In recent years the number of children diagnosed with learning, behavioural and mental health problems has escalated. Attention-deficit hyperactivity disorder (ADHD), autistic spectrum disorder (ASD) and other neurodevelopmental disorders, all classifying children as ‘neurodivergent’, as opposed to ‘neurotypical’, have rocketed in both the UK and USA.
Over the past decade there has also been a steady increase in young people with now four in ten reporting persistent feelings of sadness or hopelessness and almost a quarter (22%) reporting contemplating suicide. (1)
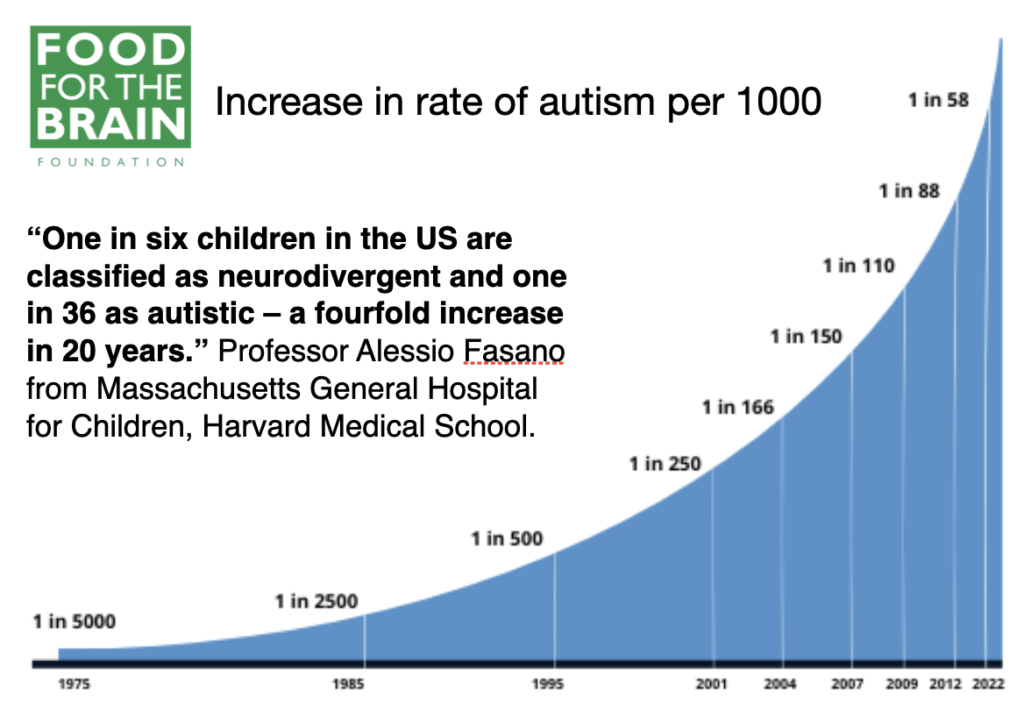
‘Now, one in six children in the USA are classified as neurodivergent and one in 36 as autistic – a fourfold increase in 20 years,’(2) says paediatric Professor Alessio Fasano from Massachusetts General Hospital for Children, Harvard Medical School.
Rising numbers are being reported in the UK. According to Dr Rona Tutt, OBE, past president of the National Association of Headteachers, ‘There has been a dramatic increase in the number of people being diagnosed with ASD. Although some of this is due to a broader definition of autism, as well as better diagnosis, it raises the question of whether it may also be the result of environmental changes, which have also been dramatic.’ Some UK schools are reporting as many as one in four children having problems.
For clarification, the University of Washington defines a ‘neurodivergent’ person as ‘a person on the autism spectrum or, more generally, someone whose brain processes information in a way that is not typical of most individuals. These people may have learning disabilities, attention deficit and anxiety disorders, obsessive-compulsive disorder, and Tourette’s syndrome. Through a neurodiversity lens, such conditions reflect different ways of being that are all normal human experiences. Although “neurodiversity” is usually used to describe a group of neurodivergent individuals, it also refers to all of humankind, because everyone has a unique way of processing information.’
For those with neurodivergent traits that cause individuals immense difficulty, the question is, why do they occur in some and not others, and can they be prevented?
Making healthy babies
Autistic spectrum disorder has often been positioned as being genetically linked. However, since the genes cannot have changed this rapidly, this suggests the influence of environmental factors, of which diet and maternal nutrition are big contributors.
Brain development starts from conception
Brain development is influenced from the moment of conception. That is why a mother’s nutrition before conception is so critical.
