Everyone knows that Alzheimer’s and cognitive decline are preventable IF you can find out who is at risk.
While those selling anti-amyloid or p’tau drugs will exaggerate the importance of blood testing for amyloid or p’tau, which are damaged proteins found in the brains of people with Alzheimer’s, so far lowering these markers hasn’t worked. In other words, they are a marker, but not a cause.
—
So, what is a biomarker that predicts risk?
And therefore what biomarkers, if corrected, reduce risk?
To date, there are four:
Homocysteine, a toxic amino acid, which goes up when your intake of B vitamins (B6, B12, folate, as well as zinc) is low. If you then lower homocysteine with B vitamins, it stops the brain shrinkage associated with Alzheimer’s and improves cognitive function. Brain shrinkage stops below 10 mcmol/l, and that’s what you’re aiming for. So that’s both ‘biomarker’ and ‘causal’ ticked.
At Food for the Brain, we are offering the first accurate at home, pinprick test for homocysteine that is both painless and accurate.
Omega-3 index is another. This is the % of your red blood cell membranes that are omega-3 EPA and DHA. The higher your % (ideally above 8) the better your cognition. Low levels also predict risk. So that’s also two boxes ticked.
Vitamin D is another. Low levels predict risk and supplementing it reduces risk. Again, two boxes ticked but we don’t really know how it does this.
Combining these three to make a ‘nutritional index’ shows that the better you score, the lower a person’s future risk of dementia is.
HBA1c is another. This is a measure of your blood sugar resilience. It measures the spikes in your blood sugar that then damage red blood cells. Below 5.4% (or 37 mmol/mol) is the idea.
We divide your scores across four levels – worst is RED, then ORANGE, then YELLOW, then GREEN, which is what you’re shooting for.
That’s what our DRIfT test measures – all four as a Dementia Risk Index functional Test.
This chart shows you why these four measures are so essential.
What about antioxidants?
But you might have noticed there’s no ‘antioxidant’ measure.
Well, actually there is. It’s the body’s most important antioxidant called glutathione. Think of it like the body’s fire department with glutathione being the water. Every time there’s an oxidant fire, glutathione rushes in to put the fire out. The water, then, turns into steam. Glutathione is called GSH. It’s not bad as a measure of ‘antioxidant potential’. That’s why most functional medicine doctors measure red blood cell glutathione. But what if it all gets used up? It becomes oxidised or spent, much like the water putting out a fire turns into steam. This is called oxidised glutathione or GSSG. Think of the fully loaded glutathione (GSH) as cold water. It’s going to protect you much better from inflammation than spent (oxidised) glutathione (GSSH), a highl level of which means you’ve been trying to put out a lot of inflammatory fires in your brain and body. Neuro-inflammation is a key driver of brain degeneration and dementia, as well as ageing in general, which is why this is important to know.
We’ve been researching the ratio that is your GSH/GSSG. If you’ve got lots of fully loaded glutathione, and very little oxidised/spent glutathione, your GSH/GSSG ratio or index is high. That’s good news. If you’ve got very little fully loaded glutathione and lots of oxidised glutathione then you’re ‘oxidising’ – which is an aspect of ageing that we want to prevent.
We want to be able to research this and test your Glutathione Index. This is exactly what we are working on right now with the hope of releasing another ‘world first’ home test kit for your Glutathione Index soon. This kind of research is funded by you, as a Friend of Food for the Brain.
An example would be a person who smokes a lot, lives in a polluted environment, eats no fresh veg, berries, herbs and spices. Their Glutathione Index will be low and their body and brain will likely be ageing faster. If you did smoke but also ate well and took vitamin C daily, (they say you need 50mg of vitamin C for each cigarette) would that mitigate the effect?
Would you join our research, support our charitable work and upgrade your own brain by ordering one of our DRIftT tests?
If you’ve also done the Cognitive Function Test and Dementia Risk Index questionnaire (which we strongly recommend) that’s even better because we can see how you score in the ANTIOXIDANT domain and in future, how that will correlate with your Glutathione Index (which is coming soon).
—
Thank you for reading!
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
Last month’s newspaper headlines pitched the new anti-amyloid Alzheimer’s drug as a ‘turning point’. The pitch has a lot in common with the statin story.
Last month’s newspaper headlines pitched the new anti-amyloid Alzheimer’s drug as a ‘turning point’. (Read our response here) The pitch has a lot in common with the statin story.
Is high cholesterol the cause of heart disease? No.
Do statins lower it? Yes.
Are amyloid deposits the cause of cognitive decline? No.
Do anti-amyloid drugs lower it? Yes.
No doubt there will be a blood test soon for amyloid, just like a blood test for cholesterol, the effect of which pushed millions into taking statins.
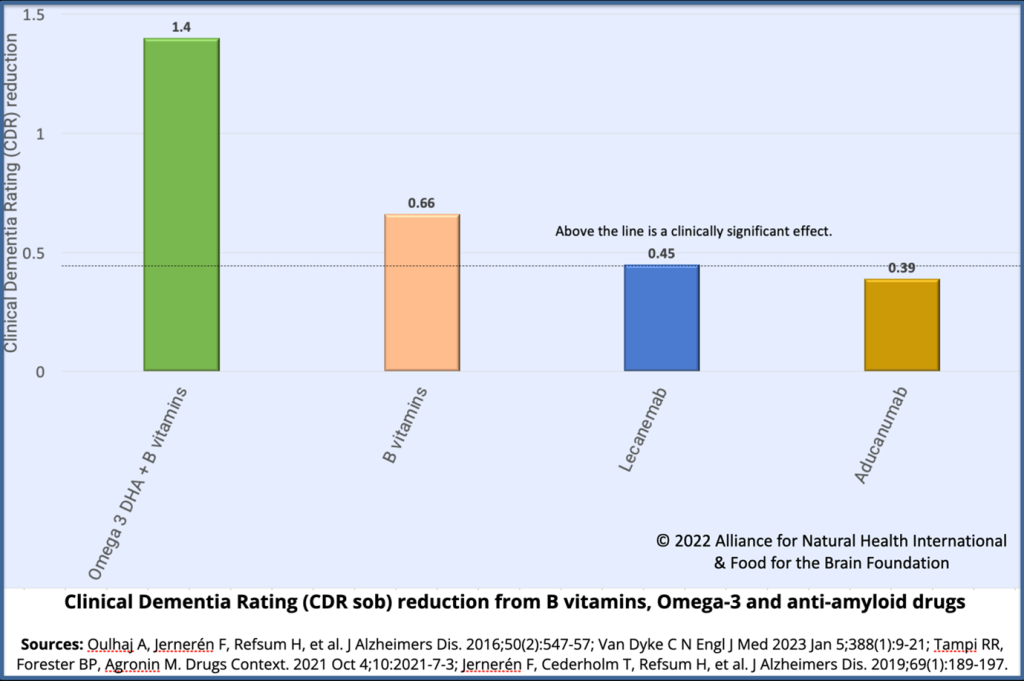
Both statins, given to people with very high cholesterol, and anti-amyloid drugs, given to people with very high amyloid levels, do have marginal benefit but not enough to establish causation. In the case of the new Alzheimer’s drug, the benefit is considerably less than half that shown by the combination of B vitamins and omega-3.
