 2023 Aug 29. PMID: 37641911; PMCID: PMC10848096; see also
10. Zhou L. Homocysteine and Parkinson’s disease. CNS Neurosci Ther. 2024 Feb;30(2):e14420. doi: 10.1111/cns.14420. Epub 2023 Aug 29. PMID: 37641911; PMCID: PMC10848096; see also
11.R.B. Postuma et al., ‘Vitamins and entacapone in levodopa-induced hyperhomocysteinemia: A randomized controlled study’, Neurology, Vol 66(12), 2006, pp. 1941-3
12. L. M. de Lau et al., ‘Dietary folate, vitamin B12, and vitamin B6 and the risk of Parkinson’s disease’, Neurology, Vol 67(2), 2006, pp. 315-8
13. G.B. Steventon et al., ‘Plasma cysteine and sulphate levels in patients with motor neurone, Parkinson’s and Alzheimer’s Disease’, Neurosci Letts, Vol 110, 1990, pp.216-20
14. S. Fahn, ‘A pilot trial of high dose alpha-tocopherol and ascorbate in early Parkinson’s Disease’, Ann Neurol, Vol 32(S), 1992, pp.128-32
15. J.S. Bland and J.A. Bralley, ‘Nutritional upregulation of hepatic detoxification enzymes’, J Applied Nutrition, Vol 4, 1992, pp.3-15
16. R.B. D’Agostino et al., ‘Plasma homocysteine as a risk factor for dementia and Alzheimer’s disease’, N Engl J Med, Vol 346(7), 2002, pp. 476-83
Are You Wasting Money On Your Omega-3 Supplements?
Are You Wasting Money On Your Omega-3 Supplements?
Omega-3 supplements are becoming increasingly popular – and rightly so – as another recent UK BioBank study (1) reported a 30% lower risk of dementia in those with higher omega-3 status in their blood.
Another study (2) found a 49% reduced risk for dementia in those with the highest omega-3 DHA level (top fifth) in their red blood cells compared with those having the lowest (bottom fifth).
Oily fish and fish oil supplements contain two types of omega-3 fat, called DHA and EPA. DHA is the main fat found in the brain cells of all animals. What’s more, your omega-3 index predicts both your brain size and cognitive abilities, according to this study (3) from Loma Linda University (featured in the Blue Zones film), so you might want to check that you’re above 8%.
The Benefits Go Beyond Preventing Dementia.
A person’s omega-3 index, which is a composite score of both EPA and DHA bound into red blood cell membranes, predicts both the risk of depression (4) and poorer reading ability, lower IQ, worse memory, sleep difficulties as well as aggression and emotional instability in children – hallmarks of ADHD (5).
It also predicts the risk of heart disease (6) and developmental problems in babies, based on measures taken in women both before and during pregnancy. Pregnant women with a higher omega-3 index have a much lower likelihood of having a baby with developmental problems, according to research from Imperial College London Institute of Brain Chemistry at the Chelsea & Westminster Hospital campus.
The Missing Piece…
However, omega-3s do not act alone. To become biologically active, DHA must be attached to phospholipids – a process entirely dependent on methylation. This, in turn, requires adequate levels of B vitamins: B6, folate, and B12.
A landmark study (7) concluded that the combination of B vitamins and fatty acids improves cognitive function. This is because, during methylation, DHA attaches to a phospholipid, enabling it to be incorporated into the neuronal membrane of the brain. The process of methylation is entirely dependent on vitamins B6, B12, and folate. When omega-3 and B vitamin status are both sufficient, the brain can build new, functional neuronal membranes – literally the structural basis of thought.
So, you need both a high omega-3 status (over 8%) and adequate B vitamins to incorporate DHA into the brain. You can be confident that methylation is working properly if your homocysteine level is below 11 µmol/L. In a large omega-3 study, people with early-stage dementia were given 2.3 grams a day (equivalent to two large fish oil capsules), but only those with lower homocysteine levels benefited (7).
Having a raised homocysteine level, above 11mcmol/L, is extremely common. In the US around 40% of people over the age of 60 have elevated levels. This is often due to poor absorption of vitamin B12 and may require high-dose supplementation to normalise homocysteine. (Read more about homocysteine here.)
Why Testing is Essential
This means two things are critical for protecting your brain:
A high omega-3 index – ideally over 8%.