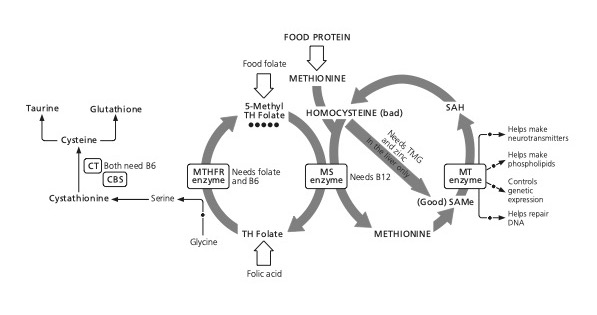
Nothing can be built without healthy methylation, which means a low homocysteine level. Raised homocysteine is a well-known predictor of miscarriage and pregnancy problems, which is why I recommend no woman attempts pregnancy until her homocysteine level is below 7mcmol/l. While we have learned that a homocysteine level above 11 means increased brain shrinkage, even a homocysteine level of above 9 during pregnancy predicts more problems, specifically withdrawn behaviour, anxiety, depression, social problems and aggressive behaviour in the child at the age of six. (3)
That’s why building a healthy child’s brain starts with ensuring mothers-to-be are optimally healthy.
We already know that pioneering researcher Professor Michael Crawford can predict which babies are going to be born preterm with a greater risk of having developmental problems from the fats in the pregnant woman’s blood. But the most convincing evidence comes from a study of 11,875 pregnant women which showed a clear relationship between the amount of seafood consumed by a pregnant woman and their child’s development. The less seafood consumed, the worse the child’s social behaviour, fine motor skills, communication and social development, and verbal IQ. (4)
Also, a lack of vitamin A during pregnancy can affect brain development and lead to long-term or even permanent impairment in the learning process, memory formation, and cognitive function. (5)
Supplementing mothers-to-be with folic acid (400 µg/day) during the second and third trimesters of pregnancy is associated with better cognition in their children at the age of three and better word reasoning and IQ (verbal and performance) at seven. (6)
Nourishing infants with optimum nutrition
Once a baby is born, 75 percent of all the energy derived from breastmilk goes to build the brain, as brain development continues at the mind-boggling rate of something like 1 million connections a minute. Babies use ketones to power their early brain development, but they also need the raw materials – essential fats, phospholipids and vitamins. Without sufficient omega-3, vitamin A, D and B vitamins, especially folate and B12, as well as minerals such as iodine, magnesium, iron and zinc, the brain cannot develop optimally.
This means that a breastfeeding mother must, at least, supplement omega-3 fish oils, but many other nutrients are also necessary. Without sufficient nutrients, not only do brain cells not make the connections, but the production and flow of neurotransmitters doesn’t happen optimally.
Low vitamin D status in both the mother and newborn baby increases the likelihood of the child developing ASD by 54 per cent. (7)
Bruce Ames, Emeritus Professor of Biochemistry and Molecular Biology at the University of California, thinks that ‘serotonin synthesis, release, and function in the brain are modulated by vitamin D and the two marine omega-3 fatty acids, eicosapentaenoic acid, EPA, and docosahexaenoic acid, DHA’. He says, ‘Insufficient levels of vitamin D, EPA, or DHA, in combination with genetic factors and at key periods during development, would lead to dysfunctional serotonin activation and function and may be one underlying mechanism that contributes to neuropsychiatric disorders and depression in children.’(8)
We know that a mother’s folate intake predicts the child’s performance in cognitive tests at the age of nine to ten (9) and the higher a baby’s B-vitamin status, the higher their cognitive function at the age of 25. (10)
Nourishing the growing child
In the UK, fewer than 5 percent of children achieve the basic dietary recommendations for omega-3 and fish. (11) Lower DHA concentrations are associated with poorer reading ability, poorer memory, oppositional behaviour and emotional instability. (12) Several studies have shown increased aggression in those with low omega-3 DHA and EPA, and giving more omega-3 reduces aggression. (13)
Fish and omega-3 are associated with better cognition in children.
A study of 541 Chinese schoolchildren found that fish consumption predicted sleep quality and that those who ate the most fish had the highest IQ, 4.8 points higher than those who ate none. Improved sleep quality, linked to fish intake, was correlated with IQ. (14)
A study in Northern Ireland found that half of schoolchildren were deficient in vitamin D, with a level below 50 nmol/l (I recommend above 75 nmol/l). Another found that low vitamin D levels in childhood were related to behaviour problems in adolescence. (15)
Is it any wonder so many children are neurodivergent?
Another nutrient that is rich in marine food is vitamin A. Cod liver oil is a rich source of vitamin A, vitamin D and omega-3 fats. Vitamin A is vital for proper black and white vision and the proper functioning of the retina in the eye, hence its name, retinol, and the idea of eating carrots to see in the dark. Dr Mary Megson, a paediatrician in the USA, identified a particular genetic weakness in several children on the spectrum which would affect their ability to use vitamin A. She associates this with children who won’t look you in the eye because they see better on the periphery of their visual field. (16) Giving a source of retinol such as cod liver oil improves eye coordination and vision, helping those with autism who don’t make eye contact.
Think zinc and magnesium
My teacher, Dr Carl Pfeiffer, was the first to put zinc on the map for mental health, in the 1970s, thanks to a girl called Lisa.
Lisa was mentally unwell, but her parents had learned how to keep her sane: oysters. If she had a couple of oysters a day, her mind calmed down.