But, even more than statins, they come with a high risk of quite serious adverse effects – over a third in the recent trial got brain bleeding or swelling and three died. Also, the whole brain shrinkage accelerated by twenty percent compared to placebo, a fact not reported in any newspaper. Any vitamin showing such adverse effects would be immediately banned.
But the important question is: what’s causing these diseases, be it cognitive decline or heart disease? To the extent that cholesterol or amyloid is relevant, what makes them go up? Cholesterol gets damaged by sugar and oxidants and is protected by antioxidants such as vitamin C and a low-carb diet. Brain cells get damaged by homocysteine and are protected by B vitamins and omega-3.
Mind the gap
Also, in those with cognitive decline, there’s an energy deficit in brain cells. Ironically, they can’t get the glucose they need due to ‘insulin resistance’ which is driven by eating too much sugar and ultra-processed carbs. So, the effect of too much sugar is to starve the brain of fuel which then leads to mental tiredness and cognitive decline.
There is a way around this – and that is to give the brain an alternative fuel – ketones.
Ketones can either be supplied as ketone salts or esters, both of which taste disgusting or made from a type of fat – principally C8 oil, which is a medium-chain triglyceride. About 7 percent of coconut oil is C8. Studies giving people with cognitive decline a C8-rich MCT oil have shown clear improvements in cognition by increasing the brain’s energy supply and production. Ripping out amyloid deposits isn’t going to fill this energy gap. Eating less carbs, reversing diabetes, which is a big risk factor for dementia, and having C8 oil will. Our podcast with Professor Stephen Cunnane, who heads the Brain Research Team at Sherbrooke University in Sherbrooke, Quebec, Canada and holds the clinical research chair in ketotherapeutics and on the Food for the Brain Scientific Advisory Board, discusses this area with Patrick Holford – listen to the podcast here.
Also, in those with cognitive decline, there’s an energy deficit in brain cells. Ironically, they can’t get the glucose they need due to ‘insulin resistance’ which is driven by eating too much sugar and ultra-processed carbs. So, the effect of too much sugar is to starve the brain of fuel which then leads to mental tiredness and cognitive decline.
An increase in amyloid in the brain is really a consequence of the disease, not the cause. It’s part of an inflammatory reaction, much like the nodules in joints that occur from inflammation resulting in arthritis. Should you cut out the nodules or reduce inflammation? Do you eliminate the root cause or target the consequences? Inflammation is both a function of a bad diet high in ultra-processed and fried food, smoking, lack of antioxidants, omega-3 fats and vitamin C to name a few key nutrients. Having an active lifestyle is also important.
The same story exists with all major diseases. Cancer cells thrive on sugar. Do you starve them and in the process protect healthy cells, or cut or drug them out?
The big difference in approach – treat the cause or the consequences – is money. You can’t patent nutrients, but you can patent drugs that stop you from making cholesterol or amyloid. More than $1 billion has been spent on the anti-amyloid approach and the push isn’t going to stop. Pharma needs a return on their investment. This latest drug treatment, according to the Financial Times, will be sold for $26,000 a year. Taking B vitamins, eating fish and/or supplementing omega-3, which has shown more clinical benefit and reduced the rate of brain shrinkage by over 70% with no side-effects – actually side-benefits – might cost £100 a year. Which would you choose?
Food for the Brain is a non-for-profit educational and research charity that offers a freeCognitive Function Testand assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing theCognitive Function Testyou are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices.
Friday’s Guardian article on ‘I refuse to get old’ about how readers strive to keep dementia at bay, on the face of it, seems like a good message. Most cases given focussing on people increasing physical and mental activity, as an active lifestyle is certainly a positive step towards prevention. But these two prevention steps reduce risk by less than B vitamins, omega-3 and reducing sugar and carbs.
The first error is the extent to which dementia can be prevented. The article says by 40%, which is based on the inaccurate Lancet Commission’s Livingston report which, despite being sent all the evidence, doesn’t even mention B vitamins and homocysteine, which is the single most important prevention step. There’s also only one mention of omega-3 from a redundant study so this risk factor is also ignored to arrive at the ‘40% preventable’ figure.
80% of dementia cases could be prevented, not 40%
The latest assessment of how much can be prevented, based on UK Biobank data is “47%–73% of dementia cases could be prevented.” This was published last week in Nature and even this is an underestimate because, while including B vitamins, it excludes the impact of omega-3 and seafood. If that modifiable risk factor were included it is likely that around 80% of dementia cases could be prevented. This would mean that the Guardian is halving the impact of prevention.
The next error is no-one quoted in the article mentions diet, let alone B vitamins or omega-3, except for Professor David Smith. He rightly says: ‘The large leap forward in what we know about preventability has informed his own retirement lifestyle: he walks for half an hour a day, spends at least 15 minutes on an exercise bike, drinks alcohol sparingly, and follows a Mediterranean diet.
Having led a clinical trial into the benefits of B vitamins in people with mild cognitive impairment – a memory-loss condition that increases the chance of those who have it developing dementia – Smith takes 500mcg of vitamin B12 daily and fish oil with Omega 3. Nutrition, he believes, is not given enough prominence when we talk about prevention.’
When we calculated the attributable risk for each risk factor for our online Dementia Risk Index questionnaire each domain scores as follows, adding up to 100%:
B Vitamins 18%
Brain Fats 17%
Glycemic Load 15%
Active Body 15%
Active Mind 10%
Sleep & Calm 10%
Antioxidants 10%
Gut Health 5%
So, the biggest impact you can have on your risk is to supplement B vitamins, especially B12, and omega-3 fish oils, as David Smith does. But the Guardian article then downplays the role of supplements with this statement ‘Alzheimer’s Research UK does not recommend any supplements in particular, but says “there is no harm in people taking a supplement to reduce the risk of deficiency”.
