In a culture where the average plate still leans heavily towards meat – often processed, often excessive – it’s time to reassess the impact of our protein choices not just on our waistlines, but on our brains. A recent study in Neurology (2025) has added fresh weight to decades of evidence linking red and processed meat consumption to an increased risk of dementia and cognitive decline (1). Meanwhile, fish – particularly oily fish – continues to top the charts as the most protective food for your brain (2,3).
So, what does this mean practically for those of us trying to upgrade our brains and reduce our risk of cognitive decline? The answer may be as simple as this: eat more fish and fewer sausages.
Red Meat, Processed Meat and the Rising Risk to Brain Health
A new US cohort study, which followed over 77,000 adults across 30 years, found that:
Processed red meats (bacon, hot dogs, sausages, salami, bologna and other processed meat products) were clearly problematic. Consuming just 0.25 servings per day or more was associated with a 13% higher risk of developing dementia compared with those eating less than 0.1 serving (1).
Unprocessed red meat (e.g. beef or lamb) was linked to a 16% increased risk of subjective cognitive decline – that is people reporting that their memory or mental sharpness was worsening – when consuming more than one serving daily compared to less than half a serving per day. However, the researchers noted that this link did not reach statistical significance for diagnosed dementia overall (1).
More encouragingly, replacing one daily serving of processed red meat with a serving of nuts, lentils, or beans was associated with a 19% lower risk of dementia (1).
These findings are consistent with a large UK Biobank analysis of almost half a million adults, which found that each additional 25 g/day of processed meat (bacon, ham, sausages, meat pies, kebabs, burgers, chicken nuggets) was associated with a 44% higher risk of all-cause dementia and a 52% higher risk of Alzheimer’s disease. In contrast, each 50 g/day of unprocessed red meat was linked to a 19% lower risk of all-cause dementia and a 30% lower risk of Alzheimer’s disease (4). This reinforces the idea that it is the processing – not necessarily the meat itself – that may be most harmful.
These associations were observed regardless of whether participants carried the APOE ε4 gene variant – further evidence that dietary choices have a significant impact and that Alzheimer’s is ‘not in the genes’. (4).
The Global Pattern
The irrelevance of genetics in these findings is further supported by global evidence. An ecological analysis across 204 countries found that higher national per-capita total meat supply – including both red and white meats – was significantly associated with higher dementia incidence, even after adjusting for ageing, economic development and genetic risk, including APOE ε4 prevalence where available (5). In other words, the meat-dementia link is not confined to particular genetic subgroups but is observable across populations worldwide, suggesting that the way we produce and consume meat may be influencing brain health trends on a global scale.
What we put on our plate is powerful when it comes to reducing dementia risk – more so than any genetic variations that attract attention in the media.
Why Fish is Brain Food
The answer is not to go hungry, but to swap for something else – and when it comes to brain health, marine foods are your answer.
Unlike red meat, fish – especially oily varieties like salmon, sardines or mackerel – continue to show a strong protective effect.
A comprehensive 2024 meta-analysis found that:
Eating one to two servings of fish per day (roughly 150 g) is associated with a 20% reduced risk of Alzheimer’s disease and up to 30% slower cognitive decline (2).
Another study found that people who ate fish at least once a week had a one-third lower risk of Alzheimer’s compared with those eating fish less than weekly (3).
Why? Omega-3 fats, especially DHA, are critical for brain function and structure. They reduce inflammation, support synaptic plasticity and help clear beta-amyloid – a protein associated with Alzheimer’s disease.
As explained in the COGNITION™ 6-month programme, omega-3 fats from fish oil play a pivotal role in building and repairing the brain, particularly in mid-life, when early signs of cognitive decline can start to emerge.
That’s why we offer omega-3 at-home blood tests – so you can check whether you’re getting enough through your diet or if it’s time to add a supplement. You can test omega-3 on its own here, or as part of our5-in-1 DRIfT testwhere you can also check your homocysteine and glutathione status at the same time.
A Simple Swap with Profound Impact
From a cognitive health perspective, the data is now hard to ignore: if you’re regularly eating red or processed meat – especially more than once a day – your brain may be paying the price. But shifting even one of those servings towards fish, eggs or plant-based proteins could make a meaningful difference.
Interestingly, the main culprit in the latest studies was processed meat. This supports a key principle in brain-friendly eating: most natural whole foods – whether meat, fish, fruit, nuts, legumes, wholegrains or dairy – are not the problem. It’s when we distort them into ultra-processed, factory-made food that health is undermined.
This isn’t about becoming vegan or pescatarian. It’s simply more evidence to reduce processed foods and ensure optimalomega-3 intake.
So next time you’re at the supermarket make a cow happy and buy a fish.
Resources:
Need help knowing what to eat? Get inspired with over 125 brain-friendly recipes in the Upgrade Your Brain Cook App.
Order your omega-3 test today to find out if you are eating enough of these essential fatty acids. You can test omega-3 on its own here, or as part of our5-in-1 DRIfT test. Available globally.
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
References:
You J, Zhang L, Zhou Y, et al. Total meat supply and incidence of dementia: an ecological study of 204 countries. Front Public Health. 2025;13:1589936. doi:10.3389/fpubh.2025.1589936.
Li Y, Li Y, Gu X, Liu Y, Dong D, Kang JH, Wang M, Eliassen H, Willett WC, Stampfer MJ, Wang D. Long-Term Intake of Red Meat in Relation to Dementia Risk and Cognitive Function in US Adults. Neurology. 2025;104(3):e210286. doi:10.1212/WNL.0000000000210286.
Godos J, Micek A, Currenti W, Franchi C, Poli A, Battino M, Dolci A, Ricci C, Ungvari Z, Grosso G. Fish consumption, cognitive impairment and dementia: an updated dose-response meta-analysis of observational studies. Aging Clin Exp Res. 2024;36(1):171-182. doi:10.1007/s40520-024-02823-6.
Beydoun MA, Beydoun HA, Gamaldo AA, Teel A, Zonderman AB, Wang Y. Epidemiologic studies of modifiable factors associated with cognition and dementia: systematic review and meta-analysis. BMC Public Health. 2014;14:643. doi:10.1186/1471-2458-14-643.
Zhang Z, He P, Liu M, et al. Meat consumption and risk of incident dementia: cohort study of UK Biobank participants. Am J Clin Nutr. 2021;113(5):1228-1236. doi:10.1093/ajcn/nqaa343.
Imagine if a simple, well-researched nutrient protocol could prevent cognitive decline in millions of people worldwide. Imagine further that this protocol has been known for years, supported by multiple clinical trials and global experts, yet systematically ignored by the very institutions meant to protect public health. That is precisely the case when it comes to homocysteine, B vitamins, and dementia.
Last year, the UK-based Lancet Commission on Dementia Prevention, Intervention and Care released its third major report, once again omitting any mention of homocysteine as a modifiable risk factor. This was despite direct submissions of evidence and letters from leading scientists demonstrating that lowering homocysteine with B vitamins can slow brain shrinkage and cognitive decline.
Now, in response to this silence, six of the leading dementia researchers, Professors Joshua Miller (Rutgers), David Smith (Oxford), Helga Refsum (Oslo), Jin-Tai Yu (Fudan), Babak Hooshmand (Karolinska), and Andrew McCaddon (Wrexham), have published a powerful rebuttal in the Journal of Alzheimer’s Disease. Many of these experts serve in the Alzheimer’s Prevention Expert Group (APEG) at Food for the Brain.
They wrote:
“In 2018, we published an ‘International Consensus Statement on Homocysteine and Dementia’ in this journal, in which we concluded that elevated plasma total homocysteine is a modifiable risk factor for the development of cognitive decline, dementia, and Alzheimer’s disease (AD) in older persons. (1)
We further stated that intervention trials in elderly people with cognitive impairment show that homocysteine-lowering treatment with B vitamins markedly slows the rate of both wholeand regional brain atrophy, and also slows cognitive decline. We were therefore puzzled as to why the Lancet Commission on Dementia Prevention, Intervention and Care, failed to discuss the possible role of homocysteine and B vitamins in any of their three reports, including the most recent one.” (2)
A Systematic Omission
The UK-based Lancet Commission on Dementia Prevention is meant to objectively consider the evidence on dementia prevention. Yet each edition, despite being sent the relevant papers, has ignored the evidence concerning homocysteine.
Furthermore, it’s expected to uphold the standards for critical debate which allows for experts to question Published findings. That is exactly what these experts did – yet it declined to publish their letter, instead printing a rebuttal from its own Commission while refusing to let readers see the original letter. (3, 4)
The experts wrote to The Lancet again to respond to the Commission’s letter, but their second letter was also rejected.
Thatetter has now been published in the leading Alzheimer’s journal where the authors finally have their rightful say. It includes the following:
“We wish to reply to the Commission and continue the debate with the aim of reaching a common view on homocysteine, B vitamins and dementia. This is an important matter of public health.”
In other words, The Lancet published the ‘case for the defence’ for the exclusion of homocysteine without allowing readers to even read the ‘case for the prosecution’. (5)
So, what was The Lancet’s case against B vitamins? It rested on three criticisms – each of which these leading dementia researchers refute with scientific precision in their recent journal paper.
Criticism 1: Misunderstanding Who Benefited in the VITACOG Trial
The Lancet Commission questioned the relevance of the VITACOG trial, arguing that the results “do not show benefits in populations already consuming B vitamins in their food or through supplements.” But this fundamentally misrepresents the study population.
In the VITACOG trial, participants with mild cognitive impairment were given high doses of B6, B12, and folic acid for two years. The result was a 31% reduction in whole brain shrinkage and significantly slower rate of cognitive decline in those with raised homocysteine (6). In participants with levels above 11.3 μmol/L – the median – both cognitive and clinical improvements were observed. Importantly, key Alzheimer’s-related brain regions shrank seven times more slowly in these individuals (7, 8).
The Lancet Commission implied that participants were already supplementing, but that is incorrect. The study excluded anyone taking more than 300 mcg of folic acid, 3 mg of vitamin B6, or 1.5 mcg of vitamin B12 – doses lower than those found in many common multivitamins. Only 16 to 20 percent were taking low-dose supplements, while the majority were not.. No one was excluded based on their dietary intake of B vitamins.
The experts respond:“The Commission authors’ comment is analogous to expecting additional drug treatment to provide benefits over and above the benefits being obtained in people already taking a high dose of the drug, which is why it puzzles us.”
Criticism 2: No Benefit in the Hong Kong Trial?
The Commission’s response also cited a Hong Kong trial that reported no benefit of B vitamins over two years in people with mild cognitive impairment (MCI) (9). However, this overlooks several important confounders.
Firstly, 22% of participants were taking aspirin, which the study authors themselves found to impair the effect of B vitamins. This interference has since been confirmed in further research (10).
Secondly, the authors of The Lancet response failed to consider another critical factor: omega-3 status. Numerous studies show that B vitamins only deliver cognitive benefits when omega-3 fatty acid levels are sufficient. The Hong Kong study did not measure or control for omega-3 status, which likely explains the lack of consistent benefit over the two-year period.
Thus, the absence of effect in this trial does not disprove the role of B vitamins. The experts go on to demonstrate in their article the overwhelming body of evidence – reported by us – that homocysteine-lowering B vitamins do not work optimally in individuals with low omega-3 status.
Criticism 3: No Benefit in the VITAL Trial in Alzheimer’s Patients?
The Lancet authors also referenced the VITAL trial, which reported no overall cognitive benefit from B vitamins in patients already diagnosed with Alzheimer’s disease (11). But again, this conclusion overlooks key details.
In a subgroup analysis, those in the early stages of Alzheimer’s disease did show significant benefit (12). The authors of the VITAL trial themselves highlighted this in their paper, suggesting that earlier intervention is more effective. This finding aligns with multiple other studies showing that B vitamin treatment is most effective in the pre-dementia stages (13).
Furthermore, participants in the VITAL trial began with an average homocysteine level of 9 μmol/L, which is below the threshold (>10–11 μmol/L) associated with brain atrophy. It is extremely rare to find a group of people with Alzheimer’s disease that start with such a low homocysteine level. While the B vitamins did reduce homocysteine further to 7μmol/L, there was no overall cognitive benefit observed. But this is akin to giving painkillers to people who are not in pain and then reporting no change in pain levels. At Food for the Brain, we consider a homocysteine level above 10μmol/L as in need of correction with B vitamins.
There are also concerns about conflicts of interest. The lead author, Paul Aisen, is described as “a consultant to the following pharmaceutical companies involved in the development of potential treatments for Alzheimer’s disease”. with more than a dozen firms listed. These companies would certainly favour a trial designed to fail – especially if it were widely publicised.
Additionally, when an anti-amyloid drug trial for lecanemab was published – now licensed in the US and UK – the names of Paul Aisen and Christopher Van Dyck appeared once again as lead authors. In other words, the paid pharmaceutical consultants, responsible for running the drug trial were also tasked with overseeing a trial – designed to fail – on a competing approach: lowering homocysteine with B vitamins. The conflict of interest here is both clear and concerning.
What Does the Evidence Really Say?
You can read the full expert response published in the Journal of Alzheimer’s Diseasehere.
Their conclusion is clear:
“We hope that the Lancet Commission will consider the substantial existing evidence of raised homocysteine as an important risk factor for dementia and the possibility of modifying its harm by supplementation with B vitamins.”