Dr Pfeiffer worked out it was zinc. Zinc is essential for cellular growth and repair, and thus found in all seeds, nuts, beans and lentils, as well as eggs, meat and fish, but nothing beats oysters. Zinc is one of the most essential minerals in pregnancy, along with iron, and babies and children, due to their rapid growth, need more.
Bear in mind that vegetarian sources of zinc, such as nuts and seeds, also contain phytates, which inhibit zinc’s absorption, so those on an exclusively plant-based diet might need more.
The basic calculation for our zinc needs to support growth is 7.5mg a day. (An oyster gives 5.5mg.) But is that really the minimum? What’s the optimum? The Nutrient Reference Value is 10mg. Many children fail to achieve this.
Few have explored what zinc intake is needed for optimal mental health. Researchers in North Dakota gave 200 schoolchildren in the 7th grade zinc supplements and found that those taking 20mg of zinc a day, as opposed to those taking 10mg (the RDA) or a placebo, had faster and more accurate memories and better attention spans within three months.(17) The girls, also, behaved better.
Children with ADHD tend to have lower levels of zinc, chromium and magnesium.
Some have low levels of copper, according to research in New Zealand. (18)
One study of ADHD children found higher levels of copper. (19) Copper, the main source of which is copper water pipes, and zinc compete, so if zinc is low the body’s copper levels tend to rise. It was the copper-to-zinc ratio that was especially high in neurodivergent versus neurotypical children and predicted the degree of ADHD.(20)
The same applies to schizophrenia, with some of those diagnosed having low zinc levels (21) and higher copper levels (22) Copper is likely to be higher in softer water areas and in newer houses with copper pipes. Blue staining in baths or sinks is an indication of a high copper level in the water. Both zinc and magnesium levels tend to be lower in those with depression.
Magnesium, a commonly deficient mineral, is calming. Zinc deficiency is linked to disperceptions both in eating disorders and schizophrenia, as well as depression and anxiety. Both zinc and magnesium are critical co-factor nutrients, activating enzymes that make the all-important brain fats such as DHA and EPA, as well as neurotransmitters, from the food we eat.
Checking a child’s zinc, chromium and magnesium status, which can be done with a hair or blood sample, is a standard practice in nutritional therapy, but not routine in mainstream medicine. Red cell magnesium levels and serum zinc are perhaps more reliable, but hair is less invasive in children. A small study found lower hair levels of chromium in those with ADHD.(23)
Nuts and seeds are high in all three nutrients, and correcting deficiencies with diet and/or supplementation is a must for neurodivergent children. Greens and other vegetables are rich in magnesium. A placebo-controlled trial giving ADHD children magnesium together with vitamin D for eight weeks showed a major reduction in emotional, conduct and peer problems and improved socialisation compared with children given a placebo.(24)
A Polish study from 1997 which examined the magnesium status of 116 children with ADHD found that magnesium deficiency occurred far more frequently in them than in healthy children (95 per cent of the children with ADHD were deficient), and also noted a correlation between the levels of magnesium in the body and severity of symptoms. The children were divided into two groups, one supplemented with 200mg of magnesium a day for six months and the other receiving no supplements. The magnesium status of the group receiving supplements improved and their hyperactivity was significantly reduced, while hyperactive behaviour worsened in the control group.(25)
Andrew’s story is a classic example of how effective magnesium can be in helping restless, hyperactive children:
When he was three years old, Andrew’s sleep-deprived parents brought him to our Brain Bio Centre. He was hyperactive and seemed never to sleep. Not surprisingly, he was grumpy most of the time.
We recommended that his parents give him 65mg of magnesium daily in a pleasant-tasting powder added to a drink before bed. Two weeks later, his mum phoned to say that he was sleeping right through every night and had been transformed into a delightful child during the day too.
The four drivers of ADHD
Optimum nutrition has a big role to play in helping neurodivergent children.
Multi-nutrient trials have shown improvements in irritability, hyperactivity and self-harm.(26) Raised homocysteine and low B12 or folate are associated with greater risk of developing ASD and worse symptoms,(27) creating methylation abnormalities that could explain many of the symptoms (28). Supplementing homocysteine-lowering B vitamins makes symptoms better. (29)
Conditions like ADHD may be the result of either:
- a high-GL diet, with too much sugar
- a lack of essential omega-3 fats
- a lack of critical nutrients such as B vitamins, zinc and magnesium
- unidentified food intolerances.
Adolescents with blood sugar problems and diagnosed with metabolic syndrome, already show the same kind of cognitive deficiencies and hippocampal brain shrinkage found in adults with pre-dementia. (164)
That’s how important it is to stop children developing a sweet tooth.
Studies by Dr Alex Richardson from the University of Oxford, giving children with ADHD these vital brain fats, have shown an improvement in learning and the behavioural problems that define ADHD. (30) Her book They Are What You Feed Them, based on a lifetime of research, explains how diet affects children’s behaviour and learning.