B12 Reference Ranges are wrong
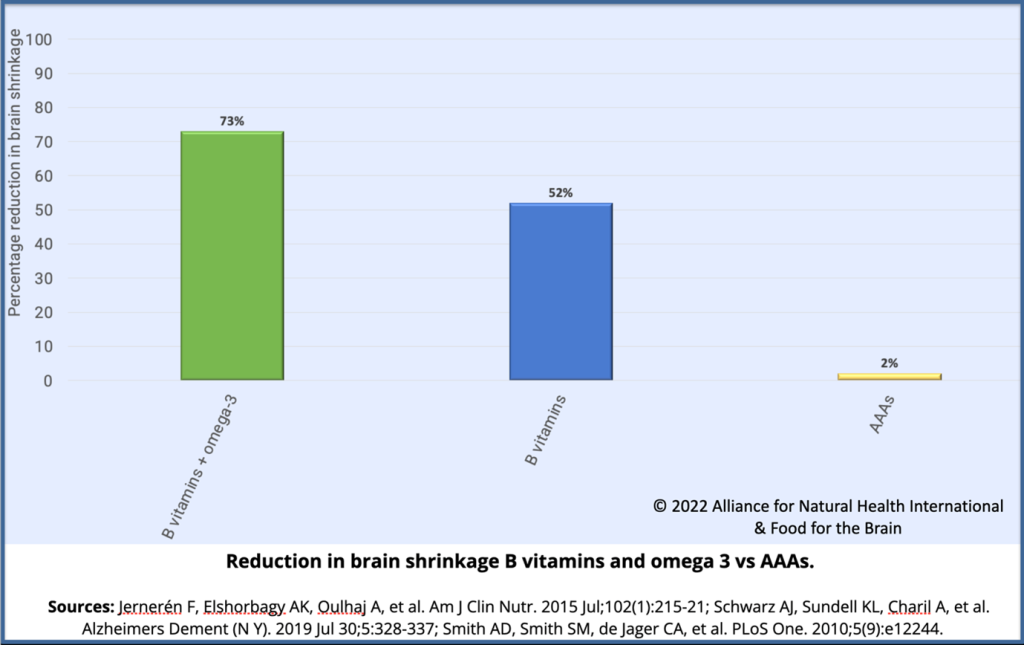
This is not only wrong because brain shrinkage occurs well within the ‘normal’ range of either B12 dietary intake or blood tests, but also ARUK, who largely promotes drug-based solutions, happened to know what they are saying is wrong because they funded, back in 2010, a top level, randomised placebo controlled trial on B vitamins that, virtually stopped cognitive decline and reduced brain shrinkage by 52% – in the group with higher omega 3 , by 73% – that is the most effective disease modifying treatment to date! In fact, David Smith and I have written to ARUK to stop making this inaccurate statement. Here’s why it’s wrong:
The reason so many people are low in B12 is less to do with dietary intake and more due to malabsorption which often becomes worse with age, due to lack of stomach acid secretions which are needed to absorb B12. So relying only of analysing what someone eats (meat, fish, eggs, dairy being the only sources of B12) doesn’t prove sufficiency. Note that David Smith says he supplements 500mcg of B12 daily, while the basic ‘Nutrient Reference Value’ (NRV) that you’ll see on the back of a vitamin supplement is 2.5mcg. So, why does he take two hundred times this amount? Because you cannot rely on your dietary intake to confirm sufficiency. Also, there is growing body of evidence from well designed studies showing that supplements giving nutrients at levels beyond the basic ‘recommended intakes’ delay, eliminate or ameliorate symptoms of dementia.
So, what about blood tests? One UK study reports that 2 in five people over 61 have insufficient levels of B12 to prevent accelerated brain shrinkage. Serum B12 is the ‘standard’ test used by doctors. The UK reference range of above 180pg/ml being sufficient (and the US lower level of 200pg/ml) is out of date and in need of revision. In Europe and Japan anything below 500pg/ml is considered deficient. Accelerated brain shrinkage due to a lack of B12 does happen with B12 levels below 500pg/ml.
In conclusion, while it is good to recommend a physically and intellectually lifestyle, ignoring the need to supplement B vitamins, especially B12, eat fish and supplement omega-3, and cut your intake of carbs and sugar, is not doing anyone any favours.
Food for the Brain is a non-for-profit educational and research charity that offers a freeCognitive Function Testand assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing theCognitive Function Testyou are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices.
Autism is one disease where there is a very high ‘inherited’ component.
In studies with genetically identical twins, if one twin has it, the odds of another having a diagnosis is about 60%. But it’s not in the ‘in the genes’ since we share the same ‘environment’ as our siblings.
Perhaps the more interesting question is why the number of children diagnosed with Attention-deficit /hyperactivity disorder (ADHD), autism and other neurodevelopmental disorders classifying them as ‘neurodivergent’, has rocketed in both the UK and US.
One in six children is ‘neurodivergent’ as autism numbers quadruple.
UK figures (see here) which show that just under 1.5 million pupils in England have special educational needs which is one in six children. Autism is the biggest part of this, has been steadily rising in both the Uk and US.
“Now, one in six children in the US are classified as neurodivergent and one in 36 as autistic – a fourfold increase in 20 years.” says pediatric Professor Alessio Fasano from Massachusetts General Hospital for Children, Harvard Medical School.
—
All down to our increased awareness & better diagnosis?
According toDr Rona Tutt OBE, past president of the UK’s National Association of Head Teachers “There has been a dramatic increase in the number of people being diagnosed with ASD. Although some of this is due to a broader definition of autism as well as better diagnosis, it raises the question of whether it may also be the result of environmental changes, which have also been dramatic.”
Some UK schools are reporting as many as one in four children having problems.
Have our genes changed in the past few decades?
Since the genes cannot have changed this rapidly, the increase points to the influence of environmental factors of which there are many candidates.
The main suspects are:
Gut problems
Wheat, milk and sugar
Vaccines
Environmental anti-nutrients and toxins
Social media overuse and social issues
Maternal nutrition and brain formation essential fats
—
The gut’s role
World-renowned pediatric gastroenterologist, and research scientist Professor Alessio Fasano, MD, directs the Center for Celiac Research and Treatment at Massachusetts General for Children thinks something is going wrong in the gut, with many ASD children reporting gut problems including diarrhoea, constipation, belching and excessive flatulence and ‘dysbiosis’ – abnormal patterns of gut bacteria. In some children, wheat and milk may contribute to these symptoms. His research finds that neurodivergent children show high levels of ‘zonulin’, a family of proteins that regulate the barrier between intestinal cells in the digestive tract that can lead to “leaky gut.” ASD children are often found to have opioid-like wheat and milk proteins in their urine, making these foods especially ‘addictive’.
—
Prenatal nutrition?