They emphasise that the evidence for B vitamin intervention is as strong – or stronger than – many of the risk factors the Commission did include in its 2024 report. To continue ignoring the proven impact of homocysteine, and the benefits of lowering it through B vitamins is not merely a scientific oversight – it is a missed opportunity with major implications for medicine and public health.
Remember, prevention is better than cure, and there is so much you can do to protect your brain health
The perfect time to start? Today.
What Can You Do?
Test your homocysteine (and omega-3 status) TODAY – especially if you’re over 50 or at risk of cognitive decline. At Food for the Brain, we offer an accurate at-home test kit that reliably measures plasma homocysteine reliably.
You can order your single Homocysteine test here or save money and test both omega-3 index and homocysteine (plus other markers) as part of ourDRIfT tests here. International shipping available.
Act on your results – if your level is above 10 μmol/L, supplementation with vitamin B6 (20 mg), methylfolate (400 µg), and vitamin B12 (500 µg) is recommended. Read more on supplements and homocysteine here.
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
References
1. Smith AD, Refsum H, Bottiglieri T, et al. Homocysteine and dementia: an international consensus statement. J Alzheimers Dis 2018; 62: 561–570.
2.Livingston G, Huntley J, Liu KY, et al. Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission. Lancet 2024; 404: 572–628.
3.Miller JW, McCaddon A, Hooshmand B, et al. The Lancet ‘Omission’: Why are homocysteine and B vitamins missing from the Lancet Commission’s Report on Dementia Prevention, Intervention and Care? https://foodforthebrainorg/lancet-commission-letters/ (2024).
4.Livingston G, Costafreda SG, Kivimaki M, et al. B vitamins and the 2024 Lancet Commission on dementia. Lancet 2025; 405: 623.
5. Miller JW, McCaddon A, Yu J-T, Hooshmand B, Refsum H, Smith AD. Concerning the debate about homocysteine, B vitamins, and dementia. Journal of Alzheimer’s Disease. 2025;0(0). doi:10.1177/13872877251350297
6. Smith AD, Smith SM, de Jager CA, et al. Homocysteine-lowering by B vitamins slows the rate of accelerated brainatrophy in mild cognitive impairment. A randomized controlled trial. PLoS One 2010; 5: e12244.
7. de Jager CA, Oulhaj A, Jacoby R, et al. Cognitive and clinical outcomes of homocysteine-lowering B-vitamin treatment in mild cognitive impairment: a randomized controlled trial. Int J Geriatr Psychiatry 2012; 27: 592–600.
8. Douaud G, Refsum H, de Jager CA, et al. Preventing Alzheimer’s disease-related gray matter atrophy by B-vitamin treatment. Proc Natl Acad Sci U S A 2013; 110: 9523–9528.
9. Kwok T, Wu Y, Lee J, et al. A randomized placebo- controlled trial of using B vitamins to prevent cognitive decline in older mild cognitive impairment patients. ClinNutr 2020; 39: 2399–2405.
10. Wu Y, Smith AD, Refsum H, et al. Effectiveness of B vitamins and their interactions with aspirin in improving cognitive functioning in older people with mild cognitive impairment: pooled post-hoc analyses of two randomized trials. J Nutr Health Aging 2021; 25: 1154–1160.
11. Aisen PS, Schneider LS, Sano M, et al. High-dose B vitamin supplementation and cognitive decline in Alzheimer disease: a randomized controlled trial. JAMA 2008; 300: 1774–1783.
12. Smith AD and Homocysteine RH. B vitamins, and cognitive impairment. Ann Rev Nutr 2016; 36: 211–239.
13. Chen H, Liu S, Ge B, et al. Effects of folic acid and vitamin B12 supplementation on cognitive impairment and inflammation in patients with Alzheimer’s disease: a randomized, single-blinded, placebo-controlled trial. J Prev Alzheimers Dis 2021; 8: 249–256.
The reason we advocate natural, nutritional, and lifestyle-based approaches to mental health is simple – because they work, and they’re safe.
Unspoken Risks of Psychiatric & Dementia Drugs
The next big challenge is to discover which combination of changes has the most impact. This is what our research is focused on.
From depression to dementia, the typical approach is still, all too often, medication While it’s valid to compare a nutrient or diet to a pharmaceutical – take omega-3s, for example, which have been shown to be as effective as antidepressants – the real concern is how rarely we hear about the risks of psychiatric drugs. For many, by the time those dangers become clear, it’s already too late.
A classic example of this is the well-known increased risk of suicide particularly in young people prescribed antidepressants. Not only did this take more than ten years to ‘come out’, even now, despite on-the-box warnings, many remain unaware of this well-established risk.
A similar situation is emerging with the new anti-amyloid antibody treatments being proposed for dementia sufferers. Reported deaths are often downplayed or not fully disclosed.. In trials of the two drugs Lecanemab and Donanemab, eight deaths were reported. Eight deaths were reported during the trials, which involved 1,785 participants – a rate of one in every 219 – though not all were officially attributed to the drug. That’s quite a risk. But it is also the nature of these deaths, caused by brain bleeding and swelling, that is even more concerning.
Investigative journalist Charles Piller, in his book ‘Doctored’, interviewed the pathologist for the first Lecanemab death who said it was like “her brain exploded”. Another Lecanemab associated death was a 65 year-old woman, who had a blood clot induced stroke and was given a common, often lifesaving intervention (tPA) which went badly wrong. “As soon as they put it in her, it was like her body was on fire,” the woman’s husband told me, he said. “She was screaming, and it took, like, eight people to hold her down. It was horrific. Everybody’s running in and (asking) ‘What the hell is going on?’” His wife was sedated and recovered to intensive care, he said. Soon the woman suffered seizures and was placed on a ventilator. After a few days the family approved disconnecting the device and she died. In his book Piller also reports another case in which a participant ‘died after hideous brain swelling and bleeding, and violent seizures.’
The UK has licensed the use of Lecanemab. The EU has not. The UK has licensed Donanemab, but NICE hasn’t approved it for NHS use.
Safer, Evidence-Based Alternatives
Despite more effective and safer alternatives being available, Alzheimer’s charities continue to advocate for NHS access to these drugs. This raises an important question: why? The combination of homocysteine-lowering B vitamins and omega-3 already has stronger evidence of efficacy – with no adverse effects – and certainly no risk of death (Read Alzheimer’s: Prevention is the Cure for the evidence and the comparison).
We invited Dr Peter Gøtzsche – co-founder of the Cochrane Collaboration, originally established to evaluate health treatments without bias – to speak about the risks of psychiatric drugs and their link to mortality. When the Cochrane Collaboration became corrupted, which he later criticised for being influenced by commercial interests, he founded the Institute for Scientific Freedom.
“Overtreatment with drugs kills many people, and the death rate is increasing. It is therefore strange that we have allowed this long-lasting drug pandemic to continue, and even more so because most of the drug deaths are easily preventable.” he says.
“In 2013, I estimated that our prescription drugs are the third leading cause of death after heart disease and cancer,(1)and in 2015, that psychiatric drugs alone are also the third leading cause of death”.(2)”
Read on to understand how he arrived at the conclusion that psychiatric drugs may be the third leading cause of death.
How many people are killed by psychiatric drugs?
If we want to estimate the death toll of psychiatric drugs, the most reliable source of data comes from placebo-controlled randomised trials. However, we need to consider their limitations.
First, these trials typically last just a few weeks, despite the fact that most patients take psychiatric medications for many years.(3, 4)
Second, polypharmacy – the use of multiple medications – is common in psychiatry, and this significantly increases the risk of mortality.. As an example, the Danish Health Authority has warned that adding a benzodiazepine to a neuroleptic increases mortality by 50-65% (5).
Third, up to half of all deaths go unreported in published clinical trial data.(6) For dementia, published data shows that for every 100 people treated with a newer neuroleptic for ten weeks, one patient dies as a result. (7) This represents a high mortality rate for a pharmaceutical intervention, but FDA data on the same trials show it is double this number, equivalent to two deaths per 100 people over ten weeks. (8) And if we extend the observation period, the death toll becomes even higher. A Finnish study of 70,718 community-dwellers newly diagnosed with Alzheimer’s disease reported that neuroleptics kill 4-5 people per 100 annually, compared to patients who were not treated.(9)
Fourth, the design of psychiatric drug trials is biased. In almost all cases, patients were already in treatment with psychiatric medication before they entered the trial, (1, 2), and some of those randomised to placebo will therefore experience withdrawal effects that will increase their risk of dying, due to withdrawal symptoms such as akathisia. Placebo-controlled trials in schizophrenia cannot be reliably used to assess the effect of neuroleptics on mortality because of the drug withdrawal design. The suicide rate in these unethical trials was 2-5 times higher than the norm. (10,11) Among those enrolled in trials of risperidone, olanzapine, quetiapine, and sertindole, one in every 145 patients died. However, none of these deaths were mentioned in the published scientific literature, and the FDA did not require their inclusion in trial reporting.
Fifth, events occurring after the trial period are often ignored. In Pfizer’s trials of sertraline in adults, the risk ratio for suicides and suicide attempts was 0.52 when follow-up lasted only 24 hours, but increased to 1.47 when follow-up was extended to 30 days — indicating a rise in suicidal events. (12) Furthermore, when researchers reanalysed the FDA trial data on depression drugs and included harms occurring during follow-up, they found that antidepressants were associated with twice the number of suicides in adults compared to placebo (13, 14)
Estimating the True Death Toll of Mental-Health Medications
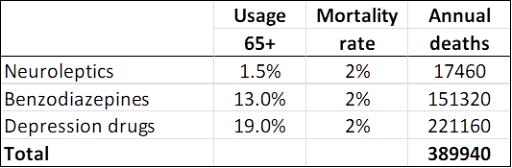
In 2013, I estimated that, in people aged 65 and above, neuroleptics, benzodiazepines or similar, and antidepressants kill 209,000 people annually in the United States.(2) I used relatively conservative estimates, however, and usage data from Denmark, which is far lower than those in USA. I have therefore updated the analysis based on US usage data, again focusing on older age groups.
For neuroleptics, I used the estimate of 2% mortality from the FDA data.(8)
For benzodiazepines and similar drugs, a matched cohort study showed that the drugs doubled the death rate, although the average age of the patients was only 55.(15) The excess death rate was about 1% per year. In another large, matched cohort study, the appendix to the study report shows that hypnotics quadrupled the death rate (hazard ratio 4.5). The study authors estimated that sleeping pills kill between 320,000 and 507,000 Americans every year. (16) A reasonable estimate of the annual death rate would therefore be 2%.
For SSRIs, a UK cohort study of 60,746 depressed patients older than 65 showed that they led to falls and a 3.6% annual mortality rate among those treated.(17) The study was well-designed, in that the patients were their own control in one of the analyses, which helps control for confounding variables. Nonetheless, the reported death rate is notably high.
Another cohort study, of 136,293 American postmenopausal women (age 50-79) participating in the Women’s Health Initiative study, found that depression drugs were associated with a 32% increase in all-cause mortality after adjustment for confounding factors, which corresponding to an estimated 0.5% annual mortality rate among women treated with SSRIs.(18). The authors noted that the mortality rate was likely underestimated. The authors warned that their results should be interpreted with great caution due to a high risk of exposure misclassification, which would make it more difficult to find an increase in mortality. Further, the patients were much younger than in the UK study, and the death rate increased markedly with age and was 1.4% for those aged 70-79. Finally, the exposed and unexposed women were different for many important risk factors for early death, whereas the people in the UK cohort were their own control.
For these reasons, I decided to use the average of the two estimates, a 2% annual death rate.
These are my results for USA for these three drug groups for people at least 65 years of age (58.2 million; usage is in outpatients only): (19, 20, 21, 22)
—
A limitation in these estimates is that you can only die once, and many people receive polypharmacy. It is not clear how we should adjust for this. In the UK cohort study of depressed patients, 9% also took neuroleptics, and 24% took hypnotics/anxiolytics. (17)
On the other hand, the data on death rates come from studies where many patients were also on several psychiatric drugs in the comparison group, so this is not likely to be a major limitation considering also that polypharmacy increases mortality beyond what the individual drugs cause.
Statistics from the Centers for Disease Control and Prevention list these four top causes of death: (23)
COVID-19 deaths are rapidly declining, and many of such deaths are not caused by the virus but merely occurred in people who tested positive for it because the WHO advised that all deaths in people who tested positive should be called COVID deaths.
Young people have a much smaller death risk than the elderly, as they rarely fall and break their hip, which is why I have focused on the elderly. I have tried to be conservative. My estimate misses many drug deaths in those younger than 65 years; it only included three classes of psychiatric drugs; and it did not include hospital deaths.
I therefore do not doubt that psychiatric drugs are the third leading cause of death after heart disease and cancer.
—
Learn more and begin your brain upgrade journey today:
Order Alzheimer’s: Prevention is the Cure book here
Contribute to our research and order your accurate, at home, blood tests here.
If you are looking for personalised one to one support, visit the Brain Bio Centre here.
—
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
References: 1 Gøtzsche PC. Deadly medicines and organised crime: How big pharma has corrupted health care. London: Radcliffe Publishing; 2013.
2 Gøtzsche PC. Deadly psychiatry and organised denial. Copenhagen: People’s Press; 2015.. US News 2016; Sept 27.
2. Gøtzsche PC. Mental health survival kit and withdrawal from psychiatric drugs. Ann Arbor: L H Press; 2022.
3 Gøtzsche PC. Long-term use of antipsychotics and antidepressants is not evidence-based. Int J Risk Saf Med 2020;31:37-42.