Over in New Zealand, Professor Julia Rucklidge tested the effects of giving children aged 7 to 12 who had been diagnosed with ADHD a high-strength comprehensive multivitamin and mineral supplement, including plenty of B vitamins (B6 23mg, folate 267mcg, B12 300mcg, magnesium 200mg, zinc 16mg). A total of 47 children were given the supplement and 46 a placebo. At the end of the 10-week trial, almost four times more children (32 per cent versus 9 per cent) had shown a clinically meaningful improvement in their attention. Also, based on a clinician’s assessment and parent and teacher reports, those on micro-nutrients showed greater improvements in emotional regulation, aggression and general functioning compared to those on the placebo. (31)
Autism and the gut
Many children on the spectrum complain of gut problems. Some, though certainly not all, respond well to gluten and casein-free diets (32) My strong advice is to test a child for IgG-based food intolerance before embarking on a restrictive diet.
But it’s not just milk and wheat that can be a problem, nor do food intolerances only affect those with ASD.
Michael, a five-year-old we saw at the Brain Bio Centre, used to be so hyperactive that he could only go to school on a part-time basis.
He was unable to concentrate on anything, was disruptive in class and also found it difficult to socialize with other children. After taking a YorkTest 113 food intolerance test, Michael discovered he was intolerant to a range of foods, mainly dairy, wheat, oranges, carrots, soya, chicken and pork.
Staff at Michael’s school were amazed by the changes in his behaviour just one week after making the dietary changes. He could sit still and calmly draw pictures and went back to school on a full-time basis.
Putting all these pieces together, US researchers ran a 12-month study of a comprehensive nutritional and dietary intervention, enrolling 67 children and adults with autism spectrum disorder (ASD) aged 3–58 years and using 50 non-sibling neurotypical controls of similar age and gender. Treatment began with a comprehensive vitamin/mineral supplement, and additional treatments were added sequentially, including essential fatty acids, Epsom salts baths, carnitine, digestive enzymes and a healthy, gluten-free, casein-free, soy-free (HGCSF) diet. There was a major improvement in both autistic symptoms and non-verbal intellectual ability (non-verbal IQ) in the treatment group compared to the non-treatment group, with a gain of 7 IQ points. This is equivalent to what we found in the first vitamin IQ study back in 1987, when adolescents put on a B-vitamin-rich multivitamin had a 7-point increase in IQ compared to those on a placebo over seven months. (33)
Parents in the ASD study reported that the vitamin/mineral supplements, essential fatty acids and HGCSF diet were the most beneficial. (34)
I did a similar thing in a south London school for the BBC. They had challenged me to change the behaviour of disruptive kids in a week.
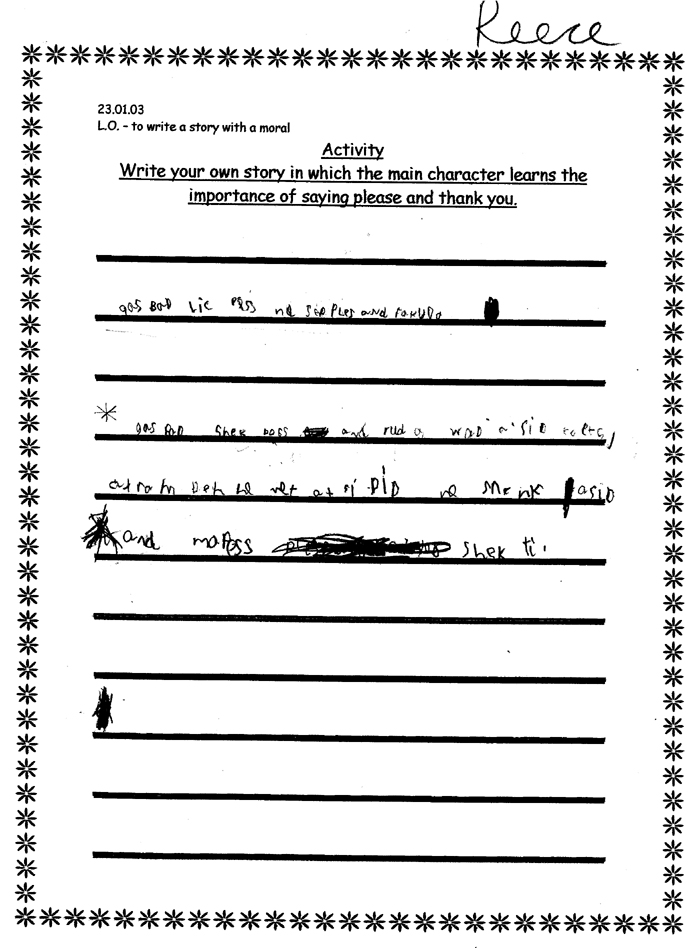
Of the 30 children, aged six to seven, the teacher said 10, roughly a third, were disruptive or had learning or behaviour problems. The worst was Reece. He couldn’t sit still or pay attention and was constantly getting into trouble.