Professor Michael Crawford, who heads the Institute of Brain Chemistry and Human Nutrition at the Chelsea & Westminster Hospital says “We can predict which babies are going to have developmental problems from the fats in the mother’s blood. When omega-3 levels are low, the mother produces a non-functional ‘brain fat substitute’ to build their baby’s brain during pregnancy, high levels of which predict problems. The brain is 50% fat, and omega-3 DHA should make up most of the structural fat in brain cells.” Less than 5 per cent of children in the UK achieve the basic dietary recommendations for omega-3 and fish.
—
Methylation & B vitamins
Vitamins may help. ‘A high level of homocysteine, a marker for B vitamin deficiency, predicts ASD and studies have shown that giving homocysteine-lowering vitamin B6, B12 and folate help reduce symptoms.” says Patrick Holford from the Food for the Brain Foundation, which is hosting the masterclass. “Vitamin A improves eye coordination and vision, helping those with autism who don’t look you in the eye and have visual problems.”
A 12-month randomised controlled trial giving omega-3, vitamins, digestive enzymes and a healthy gluten-free, casein-free diet showed major improvement in both autistic symptoms and raising IQ.
Nutrition and functional medicine therapist Anne Pemberton, who specialises in helping those with ASD, is spoke at theAutism Masterclass reports considerable success, not just by improving nutrition but by addressing the psychological and social circumstances of neurodivergent children. “It is critical to work with both mother and child, and not only address critical nutritional issues, stress triggers including early life traumas, and suppressed emotions as a result of their condition and conditioning, and to help them develop a sense of self and mindset. I have seen hundreds of children and adults who usually have major improvements. Peter, age 8, is a case in point. He was diagnosed with ASD and classified as needing special education. 15 months later he’s no longer even classified as ASD.”
So, as you can see, there are many layers to Autism and Neurodivergence.
In the UK progress in putting these breakthroughs into action is slow. The two leading charities, the Alzheimer’s Society and Alzheimer’s Research UK (ARUK) fail to mention the importance of homocysteine lowering B vitamins and omega-3 at all and have confirmed that they are not funding any research on their use in prevention or planning to do so. ARUK’s chief medical officer Professor Jon Schott and the Alzheimer’s Society’s associate director of research, Richard Oakley, declined to comment.
ARUK’s Brain Health Check-In, a short 13 question check list, with only one very basic question on diet, says nothing at all about B vitamins or whether or not a person supplements omega-3 fish oils despite ARUK having part-funded the Oxford University research. According to Professor Smith, who was the first Chair of their Scientific Advisory Board “ARUK part-funded our trial on B vitamins, and are aware of the results. I don’t understand why they make no mention of such an effective preventive intervention, that is taking a 10p a day B vitamin supplement if your homocysteine is high. Now we know that those who also supplement with omega-3 fish oil, or eat fish regularly, reduce their risk. These are the easiest two prevention actions anyone can take, with a significant impact on reducing the risk for dementia. Everyone needs to know this.”
“We’ve been applying to UK and EU agencies for the past 8 years to fund the obvious next trial – testing the effects of B vitamins and omega-3 combined to see if they slow, or prevent, conversion from cognitive impairment to dementia, but to no avail.” Says Professor Smith.
Neither the Alzheimer’s Society, nor ARUK are funding any vitamin or omega-3 research and spend virtually none of their annual research pot, which exceeded £37 million last year, on diet or lifestyle prevention which offer the most potential, despite these representing up to half of the risk for Alzheimer’s. Neither would confirm the percentage of their research funds that were being spent on prevention research.
UK Government have pledged to deliver ‘Dementia Moonshot’, doubling dementia research funding to £160 million to ‘fast-track the development of new treatments’, meanwhile ignoring the biggest breakthroughs in diet and lifestyle prevention. Most support is feeding failed drug research. With an estimated $50 billion [12] spent so far on amyloid drugs and research, all of which have failed to produce any clinical benefit, isn’t it time governments and Alzheimer’s charities took prevention seriously?
In contrast, the Food for the Brain Foundation are doing just that. “At Foodforthebrain.org we are testing almost 4,000 people every month on our free online Cognitive Function Test, and assessing all risk factors on a 140 question questionnaire, including the need for B vitamins and omega-3. We hope, soon, to introduce a pinprick blood test for both omega-3 and homocysteine. We don’t know why the most evidence-based, easy to action and inexpensive prevention steps are being ignored” says Holford. “Why world class scientists such as Professor David Smith’s team at Oxford University have been unable to get funding for the most essential research is shameful. Right now we know enough to cut the average person’s risk of developing Alzheimer’s by up to two thirds and the number of people developing dementia by a third if only there was the political will to do so.”
One of the reasons for complacency in the UK is the Lancet’s commissioned report on Alzheimer’s prevention chaired by Gillian Livingston, Professor of Psychiatry for Older People, at the University College London (UCL). The report, first published in 2017, didn’t include B vitamins. Despite being sent all the evidence by Smith. The 2020 revised report still excluded this vital research, as did a follow up report specifically on supplements in 2022. “There are no trials that show that lowering homocysteine has any benefit” she told us yet she had been sent the unequivocal evidence that the B vitamins reduced brain shrinkage by up to 73%, compared to the 2% reduction of anti-amyloid drugs and the combination of omega-3 and B vitamins has lowered the Clinical Dementia Rating (CDR) in placebo controlled trials by three times that reported by the recent anti-amyloid drug, Lecanemab. (see charts below).
When asked about the recent finding of a synergistic effect of B vitamins and omega-3 she said “It sounds a good hypothesis. I hope they can get the funding for it, but raised homocysteine is not common in the wider population and drug companies can’t be expected to fund nutrition trials, so money would have to come from some government agency.”
There is one prevention study, called AppleTree, underway at University College London. It focuses on reducing risk for Alzheimer’s by eating a Mediterranean style diet and lifestyle advice, including encouraging smokers to quit, which is a known risk factor for cognitive decline. One recent study shows that being a smoker increases risk for dementia by 1.5 times and quitting for at least 3 years reduces much of that risk. [13] One in twelve people over 65 smoke.
In contrast, almost half of all people over 65 have raised homocysteine [14] which increases risk for cognitive impairment by up to ten times, according to Chinese research published last year[15]. Lowering homocysteine with B vitamins, and sufficient omega-3, would virtually eliminate that risk. This suggests that targeting B vitamins and omega-3 would be about twenty times more impactful in preventing dementia than quitting smoking. Yet the need for supplemental intake of these nutrients is not part of the Apple Tree protocol.
If you’d like to test your cognitive function and find out how to reduce your risk, register here and join our citizen science campaign.