4 Gøtzsche PC. Long-term use of benzodiazepines, stimulants and lithium is not evidence-based. Clin Neuropsychiatry 2020;17:281-3.
5 Forbruget af antipsykotika blandt 18-64 årige patienter, med skizofreni, mani eller bipolar affektiv sindslidelse. København: Sundhedsstyrelsen; 2006.
6 Hughes S, Cohen D, Jaggi R. Differences in reporting serious adverse events in industry sponsored clinical trial registries and journal articles on antidepressant and antipsychotic drugs: a cross-sectional study. BMJ Open 2014;4:e005535.
7 Schneider LS, Dagerman KS, Insel P. Risk of death with atypical antipsychotic drug treatment for dementia: meta-analysis of randomized placebo-controlled trials. JAMA 2005;294:1934–43.
8 FDA package insert for Risperdal (risperidone). Accessed 30 May 2022.
9 Koponen M, Taipale H, Lavikainen P, et al. Risk of mortality associated with antipsychotic monotherapy and polypharmacy among community-dwelling persons with Alzheimer’s disease. J Alzheimers Dis 2017;56:107-18.
10 Whitaker R. Lure of riches fuels testing. Boston Globe 1998;Nov 17.
11 Whitaker R. Mad in America: bad science, bad medicine, and the enduring mistreatment of the mentally ill. Cambridge: Perseus Books Group; 2002:page 269.
12 Vanderburg DG, Batzar E, Fogel I, et al. A pooled analysis of suicidality in double-blind, placebo-controlled studies of sertraline in adults. J Clin Psychiatry 2009;70:674-83.
13 Hengartner MP, Plöderl M. Newer-generation antidepressants and suicide risk in randomized controlled trials: a re-analysis of the FDA database. Psychother Psychosom 2019;88:247-8.
14 Hengartner MP, Plöderl M. Reply to the Letter to the Editor: “Newer-Generation Antidepressants and Suicide Risk: Thoughts on Hengartner and Plöderl’s ReAnalysis.” Psychother Psychosom 2019;88:373-4.
15 Weich S, Pearce HL, Croft P, et al. Effect of anxiolytic and hypnotic drug prescriptions on mortality hazards: retrospective cohort study. BMJ 2014;348:g1996.
16 Kripke DF, Langer RD, Kline LE. Hypnotics’ association with mortality or cancer: a matched cohort study. BMJ Open 2012;2:e000850.
17 Coupland C, Dhiman P, Morriss R, et al. Antidepressant use and risk of adverse outcomes in older people: population based cohort study. BMJ 2011;343:d4551.
18 Smoller JW, Allison M, Cochrane BB, et al. Antidepressant use and risk of incident cardiovascular morbidity and mortality among postmenopausal women in the Women’s Health Initiative study. Arch Intern Med 2009;169:2128-39.
There is no doubt that autism diagnoses, both across the UK and US are escalating at a worrying rate.
A clear illustration of this is the recently published Scottish Schools Census, showing a year by year steady increase in the percentage of Scottish schoolchildren with a diagnosis. Last year, one in 21 schoolchildren had an autism diagnosis, of which one in 14 are boys. This represents a 43-fold increase in 20 years.
As discussed at Food for theBrain’s Smart Kids conference, research is consistently showing that serum homocysteine, which you cantest with us at home here, is a reliable indicator of both folate and B12 status and with each unit increase in homocysteine pre-conceptually, the core symptoms required for an autism diagnosis go up. (1)
The majority of studies show that lack of pre-natal folic acid supplementation or low folate, increase the risk of aspects of neurodivergence. Studies on B12 are less clear however. Further studies are under way which will help determine both the optimal level of folate and B12 and whether they are synergistic, as has been found in Alzheimer’s prevention. Our view is that homocysteine should be measured and high levels lowered with appropriate diet and supplementation.
A recent study of 3,000 EU children reported that one third had B12 levels below 200pg/ml, (2) with deficiency more prevalent in vegan children. Another EU survey reports than only one in ten overweight women supplement folic acid in pregnancy. This is really concerning.
—
It’s the total load – not just one thing
The over-arching theme of this excellent conference was that of ‘total load’ and the interaction between predisposing genes and a nutritional deficient diet and/or toxic overload. It stressed the need to think in terms of the ‘total load’ on a child at critical stages of development, starting in pregnancy. A study of 192 twin pairs, published in the Archives of General Psychiatry, concluded that environmental factors were a greater contributor than heritability, contributing 55% of risk (3).
Additionally, there are many gene variations which don’t cause, but do increase the risk of neurodivergence. An example is a methylation gene variant MTHFR677TT, which increases risk for both autism and Alzheimer’s. Healthy methylation requires B vitamins, especially vitamin B12 and folate, found in ‘foliage’ – vegetables and greens. A study in China in the journal ‘Frontiers in Paediatrics’(4), comparing several thousand with or without this gene variation found that having it “… was associated with the increased risk of autism. For those mothers and children who are generally susceptible to autism, prenatal folate and vitamin B12 may reduce the risk that children suffer from autism.” This is just one example of the gene-environment interplay.
The results of a survey by the Autism Research Institute of over 27,000 parents who rated different nutritional interventions they tried, rating whether their child got better or worse, reported some clear winners of diet changes and supplements. The following had 10:1 or better ratings.
Removed milk/dairy 32:1
Removed wheat 30:1
Essential fatty acids 30:1
Removed chocolate 28:1
Removed sugar 27:1
Food allergy treatment 27:1
Feingold diet (no wheat or milk) 26:1
Zinc 24:1
Rotation diet 23;1
Candida diet 20:1
Removed eggs 20:1
Vitamin C 20:1
Vitamin A 16:1
Cod liver oil 14:1
Vitamin B6/magnesium 11:1
Specific carbohydrate diet 10:1
—
‘Life-changing’ improvement through dietary changes…
Another parent-reporting survey conducted by the UK charity Thinking Autism in 2014 (5), involving similar dietary guidance, and written up into a report by academics at Queen Mary, University of London in 2016, found that, out of 237 families who reported using various dietary interventions with their children with autism, 170 families reported either ‘life-changing’ or ‘significant’ improvements, while only 12 children were reported as having no noticeable change.
If you are a practitioner and would like a deep dive into theSmart Kids conference, recordings are now available.
If you are a parent or are neurodivergent yourself and would like to hear from clinicians who have considerable experience in helping those with symptoms get better, the Optimising Neurodivergence webinar is now available.
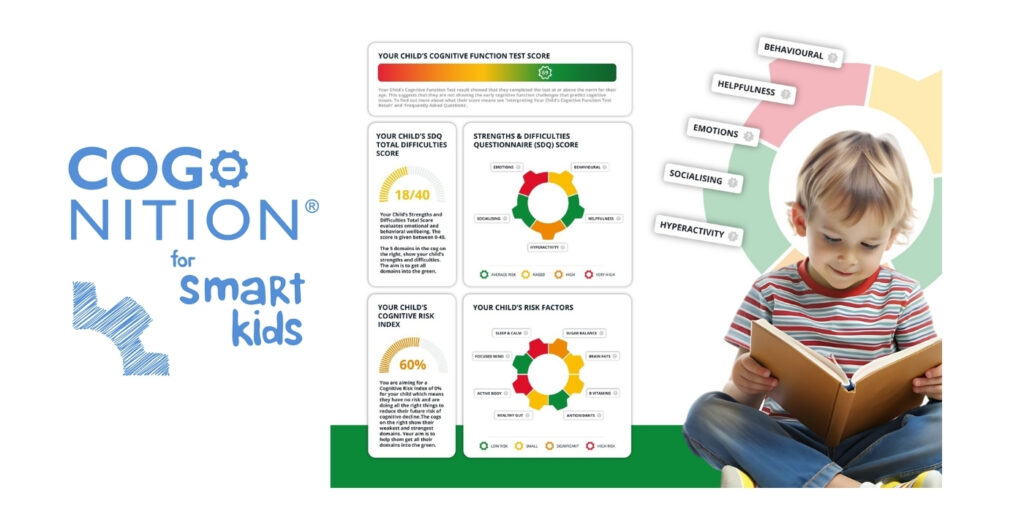
But first, do complete the COGNITION for Smart Kidstest (or the COGNITION testif you are a parent or practitioner) to help both our research and help yourself at the same time.
Here’s an example report.
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
References:
1 Roigé-Castellví J, Murphy M, Fernández-Ballart J, Canals J. Moderately elevated preconception fasting plasma total homocysteine is a risk factor for psychological problems in childhood. Public Health Nutr. 2019 Jun;22(9):1615-1623. doi: 10.1017/S1368980018003610. Epub 2019 Jan 14. PMID: 30636652; PMCID: PMC10261079. 2 Kara İS, Peker NA, Dolğun İ, Mertoğlu C. Vitamin B12 Level in Children. J Curr Pediatr. 2023 Aug;21(2):127-134. doi:10.4274/jcp.2023.75688. 3 https://pmc.ncbi.nlm.nih.gov/articles/PMC4440679/ 4 https://pmc.ncbi.nlm.nih.gov/articles/PMC7987783/ 5 https://www.thinkingautism.org.uk/taking-action/resources-and-publications/health-and-service-provision-for-people-with-autism/
Recently, the Telegraph reported: “Statins can reduce the risk of dementia among those who already have low cholesterol.” The article claimed that those on statins were less likely to develop dementia – even Alzheimer’s – and that low LDL cholesterol was somehow protective.
Frankly, this is dangerous misinformation.
Why? Because it contradicts robust scientific evidence that low cholesterol – particularly below 4 mmol/l – increases the risk for dementia. That’s hardly surprising when you consider that 25% of the cholesterol in your body is in your brain. Cholesterol is a vital component of neuronal membranes – it’s not just blood fat, it’s brain fuel.
And as for statins? There’s no credible evidence that they prevent dementia. Quite the opposite: the evidence points to statins lowering brain-essential cholesterol and raising dementia risk. So I asked cholesterol expert Dr Malcolm Kendrick for his take on the study in question.
His response was blunt but justified: “This study is horseshit. Here’s why…”
Dr Kendrick Key Critiques:
LDL measurement was vague. It’s unclear if they even measured LDL directly- most studies use the Friedewald formula, known to be wildly inaccurate, especially with high triglycerides or low HDL.
Only one measurement. LDL was recorded once at the study’s start – never again. That’s like measuring someone’s blood pressure once and claiming to predict their lifetime stroke risk.
Bizarre cohort overlap. Somehow, 170,174 participants were in both high and low LDL groups? That’s statistically and biologically nonsensical.
Alzheimer’s exclusion unexplained. Those with pre-existing Alzheimer’s were removed, but with no breakdown of their LDL levels – crucial missing data.
Propensity score manipulation. This “retrospective matching” excluded over 350,000 people, distorting the natural associations. Diabetes and hyperlipidaemia were artificially balanced between groups, masking real-world relationships.
Key confounder: statin timing. Participants were only included after being prescribed statins, meaning LDL levels were already artificially lowered. So “low LDL” here is post-drug, not natural. The entire premise collapses.
This study, like too many others published today, exemplifies what Drummond Rennie famously criticised:
“There is no study too fragmented, no hypothesis too trivial, no design too warped, no analysis too self-serving for it to be published.”
So what do we actually know? Here is an extract from Patrick’s new book – Alzheimers: Prevention is the Cure.
Cholesterol and the Brain – The Real Story
Your brain needs cholesterol. Low cholesterol (<4 mmol/l) is a clear risk factor for dementia. One biomarker study found that high homocysteine and low cholesterol were the best predictors of dementia risk【1】.
And what’s a common cause of low cholesterol in the elderly? Statins. These drugs have consistently failed to show benefits in preventing cognitive decline【2】.
This fits what we know genetically. The ApoE gene governs how cholesterol gets into neurons. Those with ApoE4 are less efficient at this – that’s why they’re more prone to cognitive decline.
It’s not high cholesterol itself that’s dangerous – it’s cholesterol mismanagement in the brain.
Yes, very high cholesterol (above 6.5 mmol/l) is statistically linked to increased dementia risk – but modest elevations, particularly with a healthy lifestyle, are not a problem【3】. And even that data is shaky. One meta-analysis of over a million people showed only a 14% increased dementia risk with “high” cholesterol. But the thresholds varied – some studies defined “high” as anything over 6.2 mmol/l【3】.
More importantly, people with higher cholesterol often eat more sugar, processed foods, and trans fats – all factors known to fuel inflammation and oxidative stress in the brain.
The Lancet Commission, which makes the anti-cholesterol case, even acknowledged this diet–dementia link: in a cohort of 94,184 Danes, poor diet predicted both high LDL and dementia risk【4】.
So maybe it’s not the cholesterol – it’s what comes with it.
Statins and the Hope for Vascular Dementia
Originally, statins were hyped for vascular dementia – about 20% of all dementia cases – because of their supposed blood vessel–protective effects. But that theory has fallen flat. A Cochrane review found no benefit from statins for dementia prevention【6】.
And the best independent trial – not funded by drug companies – also found no cardiovascular benefit for statins in older adults【5】.
There’s no data supporting the notion that statins protect the brain. Yet the Lancet Commission listed “high cholesterol” as contributing 7% to dementia risk, which will no doubt spur even more statin prescriptions【4】.
The Optimum Nutrition Perspective
From an optimum nutrition standpoint, we view cholesterol differently.