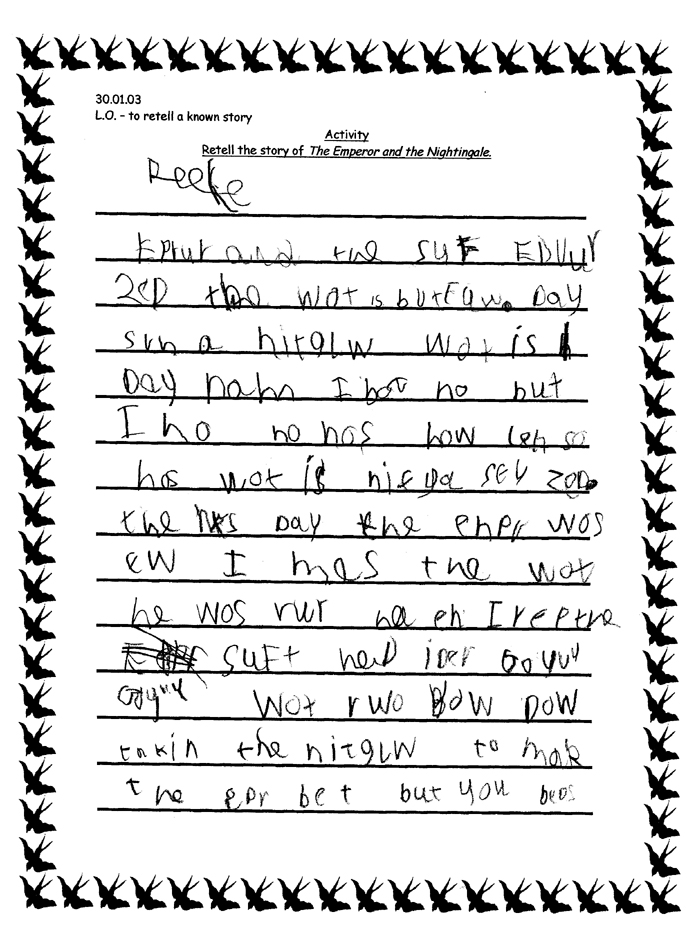
I enrolled Reece’s mother and the other parents in a one-week experiment in which they’d give their children no sweets or food with added sugar, additives or colourings, a drink containing vitamins and minerals, and try to eat more fish, fruit, vegetables, nuts and seeds. To measure change, the teacher asked the children to write a story on the day before we started and then again one week later. You can see the change in one week in Reece’s stories below.
In the following month, his reading and writing age went up by a year. Now able to sit still and concentrate, he went from close to the bottom of the class to close to the top. His parents noticed he was worse after eating Monster Munch, which contains monosodium glutamate. Some children are particularly sensitive to this flavour enhancer.
Reece’s handwriting before and after ‘optimum nutrition’
Dr Alessio Fasano, who is also both Professor of Paediatrics at Harvard Medical School and Professor of Nutrition at Harvard’s Chan School of Public Health, thinks something is going wrong in the gut, with many ASD children reporting gut problems, including diarrhoea, constipation, belching and excessive flatulence and dysbiosis indicated by an abnormal pattern of gut bacteria. (35)
His findings support a connection between metabolism, gastrointestinal physiology and complex behavioural traits. This has been confirmed by a small trial ‘cleansing’ the gut with an antibiotic, then giving ‘healthy’ faecal transplants to 18 children with ASD. (36) This resulted in significant improvements in constipation, diarrhoea, indigestion and abdominal pain, as well as behavioural ASD symptoms. The improvements persisted eight weeks after treatment.
In some children, wheat and milk may contribute to these symptoms. Professor Fasano’s research finds that neurodivergent children show high levels of zonulin, which can lead to leaky gut. (37) The gluten in wheat makes the zonulin levels go up.
ASD children have also been found to have opioid-like wheat and milk proteins in their urine, making these foods especially ‘addictive’. This was the discovery of researchers at the Autism Research Unit at the University of Sunderland, headed by Paul Shattock, now known as ESPA Research. They developed successful strategies for helping children with autism known as the Sunderland Protocol. (38)
Summary
In summary, to build healthy young brains and help prevent neurodivergence, including ADHD and autism, it is important for mothers-to-be, pregnant women and breastfeeding mothers and their children to:
- limit or avoid foods with added sugar and follow a low-GL diet
- avoid chemical colouring and flavour additives such as MSG
- optimize omega-3 intake, as phospholipids, from seafood and eggs, and supplement omega-3 DHA and EPA
- optimize vitamins A and D, with sufficient sun exposure to encourage good body stores of vitamin D
- ensure healthy methylation with B vitamins, especially vitamin B12 in vegans and those on a largely plant-based diet
- check for food intolerances, including gluten, if digestive symptoms are present.
Shape Your Child’s Future: Join COGNITION® For Smart Kids & Teens.
We don’t just want to share the research about how to upgrade your child’s brain, we want to help you do it! We are developing our COGNITION for Smart Kids & Teens and we need your help.
Thank you for reading!
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices.
Please support our research by becoming a Friend of Food for the Brain.