[3] van Soest, A.P.M., van de Rest, O., Witkamp, R.F. et al. DHA status influences effects of B-vitamin supplementation on cognitive ageing: a post-hoc analysis of the B-proof trial. Eur J Nutr (2022). https://doi.org/10.1007/s00394-022-02924-w
[4] Jernerén F, Cederholm T, Refsum H, Smith AD, Turner C, Palmblad J, Eriksdotter M, Hjorth E, Faxen-Irving G, Wahlund LO, Schultzberg M, Basun H, Freund-Levi Y. Homocysteine Status Modifies the Treatment Effect of Omega-3 Fatty Acids on Cognition in a Randomized Clinical Trial in Mild to Moderate Alzheimer’s Disease: The OmegAD Study. J Alzheimers Dis. 2019;69(1):189-197. doi: 10.3233/JAD-181148. PMID: 30958356.
[5] Walsh S, Merrick R, Richard E, Nurock S, Brayne C. Lecanemab for Alzheimer’s disease. BMJ. 2022 Dec 19;379:o3010. doi: 10.1136/bmj.o3010. PMID: 36535691.
[6] Li M, Li W, Gao Y, Chen Y, Bai D, Weng J, Du Y, Ma F, Wang X, Liu H, Huang G. Effect of folic acid combined with docosahexaenoic acid intervention on mild cognitive impairment in elderly: a randomized double-blind, placebo-controlled trial. Eur J Nutr. 2021 Jun;60(4):1795-1808. doi: 10.1007/s00394-020-02373-3. Epub 2020 Aug 28. PMID: 32856190.
[7] Yu JT, Xu W, Tan CC, Andrieu S, Suckling J, Evangelou E, Pan A, Zhang C, Jia J, Feng L, Kua EH, Wang YJ, Wang HF, Tan MS, Li JQ, Hou XH, Wan Y, Tan L, Mok V, Tan L, Dong Q, Touchon J, Gauthier S, Aisen PS, Vellas B. Evidence-based prevention of Alzheimer’s disease: systematic review and meta-analysis of 243 observational prospective studies and 153 randomised controlled trials. J Neurol Neurosurg Psychiatry. 2020 Nov;91(11):1201-1209. doi: 10.1136/jnnp-2019-321913. Epub 2020 Jul 20. PMID: 32690803; PMCID: PMC7569385.
[8] Huang Y, Deng Y, Zhang P, Lin J, Guo D, Yang L, Liu D, Xu B, Huang C, Zhang H. Associations of fish oil supplementation with incident dementia: Evidence from the UK Biobank cohort study. Front Neurosci. 2022 Sep 7;16:910977. doi: 10.3389/fnins.2022.910977. PMID: 36161159; PMCID: PMC9489907.
[9] Jeong SM, Park J, Han K, Yoo J, Yoo JE, Lee CM, Jung W, Lee J, Kim SY, Shin DW. Association of Changes in Smoking Intensity With Risk of Dementia in Korea. JAMA Netw Open. 2023 Jan 3;6(1):e2251506. doi: 10.1001/jamanetworkopen.2022.51506. PMID: 36656579; PMCID: PMC9857334.
[10] Beydoun MA, Beydoun HA, Gamaldo AA, Teel A, Zonderman AB, Wang Y. Epidemiologic studies of modifiable factors associated with cognition and dementia: systematic review and meta-analysis. BMC Public Health. 2014 Jun 24;14:643. doi: 10.1186/1471-2458-14-643. PMID: 24962204; PMCID: PMC4099157.
[11] Witte AV, Kerti L, Hermannstädter HM, Fiebach JB, Schreiber SJ, Schuchardt JP, Hahn A, Flöel A. Long-chain omega-3 fatty acids improve brain function and structure in older adults. Cereb Cortex. 2014 Nov;24(11):3059-68. doi: 10.1093/cercor/bht163. Epub 2013 Jun 24. PMID: 23796946.
[12] Cummings JL, Goldman DP, Simmons-Stern NR, Ponton E. The costs of developing treatments for Alzheimer’s disease: A retrospective exploration. Alzheimers Dement. 2022 Mar;18(3):469-477. doi: 10.1002/alz.12450. Epub 2021 Sep 28. PMID: 34581499; PMCID: PMC8940715.
[13] Lu Y, Sugawara Y, Zhang S, Tomata Y, Tsuji I. Smoking cessation and incident dementia in elderly Japanese: the Ohsaki Cohort 2006 Study. Eur J Epidemiol. 2020 Sep;35(9):851-860. doi: 10.1007/s10654-020-00612-9. Epub 2020 Feb 15. PMID: 32060675; PMCID: PMC7525275.
[14] Pfeiffer CM, Osterloh JD, Kennedy-Stephenson J, Picciano MF, Yetley EA, Rader JI, Johnson CL. Trends in circulating concentrations of total homocysteine among US adolescents and adults: findings from the 1991-1994 and 1999-2004 National Health and Nutrition Examination Surveys. Clin Chem. 2008 May;54(5):801-13. doi: 10.1373/clinchem.2007.100214. Epub 2008 Mar 28. PMID: 18375482.
[15] Teng Z, Feng J, Liu R, Ji Y, Xu J, Jiang X, Chen H, Dong Y, Meng N, Xiao Y, Xie X and Lv P (2022) Cerebral small vessel disease mediates the association between homocysteine and cognitive function. Front. Aging Neurosci. 14:868777. doi: 10.3389/fnagi.2022.868777
In the days of Hippocrates, diseases were blamed on the gods. He didn’t buy that and explored the causes of disease saying ‘let food be thy medicine’. Nowadays a lot of diseases are being blamed on genes – because knowledge about genes and their effects has advanced tremendously over the last several decades. Genes are the code, or instructions, to assemble proteins, for example to make an enzyme, a hormone or a biochemical such as cholesterol or phospholipids.
Take Alzheimer’s, which accounts for two thirds of dementia, as an example. There are only three genes that can cause Alzheimer’s (APP, PSEN1, PSEN2), and these account for considerably less than one in a hundred cases of Alzheimer’s. [1]
There are, however, 76 other genes [2] which appear to confer a very small additional risk. Taken together, estimates suggest that 75-85% of the risk can be explained by combining these into a polygenic risk score. [3] The single greatest predictor is the presence of the ApoE4 variant of the ApoE gene, carried by about one in five people. It is considered to contribute 4 to 6% of the absolute risk for Alzheimer’s disease. [4,5]
This is often exaggerated as a risk factor because, if a person has the ApoE4 gene, and changes nothing, they have about a 20% greater chance of developing Alzheimer’s later in life than someone who doesn’t. This is called ‘relative risk’. It doesn’t mean, however, that someone with the ApoE4 gene has a 20% chance of developing Alzheimer’s. This is because, as an example, a person without the ApoE4 gene at a certain age might have a 5% chance of developing Alzheimer’s, while someone with the ApoE4 gene might have a 6% chance, so their risk has gone up by, in this example, 20%. In absolute terms, the risk would be only 1% higher.