If your total cholesterol is up to 6.5 mmol/l – but you have high HDL, low triglycerides, low homocysteine, and a healthy diet low in sugar and refined carbs – you’re not at risk. In fact, you’re likely protected.
One recent study showed that higher HDL in midlife predicted significantly lower future dementia risk【7】. Low HDL, not high total cholesterol, is a hallmark of metabolic syndrome – the precursor to diabetes, heart disease, and yes, dementia.
The evidence is clear: cholesterol is essential for brain health. Statins do not prevent dementia – and may contribute to cognitive decline by pushing cholesterol levels too low.
Instead of dumbing down the brain with unnecessary statins, we need to smarten up with nutrients that build brain health: omega-3 fats, phospholipids, B vitamins, and a low-sugar diet.
Doctors prescribing statins as dementia prevention are not only missing the mark – they may be making things worse.
Let’s change the narrative. Let’s put nutrition – not cholesterol fear – at the top of the brain health agenda. Find out more in Patrick’s new book – Alzheimer’s: Prevention is the Cure.
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
References
1 Gong, Q., Xie, L., Bi, M., & Yu, L. (2021). A probability formula derived from serum indicators, age, and comorbidities as an early predictor of dementia in elderly Chinese people. Brain and Behavior 11, e2236. https://doi.org/10.1002/brb3.2236
2 Peters, R, Breitner, J, James, S, et al. Dementia risk reduction, why haven’t the pharmacological risk reduction trials worked? An in-depth exploration of seven established risk factors. Alzheimer’s Dement. 2021; 7:e12202. https://doi.org/10.1002/trc2.12202
3 Wee J, Sukudom S, Bhat S, Marklund M, Peiris NJ, Hoyos CM, Patel S, Naismith SL, Dwivedi G, Misra A. The relationship between midlife dyslipidemia and lifetime incidence of dementia: A systematic review and meta-analysis of cohort studies. Alzheimers Dement (Amst). 2023 Mar 8;15(1):e12395. doi: 10.1002/dad2.12395. PMID: 36911359; PMCID: PMC9993469.
4 Kjeldsen EW, Thomassen JQ, Rasmussen KL, Nordestgaard BG, Tybjærg-Hansen A, Frikke-Schmidt R. Adherence to dietary guidelines and risk of dementia: a prospective cohort study of 94 184 individuals. Epidemiol Psychiatr Sci 2022; 31: e71.
5 Han BH, Sutin D, Williamson JD, Davis BR, Piller LB, Pervin H, Pressel SL, Blaum CS; ALLHAT Collaborative Research Group. Effect of Statin Treatment vs Usual Care on Primary Cardiovascular Prevention Among Older Adults: The ALLHAT-LLT Randomized Clinical Trial. JAMA Intern Med. 2017 Jul 1;177(7):955-965. doi: 10.1001/jamainternmed.2017.1442. PMID: 28531241; PMCID: PMC5543335.
6 McGuinness B, Craig D, Bullock R, Passmore P. Statins for the prevention of dementia. Cochrane Database Syst Rev 2016;1: CD003160.
7 Zhang X, Tong T, Chang A, Ang TFA, Tao Q, Auerbach S, Devine S, Qiu WQ, Mez J, Massaro J, Lunetta KL, Au R, Farrer LA. Midlife lipid and glucose levels are associated with Alzheimer’s disease. Alzheimers Dement. 2023 Jan;19(1):181-193. doi: 10.1002/alz.12641. Epub 2022 Mar 23. PMID: 35319157; PMCID: PMC10078665.
If you think that Alzheimer’s or dementia is caused by amyloid plaques in the brain, or tangles of nerves (neurofibrillary tangles) associated with p-tau, you have been successfully fooled. But you would not be alone. There is a vast sleight of hand going on that remarkably continues to hijack research into true causes and potential cures for Alzheimer’s, despite a mountain of clear evidence to the contrary.
Let’s start at the beginning. Some people suffer increasingly severe cognitive decline. This affects about one in ten older people. We call this dementia. Some people with dementia, on scanning their brains, have big gaps in the central part of the brain. This is used to diagnose the form of dementia known as Alzheimer’s disease, due to the clear evidence of ‘pathology’ – something wrong in the brain that amounts to the death of significant amounts of brain cells in critical areas.
So, here we have two clear diagnostic criteria. Firstly, a loss of cognitive function, which is what is tested by the dementia prevention charity, Food for the Brain, with its free, online Cognitive Function Test. Secondly, a loss of actual brain, which is diagnosed by a type of brain scan of the central or medial part of the brain. This scan was first developed based on research at Oxford University, headed by Professor David Smith, who is a member of the Scientific Advisory Board – see foodforthebrain.org/sab.
What Causes Alzheimer’s?
So, then the question is: what causes it? There has never been any evidence (and there is still no evidence), that Alzheimer’s, except for the very rare early-onset types of Alzheimer’s caused by genes, is caused by deposits of amyloid protein or amyloid plaque in the brain. “Over the past 25 years, Alzheimer’s research has suffered a litany of ostensible fraud and other misconduct by world-famous researchers and obscure scientists alike, all trying to ascend in a brutally competitive field,” claims Charles Piller in the New York Times [1], author of the book, Doctored: Fraud, Arrogance, and Tragedy in the Quest to Cure Alzheimer’s.
An example of the ‘doctoring’, reported by Dr Matthew Schrag, professor of neuroscience at Vanderbilt University, in Science in 2022, identified as many as 10 papers on the protein that deserve deeper scrutiny [2]. The report also cited other prominent researchers who have had difficulty replicating results of the studies on the specific proteins. The original research has now been withdrawn.
The reality is that about 30% of older people have plaques in their brains without dementia. About 15% of those with dementia don’t have amyloid plaques [3]. Having amyloid plaques doesn’t cause dementia. Mice whose brains have been molecularly engineered to produce amyloid plaques behave normally. Even a head full of plaques only results in mild memory problems. Many of us have plaques in our brain and remain completely healthy.
What started the amyloid excitement?
Less than 1% of diagnoses of Alzheimer’s are caused by genes. These account for very early onset cases. The genes are Amyloid Protein Precursor (APP) gene and Presenilin (PS1 and PS2). Now these rare dementias can all plausibly be assumed to be caused by amyloid plaque deposition, and to be potentially curable by its removal. However, being so rare, there is little commercial imperative to find out. There is, however, one study in 2019 that tested two different anti- amyloid treatments given to those with this rare early-onset Alzheimer’s. Despite both drugs effectively lowering the amyloid burden, there was no clinical improvement, but a slight worsening for one of these treatments compared to placebo. In addition, one in five had brain swelling [4]. That would be reason enough to give up on the amyloid hypothesis.
The big mistake, however, was the leap of faith assuming that therefore ALL Alzheimer’s, which makes up two thirds of dementias, were also caused by amyloid accumulation and could be so treated with drugs to lower the amyloid burden.
What happens if you ‘treat’ amyloid plaques?
Blocking the enzymes that make amyloid has made people worse, not better, despite lessening the amyloid burden [5]. Vaccinating animals to remove the plaques doesn’t change anything to do with dementia, but it does reduce the amyloid. The anti-amyloid vaccine injections in humans have been equally ineffective (in terms of impacting dementia), despite lowering their amyloid burden.
The pharmaceutical companies running these failed trials have pushed and pushed until they could just about get a ‘significant’ difference in the rate of degeneration of patients versus placebo on assessment questionnaires – just enough to get a medical licence despite being clinically ineffective. Lecanemab was the first to be licensed in the UK, in 2024. The difference in the lecanemab trial between those on the drug and those on placebo was equivalent to less than half a point (0.45) change on an 18 point Clinical Dementia Rating (CDR) scale [6]. According to a British Medical Journal editorial this decrease “fell well short, representing only around a third of what a minimum clinically important difference might look like.” [7]
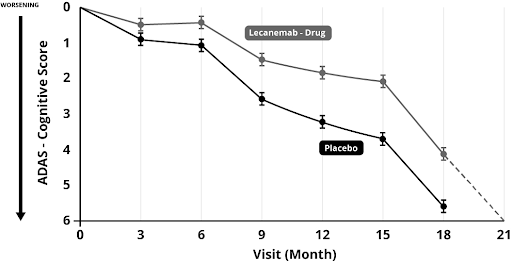
On another scale, the Alzheimer’s Disease Assessment Scale (ADAS), both those on placebo and drug treatment start to decline rapidly after 15 month (see figure 1 right). The Alzheimer’s Society [8] report this miniscule difference as ‘Lecanemab slowed down the speed at which memory and thinking skills got worse by 27%’.
Figure 1 – Worsening of ADAS cognitive score with lecanemab versus placebo
This was the figure reported in the newspapers, ignoring the fact that, in reality, those on the drug just hit the same rock bottom about 3 months later than those on the placebo and the difference is so small that no-one is likely to notice. No-one got better. They all got worse. Quite a few got adverse effects, with brain bleeding and swelling. More than a quarter had adverse reactions. A few died as a consequence. Is three months of ‘slightly less worse’ worth the suffering of one in four and the death of a few (about one in 500) at vast expense? If such treatment was started before a person was put into care, at best it could mean putting them in a care home three months later, potentially saving £3,000. If treatment were given while in a care home it would mean three months more time in a care home, potentially costing £3,000 more. Either way, at a treatment cost more likely to be in the region of £50,000 per year this is clearly not cost effective for the NHS.
But still, drug regulatory agencies, paid for by the drug industry, dished out licences because the results were ‘statistically significant’- the result of enrolling as many as 1795 people. Larger trials make small positive results look better.
Even so, the UK watchdog NICE said the evidence wasn’t good enough and recommended the National Health Service not to give anti-amyloid treatment – at about £50,000 a patient per year when you factor in the cost of scans needed to check for bleeding and swelling with each injection and medical costs. Despite this you’ll read newspaper headlines such as ‘Alzheimer’s drugs should be prescribed like statins’, as appeared in the Telegraph [9], interviewing Professor Hardy from UCL.
Please also bear in mind that even these bad results are the best that the drug company, who funded and ran their own drug trial could conjure up with questionable methodology. The CDR (Clinical Dementia Rating) is essentially a questionnaire completed by a partner/carer and clinician. If you had vested hope that your loved one might improve on an experimental drug, might you answer slightly more positively?
Also, these trials are meant to be ‘double-blind’ i.e., the patient (and carer/partner) doesn’t know if they are injected with a placebo or drug. But when almost a quarter get severe side-effects just how ‘double-blind’ is it? If you got side-effects, assumed you were on the drug, would the hope of improvement bias your answers?
The truth is it is easy to cheat in trials, or at least massage the results in your favour, and there is a strong motive to do so, if it’s your drug, job and profits at stake. That’s why I trust trials done on drugs or vitamins by independent researchers. These don’t exist for the anti- amyloid drugs and are unlikely to, due to the vast expense of such trials. Independent researcher Sarah Ackley wanted to do a meta-analysis for publication in the British Medical Journal of anti-amyloid drug trials. She identified 34 trials suitable for inclusion in her analysis, but was denied access to the data of 20.[10] In other words, a drug company can run a failed trial, ditch it and move on, only revealing those that show an effect. Out of the 14 trials she was allowed to see the data from their meta-analysis concluded: “Combined results from 14 randomized controlled trials provide evidence that reduction in amyloid levels alone is unlikely to substantially slow cognitive decline within the follow-up period of most typical trials. The results of pooled estimates suggest that use of anti-amyloid drugs is not a viable strategy for the prevention or treatment of Alzheimer’s disease and that other potential targets may merit more attention.”
Pharmacology Professor David Smith from the University of Oxford responded to the British Medical Journal[11] saying “Scientists should seriously question the validity of the basic amyloid hypothesis, as was pointed out more than 10 years ago in relation to earlier trials.[12] These findings should direct our attention to the prevention of Alzheimer’s disease by slowing down the disease process, for which there are many possible approaches. The study also raises an ethical question: is it justifiable to ask patients to undergo yet more trials of anti-amyloid treatments? Moreover, we should all question the morality of the drug companies that declined to give these researchers access to data for 20 of the 34 trials they wanted to study.”
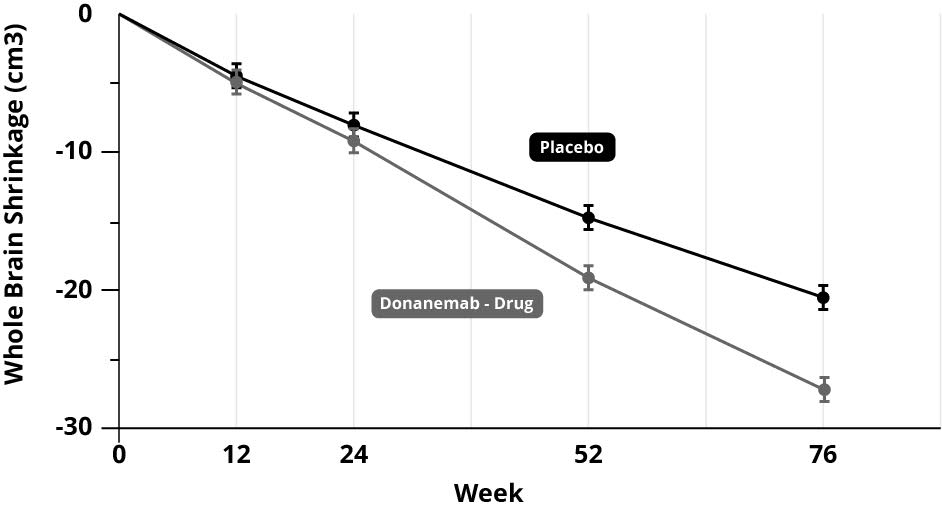
In scientific terms, the poor results of the clinical trials, despite lowering amyloid burden, added to the already existing mountain of evidence, that amyloid deposits don’t cause Alzheimer’s; lowering it doesn’t stop the disease process, doesn’t improve cognitive powers in any meaningful way and doesn’t slow down brain shrinkage. In fact, if anything, it accelerates the main physical measure of brain shrinkage. In the anti-amyloid trial for donanemab, those on the amyloid treatment had considerably more whole brain shrinkage – greater than 20% more than those on the placebo (see graph below).[13]
Figure 2 – Brain shrinkage with donanemab versus placebo
You would think that the whole field would get the message by now; stop funding this dead end and explore other avenues. But there is a lot of investment in the ‘amyloid cascade hypothesis’ that no-one wants to give up. It’s become an unhealthy obsession.