A low homocysteine level – ideally below 11µmol/L, with the optimal level being around 7 µmol/L
If either is lacking, the protective effect is lost. Taking fish oils without ensuring good B vitamin status will not deliver full benefit – and vice versa.
That is why testing both is essential for protecting your brain.
To make this simple, Food for the Brain has launched the DRIFt 5-in-1 home test – a quick pinprick blood test you can do yourself. It measures:
Omega-3 Index – how much brain-building DHA and EPA are in your cells
Homocysteine – the key methylation marker, linked to brain shrinkage
Vitamin D – vital for brain health, mood, and immunity
HbA1c – the gold-standard measure of blood sugar balance
Omega-6:3 Ratio – shows whether you’re getting the right fats for your brain
Together, these five markers account for more than half of the modifiable risk for Alzheimer’s disease and dementia.
By testing these markers, you will know exactly what to supplement and what to change in order to protect your brain. And by joining the DRIFt study, you will also become a Citizen Scientist, helping to advance dementia prevention research worldwide.
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
References
1 Sala-Vila, A.; Tintle, N.; Westra, J.; Harris, W.S. Plasma Omega-3 Fatty Acids and Risk for Incident Dementia in the UK Biobank Study: A Closer Look. Nutrients 2023, 15,4896. https://doi.org/10.3390/ nu15234896
2 Sala-Vila, A.; Satizabal, C.L.; Tintle, N.; Melo van Lent, D.; Vasan, R.S.; Beiser, A.S.; Seshadri, S.; Harris, W.S. Red Blood Cell DHA Is Inversely Associated with Risk of Incident Alzheimer’s Disease and All-Cause Dementia: Framingham Offspring Study. Nutrients 2022, 14, 2408. https://doi.org/10.3390/ nu14122408
4 Yonezawa K, Kusumoto Y, Kanchi N, Kinoshita H, Kanegae S, Yamaguchi N, Ozawa H. Recent trends in mental illness and omega-3 fatty acids. J Neural Transm (Vienna). 2020 Nov;127(11):1491-1499. doi: 10.1007/s00702-020-02212-z. Epub 2020 May 25. PMID: 32451632.
5 Montgomery P, Burton JR, Sewell RP, Spreckelsen TF, Richardson AJ. Low blood long chain omega-3 fatty acids in UK children are associated with poor cognitive performance and behavior: a cross-sectional analysis from the DOLAB study. PLoS One. 2013 Jun 24;8(6):e66697. doi: 10.1371/journal.pone.0066697. Erratum in: PLoS One. 2013;8(9).doi:10.1371/annotation/26c6b13f-b83a-4a3f-978a-c09d8ccf1ae2. PMID: 23826114; PMCID: PMC3691187; see also Raine A, Ang RP, Choy O, Hibbeln JR, Ho RM, Lim CG, Lim-Ashworth NSJ, Ling S, Liu JCJ, Ooi YP, Tan YR, Fung DSS. Omega-3 (ω-3) and social skills interventions for reactive aggression and childhood externalizing behavior problems: a randomized, stratified, double-blind, placebo-controlled, factorial trial. Psychol Med. 2019 Jan;49(2):335-344. Doi 10.1007/s11920-018-0894-y. PMID: 29623453. ; see also Liu, J., Cui, Y., Li, L. et al. The mediating role of sleep in the fish consumption – cognitive functioning relationship: a cohort study. Sci Rep 7, 17961 (2017). https://doi.org/10.1038/s41598-017-17520-w
6 Gutierrez L, Folch A, Rojas M, Cantero JL, Atienza M, Folch J, Camins A, Ruiz A, Papandreou C, Bulló M. Effects of Nutrition on Cognitive Function in Adults with or without Cognitive Impairment: A Systematic Review of Randomized Controlled Clinical Trials. Nutrients. 2021 Oct 22;13(11):3728. doi: 10.3390/nu13113728. PMID: 34835984; PMCID: PMC8621754.
7 Jernerén F, Cederholm T, Refsum H, Smith AD, Turner C, Palmblad J, Eriksdotter M, Hjorth E, Faxen-Irving G, Wahlund LO, Schultzberg M, Basun H, Freund-Levi Y. Homocysteine Status Modifies the Treatment Effect of Omega-3 Fatty Acids on Cognition in a Randomized Clinical Trial in Mild to Moderate Alzheimer’s Disease: The OmegAD Study. J Alzheimers Dis. 2019;69(1):189-197. doi: 10.3233/JAD-181148. PMID: 30958356.