Predicting risk and actually reducing risk with modifications of diet and lifestyle are two different things. The predictive risk for Alzheimer’s of having a low intake of seafood and/or omega-3 fats is 22%, and so is having a low intake of B vitamins resulting in a high blood homocysteine level. Smoking confers a similar risk. [6] Other big risk factors are an inactive lifestyle and low level of education. Add in predictive genes and apparent risk adds to well over 100% partly because there is overlap.
But the only way to find out how much you can actually reduce a person’s risk by is to either conduct ‘observational’ studies looking at, e.g. smokers vs non-smokers, or people with a good versus a bad diet, and see how many develop dementia. Even better is to change something, such as looking at what happens when a person stops smoking, or supplements omega-3 fish oils or homocysteine lowering B vitamins.
Modifying ApoE4 with orthomolecular medicine
All these so-called Alzheimer’s genes, with the exception of the causative ones, can only exert effects via non-genetic mechanisms and these mechanisms are often susceptible to modification with a person’s nutrition having the most direct influence. In other words, gene variants that are present are not either active or inactive. Even if you have a gene variant such as ApoE4 it is more like a dimmer switch and can be ‘over-expressed’ or ‘down-regulated’, turned up or dimmed down. That is why approximately half of women with the BRCA gene develop breast cancer and half don’t. The environment the gene is exposed to makes all the difference.
The expression and harmful effects of the ApoE4 gene appear to be downregulated by eating a low-glycemic load (GL) diet or a more ketogenic diet with specific Mediterranean-style food choices including fatty fish, cruciferous vegetables, olive oil, and low alcohol consumption. Six supplemental nutrients have reasonably good evidence of down-regulating ApoE4. These are omega-3 DHA, B vitamins (B2, B6, B12 and folate) vitamins D3 and K2, quercitin and resveratrol. [7] This approach to modifying the effects of the genes we inherit with personalised nutrition is a fundamental tenet of orthomolecular medicine, sometimes called personalised, precision or optimum nutrition.
But what happens to risk if a person is doing these things already? A good example of this is a recent study in China, involving 29,072 people of which 20% had the ApoE4 gene. [8] Each participant had their diet and lifestyle assessed over the 10 year period of the study to see who would or wouldn’t develop cognitive decline or dementia.
The study showed that whether or not a person had the ApoE4 ‘Alzheimer’s gene’ made no difference to the positive reduction in risk achievable by simple diet and lifestyle changes. “These results provide an optimistic outlook, as they suggest that although genetic risk is not modifiable, a combination of more healthy lifestyle factors is associated with a slower rate of memory decline, regardless of the genetic risk,” wrote the study authors.
Eating a healthy diet was the most important prevention step, followed by an active lifestyle, with one’s intellectual life, then physical activity, then social interactions being the next most important steps. Eating a healthy diet was about twice as important as exercise in predicting cognitive decline. Those with a healthy diet were about seven times less likely to have age-related cognitive decline or dementia than those with an ‘average’ diet and about nine times less likely to develop dementia than those with an unfavorable diet.
The assessment of a healthy diet was based on intake of fish, eggs, fruits, vegetables, legumes, nuts and tea, among other foods known to predict lower risk.
B vitamins modify methylation of genes linked to dementia
Other Alzheimer’s related genes affect a process called methylation. Healthy methylation depends on adequate B vitamin intake, primarily B6, B12 and folate. Inheriting a variant of a key methylation gene, MTHFR 677TT increases risk for Alzheimer’s. [9-11] About one in three people have this gene variant. It impacts risk by raising homocysteine, a toxic amino acid that damages the brain and blood vessels. Having a raised homocysteine level increases risk for cerebrovascular dysfunction 17-fold. [12]
Since methylation is needed to make phospholipids, biochemicals essential for the brain also found in eggs and fish, having a poor diet in this respect creates more methylation demand and, consequently, greater need for B vitamins.
In a placebo controlled study of older people with mild cognitive impairment, about a third of participants had the MTHFR variant that increases Alzheimer’s risk. But supplementing with B vitamins effectively lowered homocysteine in both those with and without this ‘Alzheimer’s’ gene. The B vitamin supplement almost arrested further memory decline and slowed the rate of brain shrinkage by 52%, [13,14] reducing shrinkage of the Alzheimer’s areas of the brain by 9-fold. [15] Whether a person did or didn’t have this ‘Alzheimer’s’ gene made no difference to the beneficial effect of the B vitamins.
Those with adequate omega-3 blood levels had even less brain shrinkage – 73% less than the placebo group. [16-17] Two other studies have found major protection either by giving B vitamins to those with adequate omega-3 intake, [18] or by supplementing omega-3 to those with lower homocysteine levels [19] further confirming that you need both B vitamins and omega-3 fats to keep neurons healthy – an example of synergy – regardless of one’s genes. Whether a person did or didn’t have the MTHFR variant made no significant difference.
Too often genes are blamed as drivers of disease even though (with the exception of rare causative genes) the primary drivers are what you put in your mouth or how you live your life – both factors under our control. For example, DNA genetic testing can cause panic when an individual is informed they have a dozen or more gene variants. Over-emphazing the importance of genes discourages people from preventing their own disease by improving diet and lifestyle.
Find out your dementia risk
Cognitive Function Test Results
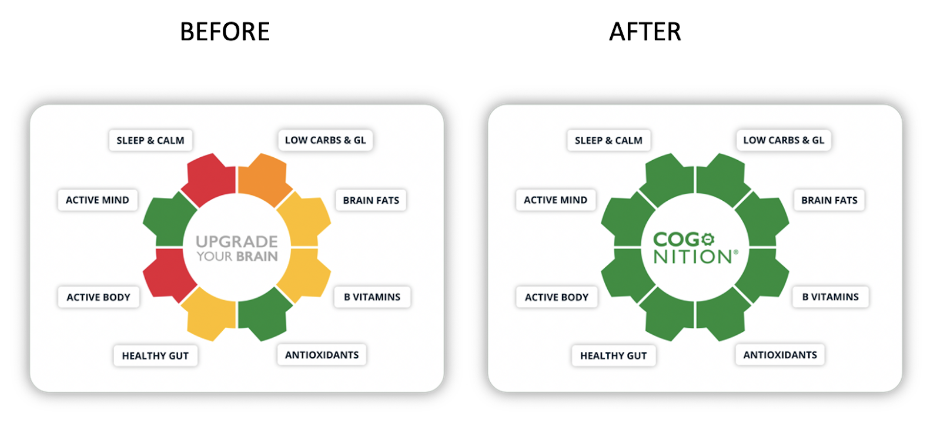
You can find out what’s driving your risk and which diet and lifestyle changes will make the biggest difference by doing the Cognitive Function Test at foodforthebrain.org and joining COGNITION, the brain upgrade program. Not only do you help yourself, you also help the hundreds of thousands of people who would benefit from the research we support at Food for the Brain to reduce risk of dementia.