In the US, the Alzheimer’s Association and in the UK the Alzheimer’s Society and Alzheimer’s Research UK, have all supported this line of research and continue to do so. The Alzheimer’s Society, having part funded original research into amyloid with Professor Hardy, consider this their greatest contribution to the field, ‘revolutionising dementia research’.[14] The trouble is, it’s a dead end.
In 2024, there were 164 clinical trials registered assessing 127 drugs, many of which are based on amyloid and p-tau.[15] With several million ‘eligible’ patients, pharma is not going to give up.
Why aren’t other avenues being explored?
It’s partly to do with money. No-one can get research money if they’re not looking at amyloid (or p-tau – more on this in a minute).
In the UK, the Medical Research Council continues to pour good money after bad by making another £20 million available for drug trials.[16] That’s taxpayers’ money backing the wrong horse, despite a lousy track record. In the US, the National Institutes of Health and the National Institutes of Aging spend vast sums pushing in this fruitless direction. Big pharma spends twice as much as the government agencies and the charities, both of which are funded by the taxpayers, probably around $150 billion so far. So, perhaps $250 billion has been spent getting almost nowhere. Sure, we know a lot more about amyloid and p-tau, but are no closer to a ‘cure’.
I remember when, at the G8 Summit in 2013 in London, pharma- funded scientists said, Within ten years we’ll have a cure. Listening to the BBC Radio 4’s Inside Health programme on ‘What’s next for Alzheimer’s’ [17] in November last year, they said the same thing. How can you claim you’ll have a cure when you don’t even know the cause? I predict we’ll be in the same place in ten years if the Alzheimer’s industry doesn’t move on from amyloid and p-tau.
But it gets worse. Despite nothing but evidence to the contrary, based on the completely false notion that ‘Alzheimer’s IS amyloid’, we are being told an amyloid blood test is around the corner. This will tell us nothing useful. It won’t tell us who has Alzheimer’s or who is at risk. So why take the test?
The case for developing a test was made by Professor Hardy in the Telegraph. “My dream is you go the doctor at age 60, have a test, just as you would do for cholesterol. So, it finds you’re at high risk for Alzheimer’s disease, let’s put you on anti-amyloid drugs. Scientifically not difficult.” This may be his pipe dream but, as you have read, no treatment has yet shown a clinically significant effect. A Cognitive Function Test is a better (and free) predictor than an amyloid test, anti- amyloid drugs don’t work and are dangerous. Also, statins don’t work nearly as well as we were led to believe. But the two-step dance of a test that feeds a prescription to healthy people certainly made a lot of money. Over $1 trillion. Statements like this are about sales not science. At best, not that there is evidence to support this, he says that it could
mean going from diagnosis to nursing home in seven years instead of five years. In other words, no-one gets better or stays the same. They would just get worse more slowly.
All this is laid out beautifully in a book by Karl Herrup, Professor of Neurobiology and Investigator at the Alzheimer’s Disease Research Centre at the University of Pittsburgh, called How NOT to study a disease – The Story of Alzheimer’s. If you are questioning what I am saying, please read this book. You can find it in the online bookstore at foodforthebrain.org in the books section.
The medical-pharmaceutical industry is so desperate to find a treatment and make money that it just can’t give up. It reminds me of the story of Mullah Nasrudin, who was looking at the illuminated ground under a lamp post. A passer-by asked, ‘What are you looking for?’ The Mullah said, ‘I dropped a coin.’ The passer-by replied, ‘Did you drop it around here?’ The Mullah said, ‘No, but it’s the only place I can see’.
It’s akin to a campaign to ‘cure’ lemmings when the only cure is for them not to jump off the cliff in the first place. Why spend all that money researching how to give lemmings the medical attention and hospital care as they approach death, when there is a far simpler and less expensive way to help them not need it. Prevention.
A person with dementia will cost the state and family around £100,000 [18]. We can help someone substantially reduce their risk by joining Food for the Brain’s COGNITION programme with a small annual donation. So, for everyone we save from dementia, we could help thousands more.
But let’s be clear. It is true that having lots of amyloid in your brain can increase the PROBABILITY of getting Alzheimer’s in the future, in much the way that being older also increases the probability of getting Alzheimer’s. But it doesn’t cause it. So ‘curing’ amyloid won’t cure the disease.
The same thing is happening with another ‘marker’ in the brain called p-tau, which is associated with having more tangled nerves. Tau is a normal protein that becomes an abnormal, toxic protein called p-tau. The ‘p’ stands for phosphorus or ‘phosphorylated’ because there’s an enzyme that adds on the ‘p’ and another that takes it away. Much like amyloid, having more p-tau increases the PROBABILITY of Alzheimer’s, but does it cause it? Many people have raised levels of p-tau (we all have some) with no problems at all. However, unlike amyloid, there is a threshold such that if you have a lot of p-tau, which means a lot of tangled nerves, this does correlate with the degree of cognitive impairment.
By using the same sleight of hand, £10 million has been put up by the Bill Gates Foundation and people funding Alzheimer’s Research UK, to find the blood test for p-tau (I think they’ve already decided on one called p-tau 217), despite questionable evidence that p-tau causes Alzheimer’s and may just be an artefact of the disease process. In a similar way, tooth decay caused by nutrition and lifestyle deficiencies, such as too much sugar and not brushing your teeth.
No doubt, those with raised p-tau 217 will be told they have ‘pre-clinical dementia’, despite no evidence that they do. Of course, if they had a p-tau lowering drug that actually worked, as in reducing dementia risk, that might be excusable, but they don’t. Those that have blocked the enzymes that cause the accumulation of p-tau have failed. A more relevant question is what causes p-tau to go up? In other words, go to the root of the problem. However, this sleight of hand may be used to sell drugs that don’t work, much like ‘cholesterol’ has been used to sell statins.
My cholesterol is slightly high – I have no disease, no risk factors for heart disease and there is no evidence that lowering my cholesterol will lower my future risk, but still my doctor wants to prescribe me statins. Why? Because GPs are given a calculator called QRisk where you pop in age and cholesterol level and it says ‘prescribe statins’. In any case – two thirds of heart attacks are predicted by high homocysteine – not cholesterol.
P-Tau Delusion
With the failure of amyloid drugs to commercialise much emphasis is being put on p-tau inhibitor drugs. So far there are no good clinical results with several horses in the race.
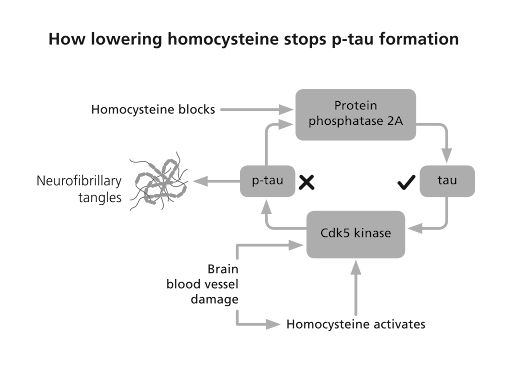
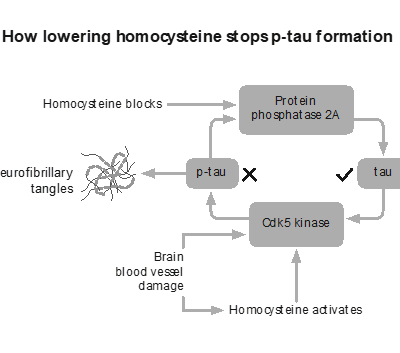
The only thing I know that does lower p-tau is lowering homocysteine with B vitamins. Homocysteine, a toxic amino acid also found in those with Alzheimer’s and dementia, promotes the enzyme that makes p-tau and blocks the enzyme that clears it from your brain [19], as the diagram overleaf shows.
However, homocysteine, unlike amyloid, is actually causal. That is, lowering homocysteine with B vitamins, stops the accelerated brain shrinkage, stops the cognitive decline and memory loss. That is consistent with a disease-modifying treatment and possibly the only thing, which from the current evidence, could be said to be causal. It is possible that some of its benefit is in lowering p-tau. There’s not enough research yet to say more than that at this point in time.
Figure 3 – How lowering homocysteine inhibits p-tau formation.
Of course, the ‘tauists’ know this and most of the drugs being developed try to do what lowering homocysteine does. Building on a few discoveries that ‘methylene blue’ [20], a methylated colouring, interfered with the formation of p-tau, and that the amino acid cysteine is involved in tau accumulation [21], drugs such as HMTM (Hydromethylthionine mesylate) exploit this bit of chemistry. Lack of B vitamins messes up methylation and homocysteine accumulates, leading to more p-tau formation. (Homocysteine is made from the amino acid methionine, which can also be turned into the amino acid cysteine, then glutathione – see Chapter 6). It is unlikely these drugs will have a substantial clinically significant effect, and much less so than lowering homocysteine. No doubt they will have adverse effects to factor in. But it won’t stop the drive to get such tau accumulation- inhibitor (TAI) drugs to market. Of course, it would be easier to just lower homocysteine with inexpensive and safe B vitamins, but these cannot be patented and hence cannot generate the profit pharma companies are looking for.
If treatment was really being driven by science, everyone would already be shouting about homocysteine lowering B vitamins (see Chapter 6). One senior representative of a pharma company told Professor David Smith, whose research on homocysteine is par excellence, that homocysteine lowering B vitamins would be a ‘multi-billion blockbuster drug if it could be patented’. But therein lies the problem
That doesn’t mean there won’t be other causes. Not everyone who develops Alzheimer’s has high homocysteine levels. There are other natural processes and compounds that can become damaging if they get out of balance. For instance, oxidants and inflammation protect against injury and infection but can damage mitochondria – the so called ‘energy’ factories inside every brain – if levels get too high. The effects of insulin resistance and damaged glucose control are similar.
Diabetes and dementia are strongly linked, the first doubling the risk of the second. [22] In truth, both homocysteine, which is a measure of a vital process called methylation, oxidation, insulin resistance and inflammation all affect the mitochondria. One clue for inflammation being involved relates to the finding that those with rheumatoid arthritis using heavy duty anti-inflammatory drugs have less risk for Alzheimer’s.[23]
These are some of the fruitful avenues that have been explored and show real promise. But they have all largely been ignored because of the unhealthy obsession by Pharma, the Alzheimer’s societies and government funding bodies on amyloid and tau. They will be explored in subsequent chapters.
In Food for the Brain’s model of dementia, glycation, oxidation, methylation and the vital role of brain fats, which actually build the brain, are central. I call them the ‘four horsemen of the mental health apocalypse’. The discovery that the homocysteine lowering B vitamins and omega-3 are co-dependent and together, dramatically slow brain shrinkage and improve cognitive function much better than any amyloid or p-tau treatment to date, is of major importance. Yet, this has been largely ignored by the blinkered Alzheimer’s establishment. So, next time you are asked to donate to Alzheimer’s charities ask them if any of the money is being spent on amyloid or p-tau. If it is, I’d suggest politely declining. If instead they are funding research into oxidation, inflammation, homocysteine, insulin or mitochondrial function, then that’s a much better sign that your money is being put to good use.
Is Alzheimer’s prevention the cure?
However, just focusing on one of these avenues may be misguided. It is based on the current paradigm of medical research – find the thing that is causing the disease, then ‘cure’ that. This assumes there is one cause and therefore one treatment. Of course, this is what you need for a drug to make money.
Let’s take homocysteine as an example. Not everyone who develops dementia or Alzheimer’s has high homocysteine. According to research at the US National Institutes of Health, it accounts for 22% of the risk.[24] Those who do have high homocysteine will reliably develop dementia and lowering it reliably reduces their cognitive decline. So, high homocysteine is a CAUSE, but not the only cause. Insulin resistance leads to diabetes and increases the risk for dementia. So, insulin resistance, driven by too much sugar and refined carbohydrates, is probably a cause, but not the only one. There isn’t enough evidence yet to declare ‘cause’, but the evidence that exists certainly points that way.
There is a different way of thinking and researching called ‘systems-based’ science. Much like the straw that breaks the camel’s back, this approach presumes there are a number of conditions, not just one, that can result in a disease such as Alzheimer’s or dementia. After all, a stroke or head injury can be a cause of cognitive decline, even if you don’t have high homocysteine or blood sugar problems. (It could be that a potential causal mechanism that ties these together is cerebrovascular dysfunction – disturbed blood supply to the brain. High homocysteine, by the way, increases risk of this by 17-fold [25]).