Alzheimer’s is a preventable, but not reversible disease.
Less than one in a hundred cases are directly caused by genes. Prevention is entirely possible if you can identify who is at risk early enough and encourage the right diet and lifestyle changes.
This is why we have designed our new pinprick blood test which not only aims to predict your future risk for dementia but tells you how to reduce it. We now have a limited number available on pre-order as part of a global prevention research study aiming to involve a million people worldwide.
This much-awaited home-test kit measures your blood sugar, vitamin D, omega-3 and B vitamin status which account for more than half the modifiable risk for dementia. The results show how a person can reduce their risk with specific diet changes.
“By tracking a person’s blood sugar, vitamin B, D and omega-3 status against changes in cognitive function over time, in addition to lifestyle factors such as sleep and physical activity, we can learn what really helps prevent cognitive decline.” says Dr Wood, Assistant Professor at the University of Washington and the principal investigator for the prevention project.
We have already tested over 410,000 people with our free Cognitive Function Test, and hope to enrol a million people, to make this the largest Citizen Science global prevention initiative.
Subtle changes in cognition occur at least 30 years before a diagnosis, which is why we screen people online with a free Cognitive Function Test. And four simple blood tests are not only predictive but can help a person to understand how to drive down that risk. We call them the four horsemen of the mental health apocalypse because they also drive depression and ADHD. The incidence of both of these are on the increase.
(Read more about the four horsemen of the mental health apocalypse here and here).
The four tests, called DRIfT (the Dementia Risk Index functional Test) is carried out using a simple home-test kit and a single pinprick of blood, adding further predictive capability, and helping guide the individual to make diet changes to reduce future risk.
—
Why these four markers?
Blood sugar (HbA1c) – Even raised blood sugar levels from age 35, but within ‘reference’ ranges, predict a 15 per cent increased risk of Alzheimer’s disease 35 years later, according to research by Boston University School of Medicine (1). This confirms other research from the University of Washington showing an 18% increased risk with raised sugar levels in older people seven years later and a 40% increased risk in those with diabetes (2). Even better than your blood sugar level, which varies across the day, is a long-term measure of blood sugar, called HbA1c, used to predict diabetes, which is what this test measures.
B vitamins (Homocysteine) – Low levels of B12, found in animal products, and folate, found in greens, raise blood levels of homocysteine. Raised homocysteine is considered a top marker for dementia risk, and is a causative driver of the disease process (3). Studies lowering homocysteine with B vitamins have more than halved the rate of age-related brain shrinkage. A Swedish study, started in 1968, found that those in the top third of homocysteine scores in their 40’s had double the risk for Alzheimer’s almost 35 years later (4). When homocysteine goes up memory gets worse and when it goes down memory gets better, according to a six-year study in Norway (5).
About half of all people over 60 have homocysteine levels above 11mcmol/l (6), which is the level associated with increased brain shrinkage. A study in Italy found that those with a homocysteine above 15mcmol/l have five times the risk of developing Alzheimer’s, compared to those with a level below 10 (7).
Last year, a study in China showed that raised homocysteine increases risk of cognitive decline by ten times (8). Homocysteine is easily lowered by supplementing vitamin B6, B12 and folate but at levels higher than achievable from diet because many older people do not absorb B12 well.
Oxford University’s health economist Dr Apostolos Tsiachristas estimates “Screening for homocysteine in people over 60 in the UK and treating those with raised levels with B vitamins could save the UK economy approximately £60 million per year.”
Omega-3 – Increased intake of omega-3, either from diet or supplements and having a higher omega-3 blood level, is associated with cutting risk for dementia by a fifth (20%), according to a study of 48 studies involving over 100,000 people (9).
Supplementing fish oils (10) cuts risk of dementia by 9%, according to research from the UK Bio Bank. Being in the top third for omega-3 blood levels, compared to the lowest third, reduced the rate of brain shrinkage in a year by more than two-thirds in those given B vitamins with mild cognitive impairment (11).
The omega-3 index, which is what the DRIfT test measures, predicts both brain size and cognitive function (12). This Oxford University research establishes that the brain needs both sufficient B vitamins and omega-3 to stay healthy.
Vitamin D – Having a higher vitamin D above 75nmol/l (25 ng/ml) cuts risk for Alzheimer’s and dementia by a third (13). In turn, those with a vitamin D level below 50nmol/l, increase their risk for Alzheimer’s and dementia by a third (14).