References
1 van Os J, Guloksuz S. Population Salutogenesis—The Future of Psychiatry? JAMA Psychiatry. Published online December 20, 2023. doi:10.1001/jamapsychiatry.2023.4582
3 Roigé-Castellví J, Murphy M, Fernández-Ballart J, Canals J. Moderately elevated preconception fasting plasma total homocysteine is a risk factor for psychological problems in childhood. Public Health Nutr. 2019 Jun;22(9):1615-1623. doi: 10.1017/S1368980018003610. Epub 2019 Jan 14. PMID: 30636652; PMCID: PMC10261079.
4. Hibbeln JR, Davis JM,] Steer C, Emmett P, Rogers I, Williams C, Golding J. Maternal seafood consumption in pregnancy and neurodevelopmental outcomes in childhood (ALSPAC study): an observational cohort study. Lancet. 2007 Feb 17;369(9561):578-85. doi: 10.1016/S0140-6736(07)60277-3. PMID: 17307104.
5. Z.Liu Behav Neurol. 2021 Dec 7;2021:5417497
6. McNulty H, Rollins M, Cassidy T, Caffrey A, Marshall B, Dornan J, McLaughlin M, McNulty BA, Ward M, Strain JJ, Molloy AM, Lees-Murdock DJ, Walsh CP, Pentieva K. Effect of continued folic acid supplementation beyond the first trimester of pregnancy on cognitive performance in the child: a follow-up study from a randomized controlled trial (FASSTT Offspring Trial). BMC Med. 2019 Oct 31;17(1):196. doi: 10.1186/s12916-019-1432-4. PMID: 31672132; PMCID: PMC6823954.
7. Wang Z, Ding R, Wang J. The Association between Vitamin D Status and Autism Spectrum Disorder (ASD): A Systematic Review and Meta-Analysis. Nutrients. 2020 Dec 29;13(1):86. doi: 10.3390/nu13010086. PMID: 33383952; PMCID: PMC7824115.
8. Patrick RP, Ames BN. Vitamin D and the omega-3 fatty acids control serotonin synthesis and action, part 2: relevance for ADHD, bipolar disorder, schizophrenia, and impulsive behavior. FASEB J. 2015 Jun;29(6):2207-22. doi: 10.1096/fj.14-268342. Epub 2015 Feb 24. PMID: 25713056.
9. Veena SR, Krishnaveni GV, Srinivasan K, Wills AK, Muthayya S, Kurpad AV, Yajnik CS, Fall CH. Higher maternal plasma folate but not vitamin B-12 concentrations during pregnancy are associated with better cognitive function scores in 9- to 10- year-old children in South India. J Nutr. 2010 May;140(5):1014-22. doi: 10.3945/jn.109.118075. Epub 2010 Mar 24. PMID: 20335637; PMCID: PMC3672847.
10. Qin B, Xun P, Jacobs DR Jr, Zhu N, Daviglus ML, Reis JP, Steffen LM, Van Horn L, Sidney S, He K. Intake of niacin, folate, vitamin B-6, and vitamin B-12 through young adulthood and cognitive function in midlife: the Coronary Artery Risk Development in Young Adults (CARDIA) study. Am J Clin Nutr. 2017 Oct;106(4):1032-1040. doi: 10.3945/ajcn.117.157834. Epub 2017 Aug 2. PMID: 28768650; PMCID: PMC5611785.
12. Montgomery P, Burton JR, Sewell RP, Spreckelsen TF, Richardson AJ. Low blood long chain omega-3 fatty acids in UK children are associated with poor cognitive performance and behavior: a cross-sectional analysis from the DOLAB study. PLoS One. 2013 Jun 24;8(6):e66697. doi: 10.1371/journal.pone.0066697. Erratum in: PLoS One. 2013;8(9). doi:10.1371/annotation/26c6b13f-b83a-4a3f-978a-c09d8ccf1ae2. PMID: 23826114; PMCID: PMC3691187.
13. Raine A, Ang RP, Choy O, Hibbeln JR, Ho RM, Lim CG, Lim-Ashworth NSJ, Ling S, Liu JCJ, Ooi YP, Tan YR, Fung DSS. Omega-3 (ω-3) and social skills interventions for reactive aggression and childhood externalizing behavior problems: a randomized, stratified, double-blind, placebo-controlled, factorial trial. Psychol Med. 2019 Jan;49(2):335-344. doi: 10.1017/S0033291718000983. Epub 2018 May 10. PMID: 29743128; see also Choy O, Raine A. Omega-3 Supplementation as a Dietary Intervention to Reduce Aggressive and Antisocial Behavior. Curr Psychiatry Rep. 2018 Apr 5;20(5):32. doi: 10.1007/s11920-018-0894-y. PMID: 29623453; see also Gow RV, Hibbeln JR. Omega-3 fatty acid and nutrient deficits in adverse neurodevelopment and childhood behaviors. Child Adolesc Psychiatr Clin N Am. 2014 Jul;23(3):555-90. doi: 10.1016/j.chc.2014.02.002. Epub 2014 May 27. PMID: 24975625; PMCID: PMC4175558.