In my book Upgrade Your Brain, which gives all the referenced studies for statements made here, I argue that every known risk factor or biomarker for cognitive decline, dementia or Alzheimer’s affects either the structure, the function or the utilisation of the neuronal network and that it is combinations of these that crank up risk and ultimately brain pathology.
It’s like saying five critical things have to work for your car to move forward and not crash. Tyre pressure good, brakes working, enough gas, oil to lubricate the engine and water to cool it. If any one of these is completely broken, the car stops or crashes. If two are not working well, such as low oil and low water, the car grinds to a halt. If the brakes aren’t working, you crash.
We tend to think this way in nutrition and lifestyle medicine. It’s the combination of insults such as high sugar intake, too many fried foods, lack of vegetables, too much alcohol and smoking, that breaks the camel’s back. That heart attack is the ‘perfect storm’ of several underlying factors.
This systems-based approach isn’t popular in science and very few funders ever put up money to fund this kind of research. Usually, a funder wants to fund one stream of research, possibly a clinical trial of one approach, in the belief that this one factor is the key and a great discovery will be made. The reality is that it is usually combinations of factors that drive risk, with the manifestation of the disease itself being the ‘broken back’. Pollution, for example, is a risk factor for dementia … but not in those with good vitamin B6, folate or B12 status [26], which are the three B vitamins needed for methylation, indicated by lower homocysteine. Methylation is a major mechanism in the body, used to detoxify pollutants and toxins.
This is where Food for the Brain’s approach is unique. By collecting data from people like you who have both taken the Cognitive Function Test and completed the COGNITION questionnaire, and keep doing so, we can look at what drives cognitive function up and down. In other words, what ‘breaks the camel’s back’ or alternatively, makes it ‘strong’. This kind of complex systems-based science has become possible due to big data gathering (such as we are doing), advances in complex statistics, computer power and programming AI algorithms. Our Head of Science, Associate Professor Tommy Wood, is an expert in this kind of approach to neuroscience.
It is, I believe, the future and why we will probably find no single primary cause for Alzheimer’s, and certainly not amyloid or p-tau, but combinations of diet and lifestyle and other factors that create the tipping point that leads to dementia. Then, we will have the means to prevent this tipping point from ever being reached. In other words, we may discover that prevention is the cure.
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
3. Herrup K. The case for rejecting the amyloid cascade hypothesis. Nat Neurosci. 2015 Jun;18(6):794–799. doi: https://doi.org/10.1038/nn.4017 (Also see references and full discussion in Chapter 8 of How Not to Study a Disease, K. Herrup, MIT Press. Lopez OL, et al. Association Between β-Amyloid Accumulation and Incident Dementia in Individuals 80 Years or Older Without Dementia. Neurology. 2024 Jan 23;102(2):e207920.)
4. Salloway S, et al. Dominantly Inherited Alzheimer Network–Trials Unit. A trial of gantenerumab or solanezumab in dominantly inherited Alzheimer’s disease. Nat Med. 2021 Jul;27(7):1187–1196. doi: https://doi.org/10.1038/s41591-021-01369-8 Epub 2021 Jun 21.
5. Volloch V, et al. Results of Beta Secretase-Inhibitor Clinical Trials Support Amyloid Precursor Protein-Independent Generation of Beta Amyloid in Sporadic Alzheimer’s Disease. Med Sci (Basel). 2018 Jun 2;6(2):45. doi: https://doi.org/10.3390/medsci6020045
6. van Dyck CH, et al. Lecanemab in Early Alzheimer’s Disease. N Engl J Med. 2023 Jan 5;388(1):9–21. doi: https://doi.org/10.1056/NEJMoa2212948 Epub 2022 Nov 29.
15. Ackley SF, et al. Effect of reductions in amyloid levels on cognitive change in randomized trials: instrumental variable meta-analysis. BMJ. 2021 Feb 25;372:n156. doi: https://doi.org/10.1136/bmj.n156 Erratum in: BMJ. 2022 Aug 30;378:o2094.
10. Smith AD. Anti-amyloid trials raise scientific and ethical questions. BMJ. 2021;372:n805. doi: https://doi.org/10.1136/bmj.n805
12. Sims JR, et al. Donanemab in Early Symptomatic Alzheimer Disease: The TRAILBLAZER-ALZ 2 Randomized Clinical Trial. JAMA. 2023 Aug 8;330(6):512–527. doi: https://doi.org/10.1001/jama.2023.13239
19. Smith AD, Refsum H. Homocysteine, B Vitamins, and Cognitive Impairment. Annu Rev Nutr. 2016 Jul 17;36:211–239. doi: https://doi.org/10.1146/annurev-nutr-071715-050947; see also Li JG, Chu J, Barrero C, Merali S, Pratico D. Homocysteine exacerbates β-amyloid, tau pathology, and cognitive deficit in a mouse model of Alzheimer’s disease with plaques and tangles. Ann Neurol. 2014;75:851–63; doi: https://doi.org/10.1002/ana.24166; see also Shirafuji N, et al. Homocysteine Increases Tau Phosphorylation, Truncation and Oligomerization. Int J Mol Sci.2018 Mar 17;19(3):891. doi: https://doi.org/10.3390/ijms19030891; see also Bossenmeyer-Pourié C, et al. N-homocysteinylation of tau and MAP1 is increased in autopsy specimens of Alzheimer’s disease and vascular dementia. J Pathol. 2019 Jul;248(3):291–303. doi: https://doi.org/10.1002/path.5254 Epub 2019 Mar 19.
20. Wischik CM, et al. Selective inhibition of Alzheimer disease-like tau aggregation by phenothiazines. Proc Natl Acad Sci U S A. 1996 Oct 1;93(20):11213–8. doi: https://doi.org/10.1073/pnas.93.20.1121
21. Al-Hilaly YK, et al. Cysteine-Independent Inhibition of Alzheimer’s Disease-like Paired Helical Filament Assembly by Leuco-Methylthioninium (LMT). J Mol Biol. 2018 Oct 19;430(21):4119–4131. Epub 2018 Aug 16. Doi: https://doi.org/10.1016/j.jmb.2018.08.010
22. Arvanitakis Z, et al. Diabetes mellitus and risk of Alzheimer disease and decline in cognitive function. Arch Neurol.2004 May;61(5):661–666. doi: https://doi.org/10.1001/archneur.61.5.661; see also Yaffe K, et al. Diabetes, impaired fasting glucose, and development of cognitive impairment in older women. Neurology. 2004 Aug 24;63(4):658–663. doi: https://doi.org/10.1212/01.WNL.0000134665.93885.71; see also Tiehuis AM, et al. Diabetes Increases Atrophy and Vascular Lesions on Brain MRI in Patients With Symptomatic Arterial Disease. Stroke. 2008 May;39(5):1600–1603. doi: https://doi.org/10.1161/STROKEAHA.107.502963; see also Samaras K, et al. The impact of glucose disorders on cognition and brain volumes in the elderly: the Sydney Memory and Ageing Study. AGE. 2014;36(2):977–993. doi: https://doi.org/10.1007/s11357-013-9585-3; see also Mortby ME, et al. High ‘normal’ blood glucose is associated with decreased brain volume and cognitive performance in the 60s: the PATH through life study. PLoS One. 2013 Sep 4;8(9):e73697. doi: https://doi.org/10.1371/journal.pone.0073697; see also Crane PK, et al. Glucose levels and risk of dementia. N Engl J Med. 2013 Aug 8;369(6):540–548. doi: https://doi.org/10.1056/NEJMoa1215740; see also Luchsinger JA, et al. Hyperinsulinemia and risk of Alzheimer disease. Neurology. 2004 Oct 12;63(7):1187–1192. doi: https://doi.org/10.1212/01.wnl.0000140292.04932.87; see also Abbatecola AM, et al. Insulin resistance and executive dysfunction in older persons. J Am Geriatr Soc. 2004 Oct;52(10):1713–1718. doi: https://doi.org/10.1111/j.1532-5415.2004.52466.x; see also Ye X, et al. Habitual sugar intake and cognitive function among middle-aged and older Puerto Ricans without diabetes. Br J Nutr. 2011 Nov;106(9):1423–1432. doi: https://doi.org/10.1017/S0007114511001760; see also Power SE, et al. Dietary glycaemic load associated with cognitive performance in elderly subjects. Eur J Nutr.2015 Jun;54(4):557–568. doi: https://doi.org/10.1007/s00394-014-0737-5; see also Seetharaman S, et al. Blood glucose, diet-based glycemic load and cognitive aging among dementia-free older adults. J Gerontol A Biol Sci Med Sci. 2015 Apr;70(4):471–479. doi: https://doi.org/10.1093/gerona/glu135; see also Taylor MK, et al. A high-glycemic diet is associated with cerebral amyloid burden in cognitively normal older adults. Am J Clin Nutr. 2017 Dec;106(6):1463–1470. doi: https://doi.org/10.3945/ajcn.117.162263; see also Gentreau M, et al. High Glycemic Load Is Associated with Cognitive Decline in Apolipoprotein E ε4 Allele Carriers. Nutrients. 2020 Nov 25;12(12):3619. doi: https://doi.org/10.3390/nu12123619
23. Xie W, et al. Association between disease-modifying antirheumatic drugs for rheumatoid arthritis and risk of incident dementia: a systematic review and meta-analysis. RMD Open. 2024 Feb 27;10(1):e004016. doi: https://doi.org/10.1136/rmdopen-2023-004016
24. Beydoun MA, et al. Epidemiologic studies of modifiable factors associated with cognition and dementia: systematic review and meta-analysis. BMC Public Health. 2014 Jun 24;14:643. doi: https://doi.org/10.1186/1471-2458-14-643
25. Teng Z, et al. Cerebral small vessel disease mediates the association between homocysteine and cognitive function. Front Aging Neurosci. 2022;14:868777. doi: https://doi.org/10.3389/fnagi.2022.868777
26. Chen C, et al. B vitamin intakes modify the association between particulate air pollutants and incidence of all-cause dementia: Findings from the Women’s Health Initiative Memory Study. Alzheimers Dement. 2022 Nov;18(11):2188–2198. doi: https://doi.org/10.1002/alz.12515 Epub 2022 Feb 1.
Something concerning is happening to our children – an increasing number are experiencing psychological and behavioural challenges, often diagnosed as autism.
These challenges range from reduced eye contact and language delays to social difficulties, cognitive struggles, emotional meltdowns, aggression, and in some cases, depression. But what is driving this surge?
—
Is it down to genetics & better diagnosis?
While mainstream medicine largely attributes autism to genetics, explaining the rise as improved diagnostic recognition, a growing body of independent researchers and clinicians in the US and UK suggests otherwise. The rapid increase in cases across multiple countries cannot be solely explained by genetics, as genes do not change so quickly. In the US, autism rates have skyrocketed from 2 in 10,000 to 1 in 36 over 50 years. In the UK, official government data estimates 1 in 62 children are classified as autistic; an eightfold increase in 20 years. Meanwhile, school census data from Scotland and Northern Ireland report even higher rates, with 1 in 20 children diagnosed. These numbers strongly indicate that environmental factors, including diet, play a key role. This also suggests that proactive steps could help reduce risk.
That is why we are launching COGNITION for Smart Kids &Teens in April with the online ‘Smart Kids’ conference. We are bringing together leading experts to examine ways to prevent and potentially mitigate the impact of autism through environmental and nutritional interventions. In addition, we also have our ‘Optimising Neurodivergence public webinar for parents, caregivers or any non-practitioners who want to learn how to support our children to reach their full potential.
—
New Approaches Show Encouraging Results
Dr. Chris D’Adamo, Assistant Professor at the University of Maryland School of Medicine and Director of the Centre for Integrative Medicine, has been at the forefront of research into environmental influences on autism. His recent paper, published in Personalized Medicine, estimates a 300% rise in autism cases since 2000. The study also documents a case where early intervention reversed autism symptoms by addressing modifiable lifestyle and environmental factors.
The case involved twin toddler girls exhibiting classic autistic traits;limited communication, repetitive behaviours, resistance to change and severe gastrointestinal issues. Under a comprehensive programme, led by a team of physicians, they implemented tailored interventions focused on diet, environment and lifestyle. The results were striking; within months, both girls showed dramatic improvements. Their autism severity scores dropped significantly, with one twin’s score reducing from 76 to 32 and the other from 43 to just 4. (Read more on this case here)
In the UK, Dr. Lorene Amet, a functional nutritionist and founder of The Lauriston Centre, has been applying similar integrative approaches. She has worked with hundreds of families, with remarkable success. A survey conducted with the charity Thinking Autism, assessed 220 children who followed her recommendations. 169 families reported either ‘life-changing’ or ‘very beneficial’ improvements, while only 11 children saw no noticeable change.
Yet, despite such promising results, the NHS maintains that autism has no cure and advises against interventions such as vitamins, minerals, and dietary modifications. The NICE guidelines currently offer no targeted nutritional strategies for autism management, leaving many parents with limited options.
—
Can Autism Risk Be Reduced Before Birth?
Another key topic at theSmart Kids Conference is prevention; reducing the likelihood of autism before birth. Research led by Associate Professor Michelle Murphy of the Universitat Rovira I Virgili in Spain, has revealed a crucial link between B vitamin deficiencies in early pregnancy and a child’s likelihood of developing autism-related traits. Her studies show that children of mothers who were low in B vitamins before conception were significantly more likely to display withdrawn behaviour, anxiety, depression or aggression by age six.