About Patrick Holford
(Patrick Holford , BSc, DipION, FBANT, NTCRP is widely published and a member of the Orthomolecular Medicine Hall of Fame. He is the director of the non-profit, UK-based “Alzheimer’s is Preventable” campaign [ foodforthebrain.org].)
2. Bellenguez C, Küçük F, Jansen IE, et al. (2022) New insights into the genetic etiology of Alzheimer-s disease and related dementias. Nat Genet. 54:412-436. https://pubmed.ncbi.nlm.nih.gov/35379992
3. Escott-Price V, Myers AJ, Huentelman M, Hardy J. (2017) Polygenic risk score analysis of pathologically confirmed Alzheimer disease. Ann Neurol. 82:311-314. https://pubmed.ncbi.nlm.nih.gov/28727176
4. Heininger K (2000), A unifying hypothesis of Alzheimer’s disease. III. Risk factors. Hum Psychopharmacol Clin Exp. 15:1-70. https://pubmed.ncbi.nlm.nih.gov/12404343
6. Beydoun MA, Beydoun HA, Gamaldo AA, et al. (2014) Epidemiologic studies of modifiable factors associated with cognition and dementia: systematic review and meta-analysis. BMC Public Health. 14:643. https://pubmed.ncbi.nlm.nih.gov/24962204
7. Norwitz NG, Saif N, Ariza I.E, Isaacson RS (2021) Precision Nutrition for Alzheimer’s Prevention in ApoE4 Carriers. Nutrients 13:1362. https://pubmed.ncbi.nlm.nih.gov/33921683
8. Jia J, Zhao T, Liu Z et al. (2023) Association between healthy lifestyle and memory decline in older adults: 10 year, population based, prospective cohort study. BMJ 380:e072691. https://pubmed.ncbi.nlm.nih.gov/36696990
9. Morris AA, Kožich V, Santra S, et al. (2017) Guidelines for the diagnosis and management of cystathionine beta-synthase deficiency. J Inherit Metab Dis. 40:49-74. https://pubmed.ncbi.nlm.nih.gov/27778219
10. Bouguerra K, Tazir M, Melouli H, Khelil M. (2022) The methylenetetrahydrofolate reductase C677T and A1298C genetic polymorphisms and plasma homocysteine in Alzheimer’s disease in an Algerian population. Int J Neurosci. 29:1-6. https://pubmed.ncbi.nlm.nih.gov/36580407
11. Zuin M, Cervellati C, Trentini A, et al. (2021) Methylenetetrahydrofolate reductase C667T polymorphism and susceptibility to late-onset Alzheimer’s disease in the Italian population. Minerva Med. 112:365-371. https://pubmed.ncbi.nlm.nih.gov/32700867
12. Teng Z, Feng J, Liu R, et al. (2022) Cerebral small vessel disease mediates the association between homocysteine and cognitive function. Front. Aging Neurosci. 14:868777. https://pubmed.ncbi.nlm.nih.gov/35912072
13. Smith AD, Smith SM, de Jager CA, et al. (2010) Homocysteine-lowering by B vitamins slows the rate of accelerated brain atrophy in mild cognitive impairment: a randomized controlled trial. PLoS One. 5(9):e12244. https://pubmed.ncbi.nlm.nih.gov/20838622
15. Douaud G, Refsum H, de Jager CA, et al. (2013) Preventing Alzheimer’s disease-related gray matter atrophy by B-vitamin treatment. Proc Natl Acad Sci USA 110:9523-9528. https://pubmed.ncbi.nlm.nih.gov/23690582
16. Jernerén F, Elshorbagy AK, Oulhaj A, et al. (2015) Brain atrophy in cognitively impaired elderly: the importance of long-chain omega-3 fatty acids and B vitamin status in a randomized controlled trial. Am J Clin Nutr. 102:215-221. https://pubmed.ncbi.nlm.nih.gov/25877495
17. Oulhaj A, Jernerén F, Refsum H, et al. (2016) Omega-3 fatty acid status enhances the prevention of cognitive decline by B vitamins in Mild Cognitive Impairment. J Alzheimer’s Dis. 50:547-557. https://pubmed.ncbi.nlm.nih.gov/26757190
18. van Soest, A.P.M., van de Rest, O., Witkamp, R.F. et al. (2022) DHA status influences effects of B-vitamin supplementation on cognitive ageing: a post-hoc analysis of the B-proof trial. Eur J Nutr. 61:3731-3739. https://pubmed.ncbi.nlm.nih.gov/35704085
19. Jernerén F, Cederholm T, Refsum H, et al. (2019) Homocysteine Status Modifies the Treatment Effect of Omega-3 Fatty Acids on Cognition in a Randomized Clinical Trial in Mild to Moderate Alzheimer’s Disease: The OmegAD Study. J Alzheimers Dis. 69:189-197. https://pubmed.ncbi.nlm.nih.gov/30958356
The BBC’s recent story headed ‘Dementia: Brain check-up tool aims to cut risk at any age’ is a step in the right direction since early prevention is the key to reducing risk. However, the online brain health check, hosted by the Alzheimer’s Research Trust, is very basic, with only a dozen questions, and ignores the key evidence-based and common nutritional risk factors for Alzheimer’s disease. It covers ‘stay sharp’ which is about mental stimulation, ‘stay connected’ which is about social interaction and ‘love your heart’.
What the test ignores
It ignores the two strongest nutritional risk factors, namely homocysteine lowering B vitamins and omega-3 intake from seafood. The US National Institute for Health’s research [1] attributes 22% of Alzheimer’s risk to each of these.
‘Love your heart’ gives advice to keep your cholesterol and blood pressure in check and manage diabetes. This refers an individual to their GP who is likely to prescribe statins to lower cholesterol and hypertensive drugs to lower blood pressure. Neither reduce Alzheimer’s risk. A recent major review [2] of the evidence concludes ‘prospective, randomized, placebo‐controlled clinical trials that have failed to provide evidence for the benefit of statin therapy’ and there is ‘insufficient [evidence] to tell us whether reducing BP for dementia risk reduction is effective.’