15. Sonia L Robinson, Constanza Marín, Henry Oliveros, Mercedes Mora-Plazas, Betsy Lozoff, Eduardo Villamor, Vitamin D Deficiency in Middle Childhood Is Related to Behavior Problems in Adolescence, The Journal of Nutrition, Volume 150, Issue 1, 2020, pp.140–148, ISSN 0022-3166, https://doi.org/10.1093/jn/nxz185.
16. Megson MN. Is autism a G-alpha protein defect reversible with natural vitamin A? Med Hypotheses. 2000 Jun;54(6):979-83. doi: 10.1054/mehy.1999.0999. PMID: 10867750.
17. Zinc Affects Cognition and Psychosocial Function of Middle-School Children, April 2005, The FASEB Journal Conference: Experimental Biology
18. Rucklidge JJ, Eggleston MJF, Darling KA, Stevens AJ, Kennedy MA, Frampton CM. Can we predict treatment response in children with ADHD to a vitamin-mineral supplement? An investigation into pre-treatment nutrient serum levels, MTHFR status, clinical correlates and demographic variables. Prog Neuropsychopharmacol Biol Psychiatry. 2019 Mar 8;89:181–192. doi: 10.1016/j.pnpbp.2018.09.007. Epub 2018 Sep 12. PMID: 30217770.
20. Skalny AV, Mazaletskaya AL, Ajsuvakova OP, Bjørklund G, Skalnaya MG, Chao JC, Chernova LN, Shakieva RA, Kopylov PY, Skalny AA, Tinkov AA. Serum zinc, copper, zinc-to-copper ratio, and other essential elements and minerals in children with attention deficit/hyperactivity disorder (ADHD). J Trace Elem Med Biol. 2020 Mar;58:126445. doi: 10.1016/j.jtemb.2019.126445. Epub 2019 Dec 6. PMID: 31869738.
21. Joe P, Petrilli M, Malaspina D, Weissman J. Zinc in schizophrenia: A meta-analysis. Gen Hosp Psychiatry. 2018 Jul-Aug;53:19-24. doi: 10.1016/j.genhosppsych.2018.04.004. Epub 2018 Apr 27. PMID: 29727763.
22. Vidović B, Dorđević B, Milovanović S, Škrivanj S, Pavlović Z, Stefanović A, Kotur-Stevuljević J. Selenium, zinc, and copper plasma levels in patients with schizophrenia: relationship with metabolic risk factors. Biol Trace Elem Res. 2013 Dec;156(1-3):22-8. doi: 10.1007/s12011-013-9842-1. Epub 2013 Oct 24. PMID: 24150923.
23. Perham JC, Shaikh NI, Lee A, Darling KA, Rucklidge JJ. Toward ‘element balance’ in ADHD: an exploratory case control study employing hair analysis. Nutr Neurosci. 2022 Jan;25(1):11-21. doi: 10.1080/1028415X.2019.1707395. Epub 2020 Jan 3. PMID: 31900097.
24. Hemamy M, Pahlavani N, Amanollahi A, Islam SMS, McVicar J, Askari G, Malekahmadi M. The effect of vitamin D and magnesium supplementation on the mental health status of attention-deficit hyperactive children: a randomized controlled trial. BMC Pediatr. 2021 Apr 17;21(1):178. doi: 10.1186/s12887-021-02631-1. Erratum in: BMC Pediatr. 2021 May 12;21(1):230. PMID: 33865361; PMCID: PMC8052751.
25. B. Starobrat-Hermelin and T. Kozielec, ‘The effects of magnesium physiological supplementation on hyperactivity in children with attention deficit hyperactivity disorder (ADHD): Positive response to magnesium oral loading test’, Magnes Res, Vol 10(2), 1997, pp. 149-56
26. Mehl-Madrona L. Journal of Alternative and Complementary Medicine 2017 , 23(7), 526–533.
27. Li B, Xu Y, Pang D, Zhao Q, Zhang L, Li M, Li W, Duan G, Zhu C. Interrelation between homocysteine metabolism and the development of autism spectrum disorder in children. Front Mol Neurosci. 2022 Aug 15;15:947513. doi: 10.3389/fnmol.2022.947513. PMID: 36046711; PMCID: PMC9421079.
28. Antonio Belardo, Federica Gevi, Lello Zolla, The concomitant lower concentrations of vitamins B6, B9 and B12 may cause methylation deficiency in autistic children, The Journal of Nutritional Biochemistry, Volume 70, 2019, Pages 38-46, ISSN 0955-2863, https://doi.org/10.1016/j.jnutbio.2019.04.004; see also James SJ, Melnyk S, Fuchs G, Reid T, Jernigan S, Pavliv O, Hubanks A, Gaylor DW. Efficacy of methylcobalamin and folinic acid treatment on glutathione redox status in children with autism. Am J Clin Nutr. 2009 Jan;89(1):425-30. doi: 10.3945/ajcn.2008.26615. Epub 2008 Dec 3. PMID: 19056591; PMCID: PMC2647708.