The connection between maternal nutrition and neurological development is well established. For decades, pregnant women have been advised to take folic acid to prevent neural tube defects; a policy delayed by 25 years, resulting in hundreds of thousands of avoidable birth defects. Children with autism are six times more likely to have neural tube defects, further linking B vitamin deficiencies to neurodevelopmental issues.
This aligns with earlier research from Oxford University’s Professor David Smith, one of our scientific advisors. His work demonstrated that B vitamins lower homocysteine, a toxic amino acid linked to autism, depression, cognitive impairments in children and Alzheimer’s in adults. Professor Murphy’s research further suggests that even mildly elevated homocysteine levels before pregnancy strongly predict neurodivergent traits in children. This underscores the importance of nutritional screening and intervention before conception.
—
There Is So Much That Parents Can Do…
We are inviting parents to take part in a free online assessment of their child’s cognitive, emotional, and behavioural function, alongside a diet and lifestyle questionnaire to help optimise brain health. Parents can also access a home test kit for homocysteine levels, providing valuable insight into potential nutritional deficiencies that may affect brain function.
The Smart Kids conference will provide further guidance on evidence-based interventions, bringing together researchers, clinicians, and parents seeking practical solutions to support children’s cognitive development.
—
“People come in assorted shapes and sizes, with brains that are unique,” says Dr Rona Tutt, OBE, a trustee of Food for the Brain and past President of the National Association of Head Teachers. “A significant minority who are neurodivergent need to be recognised, valued, and supported to maximise their strengths and overcome challenges. Understanding the factors driving the rise in neurodivergence is key to ensuring the best outcomes for future generations.”
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
2 https://researchbriefings.files.parliament.uk/documents/POST-PN-0612/POST-PN-0612.pdf; see also Russell G, Stapley S, Newlove-Delgado T, Salmon A, White R, Warren F, Pearson A, Ford T. Time trends in autism diagnosis over 20 years: a UK population-based cohort study. J Child Psychol Psychiatry. 2022 Jun;63(6):674-682. doi: 10.1111/jcpp.13505
5 D’Adamo C et al., Reversal of Autism Symptoms among Dizygotic Twins through a Personalized Lifestyle and Environmental Modification Approach: A Case Report and Review of the Literature. J Pers Med. 2024 Jun 15;14(6):641. doi: 10.3390/jpm14060641
6 Survey conducted in collaboration with the charity Thinking Autism. The full survey results will be shown at the Smart Kids conference, April 24th 20025.
9 Roigé-Castellví J, Murphy M, Fernández-Ballart J, Canals J. Moderately elevated preconception fasting plasma total homocysteine is a risk factor for psychological problems in childhood. Public Health Nutr. 2019 Jun;22(9):1615-1623. doi: 10.1017/S1368980018003610; see also Murphy MM, Fernandez-Ballart JD, Molloy AM, Canals J. Moderately elevated maternal homocysteine at preconception is inversely associated with cognitive performance in children 4 months and 6 years after birth. Matern Child Nutr 2017;13,e12289 . doi: 10.1111/mcn.12289
10 Hasler M, Fideli ÜS, Susi A, Hisle-Gorman E. Examining the relationship between autism spectrum disorder and neural tube defects. Congenit Anom (Kyoto). 2023 Jul;63(4):100-108. doi: 10.1111/cga.12516. Epub 2023 Apr 18. PMID: 37073427.11 Smith AD, Refsum H. Homocysteine – from disease biomarker to disease prevention. J Intern Med. 2021 Oct;290(4):826-854. doi: 10.1111/joim.13279
A landmark study from the Centre for Healthy Brain Ageing (CHeBA) at the University of New South Wales (Sydney, Australia) has provided compelling evidence that targeted diet and lifestyle changes can improve cognitive function in older adults.
Or put simply, what we teach and promote at Food for the Brain works when it comes to promoting brain health.
Raising awareness and providing tools to support the critical role of diet and lifestyle in long-term cognitive health is both essential and part of the solution.
This recent study affirms our approach: sustained step-by-step adjustments to diet, exercise, sleep, and social engagement significantly reduces the risk of dementia as well as maintaining – and even enhancing – cognitive function.
—
Study shows a holistic approach to brain health works
The CHeBA study recruited over 6000 adults aged 55 to 77, dividing them into two groups, one participating in an online lifestyle intervention programme and the other serving as a control group.
Physical activity (strength and balance training),
Brain training (three weekly cognitive training sessions),
Mediterranean diet (rich in plant foods and healthy fats with limited meat and dairy),
Mental well-being (a digital anxiety and depression reduction program).
While both groups showed some cognitive improvements, those in the intervention group experienced significantly greater gains, demonstrating the added value of a structured, multi-domain approach.
Professor Brodaty, one of the study’s research team, stated:
“Participants aged 55-65 showed greater improvement than those aged 66-77, suggesting that prevention programmes should start earlier.”
—
Why a Multi-Domain Approach Works!
Unlike traditional approaches that focus on just one or two factors, the COGNITION® Programme, which you get access to when you become a FRIEND of Food for the Brain, is similarly built on eight interwoven pillars—including diet, physical exercise, sleep, social involvement, and even the gut microbiome—to provide a comprehensive brain health plan.
The study’s ‘Maintain Your Brain’ trial further supports this, showing that targeting multiple lifestyle domains simultaneously – including physical activity, nutrition, brain training, and mental well-being – leads to greater cognitive benefits, rather than focusing on a single risk factor.
And, as we always say, the earlier you start, the better!
—
Your Roadmap to the 8 Pillars of Cognitive Health
In line with this study, we focus on 8 key domains that influence brain health. These areas provide strategies to help individuals reduce their risk of cognitive decline and support long-term brain health:
Domain 1: Low Glycemic Load (GL) Diet – Managing blood sugar levels is crucial for brain function. High-sugar diets contribute to inflammation and insulin resistance, impairing cognitive performance. A low-GL diet helps stabilise energy levels and protects brain cells from damage
Domain 2: B Vitamins & Homocysteine Levels – High homocysteine levels, a by-product of metabolism, are linked to cognitive decline. Ensuring adequate B vitamins (B6, B12, and folate) supports brain function and lowers homocysteine levels.
Domain 3: Brain-Boosting Fats – Healthy fats like omega-3s (found in fish, flaxseeds, and walnuts) are essential for brain cell structure and function. They help reduce inflammation, enhance memory, and support cognition.
Domain 4: Antioxidants & Polyphenols – Free radicals damage brain cells, but antioxidants (from colourful fruits, vegetables, green tea, and dark chocolate) help combat oxidative stress and keep your brain young.
Domain 5: Healthy Gut & Microbiome – The gut-brain connection is vital for mental clarity and mood. A diverse microbiome (supported by fibre-rich foods, fermented foods, and probiotics) can reduce inflammation and improve neurotransmitter function, supporting memory and mental health.
Domain 6: Active Body (Exercise & Movement) – Regular physical activity boosts blood flow to the brain, supports neuroplasticity, and reduces the risk of dementia. Both aerobic exercise (like walking and cycling) and strength training play a role in maintaining cognitive health.
Domain 7: Active Mind – The brain thrives on challenge! Lifelong learning, problem-solving activities, and hobbies stimulate new neural connections and help build cognitive resilience.
Domain 8: Sleep & Stress Resilience Management – Poor sleep and chronic stress are major contributors to cognitive decline. Deep, restorative sleep allows the brain to clear toxins, while mindfulness, relaxation techniques, and breathing exercises help reduce stress hormones that damage brain cells.
__
We know that these 8 domains can help you protect your brain and prevent cognitive decline – but most of us need support, accountability, motivation and structure to be able to implement the necessary changes consistently.
That is why the COGNITION® Programme exists.
It’s designed to make implementing the above easier and simpler, one step at a time. By providing tailored advice and guidance on all eight areas, the programme offers tangible, practical steps that members can take to enhance brain function, reduce dementia risk, and improve overall cognitive well-being.
—
Real-Life Results…
As a research charity with a stellar scientific advisory board, we care about excellent research being carried out.
Yet the most important thing is that ‘the science’ helps to transform lives, families and communities. Citizen science in action!
Here is what can happen when you join COGNITION. One participant told us:
“I have taken the CFT for at least seven years now and find it very worthwhile. By monitoring sensibly what I eat, as you advise and exercising within my limitations, I have found that despite being 84, my results have improved.”
This experience is echoed by another participant who found benefit in making small, sustainable lifestyle changes every day:
“I’ve taken on board your recommendations and I’ve increased my vitamin B intake and started doing puzzle books every day to keep my brain active in different ways from before. I also do more exercise and yoga daily. I love the fact that I can make these small changes myself and hopefully reduce my chances of getting dementia.”
Another participant shared how working with Food for the Brain and starting with the COGNITION® Programme was a wake-up call that led to lasting changes:
“Since starting with Food for the Brain, I’ve completely reshaped my lifestyle. I now attend a weekly Pilates class, work on my allotment, swim regularly, and take longer evening walks. I’ve also cut down on alcohol and meat, increased my vitamin B intake, and started doing daily puzzles to challenge my brain in new ways. My sleep has improved and I feel more energetic with fewer foggy days.”
These testimonials show how small, targeted lifestyle changes can significantly enhance cognitive resilience and well-being. The COGNITION® Programme equips individuals with the necessary tools to take charge of their brain health, which leads to improved cognitive test scores, better mental clarity, and a greater sense of control over their future.
—
Join the COGNITION® Programme today!
As a non-profit charity we aim to make resources affordable and accessible to all, while covering essential staff and research costs. Membership of the 8-domain COGNITION® Programme is just £50 per year or £5 per month, ensuring that everyone can benefit from the programme.
You get access to the programme when you become a FRIEND of Food for the Brain.
Members receive:
Guidance on which domains to target based on their test results.
Ongoing cognitive assessments to track progress.
Access to expert-backed articles for long-term brain health.
Access to regular group coaching and Q&A sessions.
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
By Patrick Holford, in response to the New York Times essay here.
Recently, investigator Charles Piller exposed the fraudulent claims behind the amyloid theory of Alzheimer’s, that has caused heads to roll.
The article, based on his new book Doctored: Fraud, Arrogance, and Tragedy in the Quest to Cure Alzheimer’s, presents evidence of fraud. It reveals that Dr Masliah, the Head of the National Institute on Ageing (a division of the US National Institutes of Health) and responsible for billions in funding, had for decades included improperly manipulated images of brain tissue and other technical visuals in his research.
With roughly 800 papers to his name, many of them considered highly influential, Dr. Masliah seemed a natural choice to steer the funding for Alzheimer’s research. He hailed the moment as the dawning of “the golden era of Alzheimer’s disease research”. The National Institutes of Health announced that it had found that Dr. Masliah engaged in research misconduct and that he no longer held his leadership position.
Marc Tessier-Lavigne, the former president of Stanford University, was known as a global leader in research on the brain’s circuitry in Alzheimer’s and other neurological conditions. He resigned in 2023 after an intrepid student journalist revealed numerous altered images in the research of his lab, in papers he co-authored. A Stanford University investigation, however, didn’t find evidence to conclude that he personally engaged in research misconduct. They did note that at various times when concerns with his papers emerged— between 2001 and 2021—Dr. Tessier-Lavigne failed to decisively and forthrightly correct mistakes in the scientific record.
__
Amyloid exaggerations
What isn’t being fully exposed, is just how bad the results of the anti-amyloid drug treatments are and how the drug companies who run these trials manage to squeeze a result, just enough to get a medical licence for their treatment. Everyone is aware of this exaggeration by bigging up the results.
For example, the Alzheimer’s Society described the miniscule difference in effect of the anti-amyloid drug as follows: ‘Lecanemab slowed down the speed at which memory and thinking skills got worse by 27%’.
This is economical with the truth.
The British Medical Journal Editorial on the trial, in relation to a clinically meaningful effect, said it ‘fell well short, representing only around a third of what a minimum clinically important difference might look like’. Those on the drug just hit the same rock bottom about 3 months later than those on the placebo and the difference was so small that no-one is likely to notice.
No-one got better. They all got worse. Quite a few had adverse effects, with brain bleeding and swelling. More than a quarter had adverse reactions. A few died as a consequence.
Is three months of ‘slightly less worse’ symptoms worth the suffering of adverse events by one in four participants including death (about one in 500) – and all this at vast expense?
__
Expensive, ineffective and rejected by NICE
If such treatment was started before a person was put into care, at best it could mean putting them in a care home three months later, potentially saving £3,000. If treatment were given whilst in a care home it would mean three months more time in a care home, potentially costing £3,000 more. Either way, at a treatment cost likely to be in the region of £50,000 per year this is clearly not cost effective for the NHS, which is why the National Institute for Health and Care Excellence (NICE) quite rightly rejected it.
The greatest missed opportunity is that we already know how to reduce Alzheimer’s risk – through targeted diet, lifestyle and nutrient optimisation – yet far less funding and attention goes toward implementing these strategies at scale.
The power is in your hands and it’s never too late or too early to start.
Prevention is key and you can start today – so please encourage everyone you know to take the Cognitive Function test here.
Get personalised data on your body and join our research by ordering your DRIfT 5 in 1 test here so you can join our research and find out what your unique body needs.
Become a Friend & join the COGNITION Programme: Support our mission with a small monthly donation and receive tailored steps to improve your brain resilience and track your progress.