The same review recommends omega-3 supplementation is start early and maintained and B vitamin supplementation to lower homocysteine, which is cited as the most evidence-based prevention approach considered. This report says “In view of the high population attributable risk, it is important that raised homocysteine can readily be lowered by the oral administration of three B vitamins (folate, B6, and B12). The doses of these vitamins that are required to lower homocysteine are considerably larger than can readily be obtained from the diet.” This is based on evidence of the VITACOG trial [3] which was part funded by the Alzheimer’s Research Trust.
A GP could lower a person’s risk much more effectively by measuring homocysteine in the blood and recommending B vitamin supplements, as well as upping omega-3 intake by eating fish and/or supplementing. This combination has reduced the rate of brain shrinkage by up to 73% in those with pre-dementia [4] but only few GPs do.
The Think Brain Health check does not assess diet, or make specific recommendations, and there’s no mention of protective supplements, but refers people to the NHS’s ‘eight tips for healthy eating’. These recommend ensuring starchy carbohydrates make up over a third of what you eat, reducing saturated fat and salt. There is no evidence that these reduce risk for Alzheimer’s. Too many carbs may actually be a promoter of cognitive decline. They also recommend eating less sugar, lots of fruit and veg and having at least 2 portions of fish a week, including at least 1 portion of oily fish. There is evidence that these recommendations may reduce dementia risk.
Food For the Brain’s Cognitive Function Test
In sharp contrast foodforthebrain.org’s validated Cognitive Function Test and Dementia Risk Index questionnaire (139 questions) both objectively measure a person’s cognitive function and calculates their risk, then gives specific and actionable instructions as to how a person can reduce their risk, inviting them back every six months to track their progress.
The Cognitive Function Test is free and for those who wish to improve, we have launched COGNITION, a new way to Upgrade your Brain at a low cost of just £5 per month. You can access both tests once logged into your account.
References
1. Beydoun MA, Beydoun HA, Gamaldo AA, Teel A, Zonderman AB, Wang Y. Epidemiologic studies of modifiable factors associated with cognition and dementia: systematic review and meta-analysis. BMC Public Health. 2014 Jun 24;14:643. doi: 10.1186/1471-2458-14-643. PMID: 24962204; PMCID: PMC4099157.
2. Peters R, Breitner J, James S, Jicha GA, Meyer PF, Richards M, Smith AD, Yassine HN, Abner E, Hainsworth AH, Kehoe PG, Beckett N, Weber C, Anderson C, Anstey KJ, Dodge HH. Dementia risk reduction: why haven’t the pharmacological risk reduction trials worked? An in-depth exploration of seven established risk factors. Alzheimers Dement (N Y). 2021 Dec 8;7(1):e12202. doi: 10.1002/trc2.12202. PMID: 34934803; PMCID: PMC8655351.
3. Smith AD, Smith SM, de Jager CA, Whitbread P, Johnston C, Agacinski G, Oulhaj A, Bradley KM, Jacoby R, Refsum H. Homocysteine-lowering by B vitamins slows the rate of accelerated brain atrophy in mild cognitive impairment: a randomized controlled trial. PLoS One. 2010 Sep 8;5(9):e12244. doi: 10.1371/journal.pone.0012244. PMID: 20838622; PMCID: PMC2935890.
4. Oulhaj A, Jernerén F, Refsum H, Smith AD, de Jager CA. Omega-3 Fatty Acid Status Enhances the Prevention of Cognitive Decline by B Vitamins in Mild Cognitive Impairment. J Alzheimers Dis. 2016;50(2):547-57. doi: 10.3233/JAD-150777. PMID: 26757190; PMCID: PMC4927899.
A recent study of 1,178 women found that those carrying the APOE4 gene taking Hormone Replacement Therapy (HRT) had a better delayed memory score compared to APOE4 carriers that were not taking HRT, and to non-APOE4 carriers.[1] They also had slightly larger brain volumes in certain areas. This study suggested that HRT may help to prevent Dementia. This study was an observational trial, not a clinical trial, meaning the statement remains a hypotheses and requires further randomised controlled trials to investigate further. We analysed the paper and provided our comments below.
Hormone Replacement Therapy (HRT) are synthetic hormones commonly prescribed to menopausal women to reduce menopausal symptoms
Clinical Trials on HRT
Clinical trials to date have not shown benefit of HRT with improving cognitive function. A systematic review of the clinical trial evidence for the effect of HRT on cognitive outcomes did not find benefit.[2] The Women’s Health Initiative Memory Study (WHIMS) conducted a double-blind, placebo-controlled clinical trial examining 8300 women 65 years of age or older over a 2- year period to observe the effects of HRTs and dementia progression. The trial failed to find a beneficial effect for HRT in reducing dementia risk, instead finding an increase in all types of dementia.[3]
The ApoE4 Gene
Roughly 1 in 5 people carry the ApoE4 gene, which accounts for 4 to 6% of risk for dementia and can be modified, downregulating the gene, with positive diet, nutritional supplement and lifestyle changes.[1]
Find out your risk for Dementia
In our Dementia Risk Index, as part of the Cognitive Function test, and COGNITION programme to reduce dementia, we excluded HRT because the evidence was not conclusive or consistent.
Have you tried our free Cognitive Function Test yet? Find out your Alzheimer’s disease risk using our evidence backed Dementia Risk Index. If your risk is high, our clever new programme COGNITION can help you make the right nutrition and lifestyle changes to help improve your score.
The 8 Domains of the Dementia Risk Index from The Cognitive Function Test
References
[1] Saleh RNM, Hornberger M, Ritchie CW, Minihane AM. Hormone replacement therapy is associated with improved cognition and larger brain volumes in at-risk APOE4 women: results from the European Prevention of Alzheimer’s Disease (EPAD) cohort. Alzheimers Res Ther. 2023 Jan 9;15(1):10. doi: 10.1186/s13195-022-01121-5. PMID: 36624497; PMCID: PMC9830747.
[2] Marjoribanks J, Farquhar C, Roberts H, Lethaby A, Lee J. Long-term hormone therapy for perimenopausal and postmenopausal women. Cochrane Database Syst Rev. 2017;1(1):CD004143.
[3] Shumaker SA, Legault C, Rapp SR, et al. Estrogen plus progestin and the incidence of dementia and mild cognitive impairment in post- menopausal women: the Women’s Health Initiative Memory Study: a randomized controlled trial. JAMA. 2003;289(20):2651-2662.