Six out of 10 adults in the UK (15) and three out of 10 in the US (16) have a vitamin D level below this. Taking vitamin D supplements may help ward off dementia, according to a 2023 study involving over twelve thousand dementia-free 70+ year olds in the US. Those taking vitamin D supplements had 40% lower incidence of dementia during a ten-year period. Vitamin D is essential to supplement during winter months.
These four risk factors, measured in the DRIfT test, are thought to account for over half the modifiable risk for Alzheimer’s disease and dementia. Having an active lifestyle, both physically, socially and intellectually further reduces risk substantially.
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
References
1 Zhang X, Tong T, Chang A, Ang TFA, Tao Q, Auerbach S, Devine S, Qiu WQ, Mez J, Massaro J, Lunetta KL, Au R, Farrer LA. Midlife lipid and glucose levels are associated with Alzheimer’s disease. Alzheimers Dement. 2023 Jan;19(1):181-193. doi: 10.1002/alz.12641. Epub 2022 Mar 23. PMID: 35319157; PMCID: PMC10078665.
2 P.K. Crane et al., ‘Glucose levels and risk of dementia’, New England Journal of Medicine (2013), vol 369(6):540–548.
3 Smith AD, Refsum H, Bottiglieri T, Fenech M, Hooshmand B, McCaddon A, Miller JW, Rosenberg IH, Obeid R. Homocysteine and Dementia: An International Consensus Statement. J Alzheimers Dis. 2018;62(2):561-570. doi: 10.3233/JAD-171042. PMID: 29480200; PMCID: PMC5836397.
4 Zylberstein DE, Lissner L, Bjorkelund C, Mehlig K, Thelle DS, Gustafson D, Ostling S, Waern M, Guo X, Skoog I (2011) Midlife homocysteine and late-life dementia in women. A prospective population study. Neurobiol Aging 32, 380-386
5 Nurk E, Refsum H, Tell GS, Engedal K, Vollset SE, Ueland PM, Nygaard HA, Smith AD (2005) Plasma total homocysteine and memory in the elderly: The Hordaland Homocysteine study. Ann Neurol 58, 847-857.
6 Pfeiffer CM, Osterloh JD, Kennedy-Stephenson J, Picciano MF, Yetley EA, Rader JI, Johnson CL. Trends in circulating concentrations of total homocysteine among US adolescents and adults: findings from the 1991-1994 and 1999-2004 National Health and Nutrition Examination Surveys. Clin Chem. 2008 May;54(5):801-13. doi: 10.1373/clinchem.2007.100214. Epub 2008 Mar 28. PMID: 18375482.
7 Ravaglia G, Forti P, Maioli F, Martelli M, Servadei L, Brunetti N, Porcellini E, Licastro F (2005) Homocysteine and folate as risk factors for dementia and Alzheimer disease. Am J Clin Nutr 82, 636-643.
8 Teng Z, Feng J, Liu R, Ji Y, Xu J, Jiang X, Chen H, Dong Y, Meng N, Xiao Y, Xie X and Lv P (2022) Cerebral small vessel disease mediates the association between homocysteine and cognitive function. Front. Aging Neurosci. 14:868777. doi: 10.3389/fnagi.2022.868777
9 Wei BZ, Li L, Dong CW, Tan CC; Alzheimer’s Disease Neuroimaging Initiative; Xu W. The Relationship of Omega-3 Fatty Acids with Dementia and Cognitive Decline: Evidence from Perspective Cohort Studies of Supplementation, Dietary Intake, and Blood Markers. Am J Clin Nutr. 2023 Apr 5:S0002-9165(23)46320-4. doi: 10.1016/j.ajcnut.2023.04.001. Epub ahead of print. PMID: 37028557.
10 Huang Y, Deng Y, Zhang P, Lin J, Guo D, Yang L, Liu D, Xu B, Huang C and Zhang H (2022) Associations of fish oil supplementation with incident dementia: Evidence from the UK Biobank cohort study.Front. Neurosci. 16:910977.doi: 10.3389/fnins.2022.910977
11 Jernerén F, Elshorbagy AK, Oulhaj A, Smith SM, Refsum H, Smith AD. Brain atrophy in cognitively impaired elderly: the importance of long-chain ω-3 fatty acids and B vitamin status in a randomized controlled trial. Am J Clin Nutr. 2015 Jul;102(1):215-21. doi: 10.3945/ajcn.114.103283. Epub 2015 Apr 15. PMID: 25877495.