–
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
If you think that Alzheimer’s or dementia is caused by amyloid plaques in the brain, or tangles of nerves (called neurofibrilliary tangles) associated with p-tau, you have been successfully conned.
But you would not be alone.
There is a vast sleight of hand going on that remarkably continues to hijack research into true causes and potential cures for Alzheimer’s despite a mountain of evidence to the contrary.
How did this all start…
Let’s start at the beginning. Some people get increasingly severe cognitive decline. This affects about one in ten older people. We call this dementia. Some people with dementia, on scanning their brains, have big gaps in the central part of the brain, which is used to diagnose that dementia as Alzheimer’s disease due to the clear evidence of ‘pathology’ – something wrong in the brain that amounts to death of significant amounts of brain cells in critical areas. So, here we have two clear diagnostic criteria: Firstly, a loss of cognitive function which is what we test at foodforthebrain.org with our Cognitive Function test. Secondly, a loss of actual brain, which is diagnosed by a type of brain scan of the central or medial part of the brain which was first developed by the team at Oxford University, headed by Professor David Smith, a member of our Scientific Advisory Board.
—
What causes Alzheimer’s?
So, then the question is what causes it? There is no evidence, that it is caused by deposits of amyloid protein or amyloid plaque, in the brain. About 30% of older people have plaques in their brains without dementia. About 15% of those with dementia don’t have amyloid plaques. Having amyloid plaques doesn’t cause dementia. Mice with amyloid plaques behave normally. Even a head full of plaques only results in mild memory problems. Many of us have plaques in our brain and remain completely healthy.
What happens if you ‘treat’ amyloid plaques? Blocking the enzymes that make amyloid have made people worse, not better, despite lessening the amyloid burden. Vaccinating animals to remove the plaques doesn’t change anything to do with dementia, but it does reduce the amyloid. The anti-amyloid vaccine injections in humans have been equally ineffective despite lowering the amyloid burden in the brains of those injected.
The pharmaceutical companies running these failed trials have pushed and pushed until they could just about get a significant difference in the rate of degeneration of patients versus placebo on questionnaires equivalent to less than half a point change on an 18 point scale. No-one got better. Quite a few got worse, with brain bleeding and swelling. A few died as a consequence. But still drug agencies, paid for by the drug industry, dished out licences. In the UK the watchdog NICE said the evidence wasn’t good enough and recommended the National Health Service not to give anti-amyloid treatment – at about £50,000 a patient per year.
In scientific terms the trials added evidence to the mountain already existing that amyloid deposits don’t cause Alzheimer’s because lowering it doesn’t stop the disease process, doesn’t improve cognitive powers in any meaningful way and doesn’t slow down brain shrinkage. In fact, if anything, it accelerates the main physical measure of brain shrinkage. In the last anti-amyloid trial, donanemab, those on the amyloid treatment had considerably more brain shrinkage than those on the placebo.
—
The unhealthy obsession
You would think that the whole field would get the message by now, stop funding this dead end and explore other avenues. But they were so hoping and invested in the ‘amyloid cascade hypothesis’ that no-one could give up. It’s become an unhealthy obsession.
In the US the Alzheimer’s Association and in the UK the Alzheimer’s Society supported this line of thinking and continue to do so. ‘We are most proud of our contribution to amyloid’, declares the research director of the Alzheimer’s Society.
Why don’t they explore other avenues? It’s partly to do with money. No-one can get research money if they’re not looking at amyloid (or p-tau – more on this in a minute.)
In the UK the Medical Research Council continue to pour good money after bad by making another £20 million available for drug trials. That’s taxpayer’s money backing the wrong horse despite a lousy track record. In the US the National Institutes of Health and the National Institutes of Aging spend vast sums pushing in this fruitless direction. Big pharma spend twice as much as the charities, funded by us taxpayers – probably around $150 billion so far. So, perhaps $250 billion has been spent getting almost nowhere. Sure, we know a lot more about amyloid and tau but are no closer to a ‘cure’.
—
Can you claim to find a cure when you don’t know the cause?
Getting the James Webb telescope into space cost $8 billion. Here we are having spent considerably more than thirty times this and we haven’t even got lift off. I remember when, at the G8 Summit in London in 2013 pharma-funded scientists said ‘within ten years we’ll have a cure. This month, listening to the BBC Radio 4’s ‘Inside Health’ programme on Alzheimer’s, they said exactly the same thing – that magical ten years from now. How can you claim you’ll have a cure when you don’t even know the cause? I predict we’ll be in the same place in ten years if the Alzheimer’s industry don’t quit on amyloid and p-tau.
But it gets worse than this. Despite nothing but evidence to the contrary, based on the completely false notion that ‘Alzheimer’s IS amyloid’ we are being told an amyloid blood test is around the corner. In other words, if you have amyloid blood test but feel completely normal, you’ll likely be told you have ‘pre-clinical Alzheimer’s’ just waiting to happen despite a third of those with amyloid plaques having no problem at all! That’s a conflation upon a conflation.
All this is laid out beautifully in a book by Karl Herrup – Professor of Neurobiology and Investigator at the Alzheimer’s Disease Research Centre at the University of Pittsburg, called How NOT to study a disease – The Story of Alzheimer’s. If you don’t believe what I’m saying, or rightly question it, please read this book. You can find it in our online Bookstore here.
But, so desperate is the medical-pharmaceutical industry to find a treatment and make money that it just can’t give up. It reminds me of the story of Mullah Nasrudin, who is looking at the illuminated ground under a lamp-post. A passer by says ‘what are you looking for?’ The Mullah says ‘I dropped a coin.’ The person says ‘did you drop it around here?’ The Mullah said ‘no, but it’s the only place I can see’.
—
Amyloid does increase the PROBABILITY of getting Alzheimer’s in the future but it doesn’t cause it.
But let’s be clear. This doesn’t mean that having lots of amyloid in your brain doesn’t increase the PROBABILITY of getting Alzheimer’s in the future in much the way that being older also increases the probability of getting Alzheimer’s. But it doesn’t cause it. So ‘curing’ amyloid won’t cure the disease. If you ‘exist for a cure’, as one charity claims, you have a start with a clue as to what’s causing it. Obviously not amyloid.
The same thing is happening with another ‘marker’ in the brain called p-tau, which is associated with having more tangled nerves. Tau is a normal protein that becomes an abnormal, toxic protein called p-tau. The ‘p’ stands for phosphorus or ‘phosphorylated’ because there’s an enzyme that adds on the ‘p’ and another that takes it away. Much like amyloid, having more p-tau increases the PROBABILITY of Alzheimer’s but doesn’t cause it. Many people have raised levels of p-tau (we all have some) with no problems at all.
But, by using the same sleight of hand, £10 million has been put up by the Bill Gates Foundation and people funding Alzheimer’s Research UK, to find the blood test for p-tau (I think they’ve already decided on one called p-tau 217) despite no evidence that p-tau CAUSES Alzheimer’s. No doubt, those with raised p-tau 217 will be told they have ‘pre-clinical dementia’ despite no evidence that they do. Of course, if they had a p-tau lowering drug that actually worked as in reducing dementia risk, that might be excusable but they don’t. However, this sleight of hand may be used to sell drugs that don’t work much like ‘cholesterol’ has been used to sell statins.
My cholesterol is slightly high – I have no disease, no risk factors for heart disease, and there is no evidence that lowering my cholesterol will lower my future risk, but still my doctor wants to prescribe me statins. In any case – two thirds of heart attacks in older people are predicted by high homocysteine – not cholesterol.
The only thing I know that does lower p-tau is lowering homocysteine with B vitamins. Homocysteine, a toxic amino acid also found in those with Alzheimer’s and dementia, promote the enzyme that makes p-tau and blocks the enzyme that clears it from your brain as the diagram below shows.
However, talking of homocysteine, it, unlike amyloid and p-tau, is actually causal. That is, lowering homocysteine with B vitamins, stops the accelerated brain shrinkage, stops the cognitive decline and memory loss. That is consistent with a disease-modifying treatment and possibly the only thing for which the evidence could be said to be causal at this point in time.
That doesn’t mean there won’t be other causes. There are some fruitful avenues that have been explored and show real promise. But they have all largely been ignored because of the unhealthy obsession by pharma, the Alzheimer’s societies and government funding bodies on amyloid and tau. These include oxidation – and the role of antioxidants; inflammation; insulin resistance and glucose control; mitochondrial dysfunction – those are the so-called ‘energy’ factories inside every brain cell. Diabetes and dementia are strongly linked, the first often predicting the second. In truth, both homocysteine, which is a measure of a vital process called methylation, oxidation, insulin resistance and inflammation all affect the mitochondria. One clue for inflammation being involved relates to the finding that those with rheumatoid arthritis using heavy duty anti-inflammatory drugs having less risk for Alzheimer’s. In our model of dementia at Food for the Brain glycation, oxidation, methylation and also the vital role of brain fats which actually build the brain are central. I call them the ‘four horsemen of the mental health apocalypse’. The discovery that the homocysteine lowering B vitamins and omega-3 are co-dependent and, together, dramatically slow brain shrinkage and improve cognitive function light years ahead of ANY amyloid or p-tau treatment to date, is of major importance. Yet, this has been largely ignored by the blinkered Alzheimer’s establishment.
So, next time you are asked to donate to Alzheimer’s charities ask them if any of the money is being spent on amyloid or p-tau. If so, I’d suggest politely declining. If instead they are funding research into oxidation, inflammation, homocysteine, insulin or mitochondrial function, then that’s a much better sign your money might not go down a black hole.
—
Is Alzheimer’s prevention the cure?
But even just focusing on one of these avenues may be misguided. It is based on the current paradigm of medical research – find the thing that is causing the disease then ‘cure’ that. This assumes there is one cause and therefore one treatment. Of course, this is what you need for a drug to make money.
Let’s take homocysteine as an example. Not everyone who develops dementia or Alzheimer’s has high homocysteine. Those who do will reliably develop dementia and lowering it reliably reduces their cognitive decline. So, high homocysteine is a CAUSE, but not the only cause. Insulin resistance leads to diabetes and increases the risk for dementia. So, insulin resistance driven by too much sugar and refined carbohydrates is probably a cause, but not the only one. There isn’t enough evidence yet to declare ‘cause’ but the evidence that exists points that way.
There is a different way of thinking and researching called system-based science. Much like the straw that breaks the camel’s back this approach presumes there are a number of conditions, not just one, that result in a disease such as Alzheimer’s or dementia. After all, a stroke or head injury can be a cause of cognitive decline even if you don’t have high homocysteine or blood sugar problems. (It could be that a potential causal mechanism that ties these together is cerebrovascular dysfunction – disturbed blood supply to the brain. High homocysteine, by the way, increases risk of this by 17-fold).
In my book Upgrade Your Brain, which gives all the reference studies for statements made in this article, I argue that every known risk factor or biomarker for cognitive decline, dementia or Alzheimer’s affects either the structure, the function or the utilisation of the neuronal network and that it is combinations of these that crank up risk and ultimately brain pathology. We will publish a paper on this soon in a scientific journal.
It’s like saying five critical things have to work for your car to move forward and not crash. Tyre pressure good, brakes working, enough gas, oil and water for the radiator to cool the engine. If any one of these is completely broken the car stops or crashes. If two are not working well, such as low oil and low water, the car grinds to a halt. If a car approaches too close (like a potential head injury) and one tyre is quite flat and the brakes aren’t working well, you crash.
We tend to think in this way in nutrition and lifestyle medicine. It’s the combo of insults – high sugar, high fried foods, lack of veg, too much alcohol, smoking, that breaks the camel’s back. That heart attack is the ‘perfect storm’ of several underlying factors.
—
The (unpopular) system-based approach
This systems-based approach isn’t popular in science and very few funders ever put up money to fund this kind of research. Usually, a funder wants to fund one stream of research, possibly a clinical trial of one approach, in the belief that that one factor is the final straw that breaks the camel’s back and a great discovery will be made. The reality is that it is usually combinations of factors that drive risk with the manifestation of the disease itself being the ‘broken back’. Pollution, for example, is a risk factor for dementia…but not in those with good vitamin B6, folate or B12 status, which are the three B vitamins needed for methylation, indicated by lower homocysteine. Methylation is a major mechanism the body uses to detoxify pollutants and toxins.
This is where Food for the Brain’s approach is unique.
By collecting data from people like you who have both taken the Cognitive Function Test and completed the COGNITION questionnaire, and keep doing so, we can look at what drives cognitive function up and down. In other words what breaks the camel’s back or makes it strong. This kind of complex systems-based science has become possible both due to big data gathering such as we are doing, advances in complex statistics, computer power and programming AI algorithms. Our Head of Science, Associate Professor Tommy Wood, is a bit of an expert in this kind of approach to neuroscience.
It is, I believe, the future and why we will probably find no single primary cause for Alzheimer’s, and certainly not amyloid or p-tau, but combinations of diet and lifestyle and other factors that create the tipping point that leads to dementia. Then, we will have the means to prevent this tipping point from ever being reached. In other words, we may discover that prevention is the cure. We hope that you’ll be part of this discovery. By becoming a FRIEND or making a DONATION you help us research what really causes, and prevents Alzheimer’s.
Similarly, if you’re inspired by our mission and would like to support groundbreaking research into the prevention and early detection of cognitive decline, consider investing in the global COGNITION Biobank project. Your contribution will help drive transformative research and create lasting change. To learn more, email us at donations@foodforthebrain.org
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.