29. Rossignol DA, Frye RE. The Effectiveness of Cobalamin (B12) Treatment for Autism Spectrum Disorder: A Systematic Review and Meta-Analysis. J Pers Med. 2021 Aug 11;11(8):784. doi: 10.3390/jpm11080784. PMID: 34442428; PMCID: PMC8400809; see also ref xx below; Adams JB, Audhya T, Geis E, Gehn E, Fimbres V, Pollard EL, Mitchell J, Ingram J, Hellmers R, Laake D, Matthews JS, Li K, Naviaux JC, Naviaux RK, Adams RL, Coleman DM, Quig DW. Comprehensive Nutritional and Dietary Intervention for Autism Spectrum Disorder-A Randomized, Controlled 12-Month Trial. Nutrients. 2018 Mar 17;10(3):369. doi: 10.3390/nu10030369. PMID: 29562612; PMCID: PMC5872787; see also James SJ, Melnyk S, Fuchs G, Reid T, Jernigan S, Pavliv O, Hubanks A, Gaylor DW. Efficacy of methylcobalamin and folinic acid treatment on glutathione redox status in children with autism. Am J Clin Nutr. 2009 Jan;89(1):425-30. doi: 10.3945/ajcn.2008.26615. Epub 2008 Dec 3. PMID: 19056591; PMCID: PMC2647708.
30. Yau PL, Castro MG, Tagani A, Tsui WH, Convit A. Obesity and metabolic syndrome and functional and structural brain impairments in adolescence. Pediatrics. 2012 Oct;130(4): e856–64. doi: 10.1542/peds.2012-0324. Epub 2012 Sep 3. PMID: 22945407; PMCID: PMC3457620; see also Mangone A, Yates KF, Sweat V, Joseph A, Convit A. Cognitive functions among predominantly minority urban adolescents with metabolic syndrome. Appl Neuropsychol Child. 2018 Apr-Jun;7(2):157-163. doi: 10.1080/21622965.2017.1284662. Epub 2017 Feb 22. PMID: 28631969
31. Richardson AJ. Review: ω-3 fatty acids produce a small improvement in ADHD symptoms in children compared with placebo. Evid Based Ment Health. 2012 May;15(2):46. doi: 10.1136/ebmental-2011-100523. Epub 2012 Feb 18. PMID: 22345102.
32. Rucklidge JJ, Eggleston MJF, Johnstone JM, Darling K, Frampton CM. Vitamin-mineral treatment improves aggression and emotional regulation in children with ADHD: a fully blinded, randomized, placebo-controlled trial. J Child Psychol Psychiatry. 2018 Mar;59(3):232-246. doi: 10.1111/jcpp.12817. Epub 2017 Oct 2. PMID: 28967099; PMCID: PMC7779340.
33. Piwowarczyk A, Horvath A, Łukasik J, Pisula E, Szajewska H. Gluten- and casein-free diet and autism spectrum disorders in children: a systematic review. Eur J Nutr. 2018 Mar;57(2):433-440. doi: 10.1007/s00394-017-1483-2. Epub 2017 Jun 13. PMID: 28612113.
34. Benton D, Roberts G. Effect of vitamin and mineral supplementation on intelligence of a sample of schoolchildren. Lancet. 1988 Jan 23;1(8578):140-3. doi: 10.1016/s0140-6736(88)92720-1. PMID: 2892988.
35. Adams JB, Audhya T, Geis E, Gehn E, Fimbres V, Pollard EL, Mitchell J, Ingram J, Hellmers R, Laake D, Matthews JS, Li K, Naviaux JC, Naviaux RK, Adams RL, Coleman DM, Quig DW. Comprehensive Nutritional and Dietary Intervention for Autism Spectrum Disorder-A Randomized, Controlled 12-Month Trial. Nutrients. 2018 Mar 17;10(3):369. doi: 10.3390/nu10030369. PMID: 29562612; PMCID: PMC5872787.
36. Needham BD, Adame MD, Serena G, Rose DR, Preston GM, Conrad MC, Campbell AS, Donabedian DH, Fasano A, Ashwood P, Mazmanian SK. Plasma and Fecal Metabolite Profiles in Autism Spectrum Disorder. Biol Psychiatry. 2021 Mar 1;89(5):451-462. doi: 10.1016/j.biopsych.2020.09.025. Epub 2020 Oct 10. PMID: 33342544; PMCID: PMC7867605.
37. Kang DW, Adams JB, Gregory AC, Borody T, Chittick L, Fasano A, Khoruts A, Geis E, Maldonado J, McDonough-Means S, Pollard EL, Roux S, Sadowsky MJ, Lipson KS, Sullivan MB, Caporaso JG, Krajmalnik-Brown R. Microbiota Transfer Therapy alters gut ecosystem and improves gastrointestinal and autism symptoms: an open-label study. Microbiome. 2017 Jan 23;5(1):10. doi: 10.1186/s40168-016-0225-7. PMID: 28122648; PMCID: PMC5264285.
38. Asbjornsdottir, Birna, et al. “Zonulin-dependent intestinal permeability in children diagnosed with mental disorders: a systematic review and meta-analysis.” Nutrients 12.7 (2020): 1982.
Further info