14 Chai et al. BMC Neurology (2019) 19:284 https://doi.org/10.1186/s12883-019-1500-6
15 Calame W, Street L, Hulshof T. Vitamin D Serum Levels in the UK Population, including a Mathematical Approach to Evaluate the Impact of Vitamin D Fortified Ready-to-Eat Breakfast Cereals: Application of the NDNS Database. Nutrients. 2020 Jun 23;12(6):1868. doi: 10.3390/nu12061868. PMID: 32585847; PMCID: PMC7353432.
16 Liu X, Baylin A, Levy PD. Vitamin D deficiency and insufficiency among US adults: prevalence, predictors and clinical implications. Br J Nutr. 2018 Apr;119(8):928-936. doi: 10.1017/S0007114518000491. PMID: 29644951.
This is why we launched our highly accurate and groundbreaking at-home homocysteine test just before Christmas (and quickly sold out) because knowing this marker – your H factor – can help predict over 100 diseases. Specifically, homocysteine is an indicator of a person’s B vitamin status, and knowing this, can help reduce the risk of mental illness.
Yet it hasn’t been easily available or affordable to test this at home and is often not a marker checked by Dr’s.
But not any more!
Homocysteine & the Central Nervous System
“Homocysteine is a biomarker for over 100 diseases, but especially those of the central nervous system.” says pharmacology professor David Smith FMedSci, formerly Deputy Head of the Faculty of Medical Sciences at the University of Oxford. “It is a biomarker of impaired cognitive abilities in children, and in adults is a risk marker for stroke, dementia and Alzheimer’s, but also possibly for depression, anxiety, bipolar, schizophrenia, obsessive-compulsive disorder, Parkinson’s and multiple sclerosis. It is very much the forgotten factor, despite the research evidence being strongly positive (1). And the good news is, it is so easily corrected.”
Patrick Holford, psychologist and our CEO and founder says “A raised homocysteine level means something is going wrong with a vital process that controls how we think, feel and perceive. It’s called methylation and is dependent on B vitamins. Some people absorb B12 less well. Some just need more of the B vitamin than others and that biochemical individuality, especially if their diet is already deficient, can tip them into a mental or neurological illness.”
Depression & Homocysteine
Those suffering from depression are also more likely to have higher homocysteine levels (2, 3). Amanda-Jane is a case in point. She was suffering with chronic fatigue and low mood, so she decided to check her homocysteine level. She was shocked when she found her score was 26 mcmol/l (7 or less is considered optimal). After changing her diet and supplementing the B vitamins her sleep improved almost immediately and within four weeks, she had much more energy. Two months later she re-tested her homocysteine level and found it had dropped to 9. “I feel much better. My mood is very positive– no panic or depression. I feel buoyant, energetic and enthusiastic. I’m sleeping much better and my PMS has disappeared.” she said.
Also, every 5-point increase in homocysteine increases risk of being diagnosed with schizophrenia by a staggering 70%! (4) Yet very few sufferers are ever checked for raised homocysteine.
Homocysteine & B Vitamins
Professor Joseph Levine from the Stanley Research Centre and Beersheva Mental Health Centre in the Ben Gurion University in Israel devised a study to see what effect lowering homocysteine with B vitamins would have (5). He gave half of a group of 42 schizophrenic patients B vitamins (B6, B12 and folic acid) and the other half a placebo. Those taking the B vitamin supplements had both a dramatic reduction in their homocysteine levels and a significant improvement in their symptoms, except for one patient, who didn’t comply with the B vitamin treatment, didn’t improve and didn’t have a reduction in their homocysteine level. They were the exception that proves the rule.
Professor David Smith, writing in the Journal of Internal Medicine, together with world leading expert on homocysteine, Professor Helga Refsum from the University of Oslo, Norway, say “There are five diseases that can, at least in part, be prevented by lowering total homocysteine: neural tube defects, impaired childhood cognition, macular degeneration, primary stroke, and cognitive impairment in the elderly. We conclude from our review that total homocysteine values in adults of 10 mcmol/L or below are probably safe, but that values of 11 above may justify intervention. Homocysteine is more than a disease biomarker: it is a guide for the prevention of disease.” Not only does it predict an increased risk for a stroke, but having a lower homocysteine level, achieved by eating B12 rich foods such as fish and eggs, and folate and B6 rich foods such as whole foods, vegetables, nuts, seeds and beans, and supplementing B vitamins, helps those who’ve had a stroke recover faster (6).
We recommend anyone with a homocysteine level over 10 mcmol/L to supplement extra B vitamins, especially B6 (20mg), folate (400mcg) and B12 (500mcg). Homocysteine is a toxic amino acid that accumulates when there is a lack of B vitamins and damages your brain as well as your arteries.
Professor Smith’s research group at Oxford University has shown that giving people with pre-dementia these vitamins reduced the rate of brain shrinkage to less than half of that in those given placebos.
“Further cognitive decline virtually stopped in those taking the B vitamins.” says Smith.
Homocysteine, Pregnancy & Children’s School Grades
As many as two in five people over 60 have a raised homocysteine level. The reason why the B vitamin folic acid is recommended in pregnancy is because it lowers homocysteine. In ‘normal’ pregnancies with no complications in either mother or child, homocysteine remains below 7mcmol/L. In five out of seven studies women who have spontaneous abortions or miscarriages have a level above 15. The risk for having a pre-term baby is four times higher in women with a homocysteine level above 12 (7). A study of 81 healthy women who then became pregnant found that the children of the women whose homocysteine before conceiving was above 9 were significantly more withdrawn, anxious and depressed and had more social problems including increased aggressive behaviour (8).
“It is vital that a woman intending to become pregnant first checks her homocysteine level. Raised homocysteine, plus a lack of omega-3 fats found in fish is a major promoter of developmental problems and mental illness in children later in life.” says Holford.
A child’s homocysteine level even predicts their school grades. A study compared the sum of school grades for ten core subjects, with homocysteine levels in a group of 692 Swedish school children aged 9 to 15. Increasing homocysteine levels were strongly associated with reducing grades as was inadequate folate intake (9).
Join us in our Citizen Science Project by testing your homocysteine! The home pin prick blood test is now back in stock.
Thank you for reading!
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices.
Please support our research by becoming a Friend of Food for the Brain.
References
1 Smith AD, Refsum H. Homocysteine – from disease biomarker to disease prevention. J Intern Med. 2021 Oct;290(4):826-854. doi: 10.1111/joim.13279. Epub 2021 Apr 6. PMID: 33660358.
2 Moradi F, Lotfi K, Armin M, Clark CCT, Askari G, Rouhani MH. The association between serum homocysteine and depression: a systematic review and meta- analysis of observational studies. Eur J Clin Invest 2021: e13486.
3 Nabi H, Bochud M, Glaus J, Lasserre AM, Waeber G, Vollenweider P, Preisig M. Association of serum homocysteine with major depressive disorder: results from a large population-based study. Psychoneuroendocrinology 2013; 38: 2309-18.
5 Levine J, Stahl Z, Sela BA, Ruderman V, Shumaico O, Babushkin I, Osher Y, Bersudsky Y, Belmaker RH. Homocysteine-reducing strategies improve symptoms in chronic schizophrenic patients with hyperhomocysteinemia. Biol Psychiatry. 2006 Aug 1;60(3):265-9. doi: 10.1016/j.biopsych.2005.10.009. Epub 2006 Jan 17. PMID: 16412989.
6 Yahn GB, Leoncio J, Jadavji NM. The role of dietary supplements that modulate one-carbon metabolism on stroke outcome. Curr Opin Clin Nutr Metab Care. 2021 Jul 1;24(4):303-307. doi: 10.1097/MCO.0000000000000743. PMID: 33631772; see also
7 Dai C, Fei Y, Li J, Shi Y, Yang X. A Novel Review of Homocysteine and Pregnancy Complications. Biomed Res Int. 2021 May 6;2021:6652231. doi: 10.1155/2021/6652231. PMID: 34036101; PMCID: PMC8121575.
8 Roigé-Castellví J, Murphy M, Fernández-Ballart J, Canals J. Moderately elevated preconception fasting plasma total homocysteine is a risk factor for psychological problems in childhood. Public Health Nutr. 2019 Jun;22(9):1615-1623. doi: 10.1017/S1368980018003610. Epub 2019 Jan 14. PMID: 30636652; PMCID: PMC10261079.
9 Torbjörn K. Nilsson, Agneta Yngve, Anna K. Böttiger, Anita Hurtig-Wennlöf, Michael Sjöström; High Folate Intake Is Related to Better Academic Achievement in Swedish Adolescents. Pediatrics August 2011; 128 (2): e358–e365. 10.1542/peds.2010-1481