Lithium and Brain Health: The Overlooked Mineral That Could Protect Your Mind
Lithium and Brain Health: The Overlooked Mineral That Could Protect Your Mind
by Greg Potter
Lithium and brain health are more connected than many realise. One of the universe’s oldest elements could also be one of the brain’s most powerful protectors.
Long associated with bipolar treatment, lithium is often dismissed as a heavy-duty psychiatric drug – yet new research tells a different story. Trace amounts of lithium appear to influence mood, longevity and even cognitive decline. With dementia rates rising fast, scientists are revisiting this humble mineral to understand whether it could slow or prevent neurodegeneration altogether.
In this article, Dr Greg Potter, member of our Scientific Advisory Board and Sleep Scientist, explores the remarkable – and misunderstood – role of lithium in supporting brain health, from dementia protection to lifespan extension and neural resilience.
Lithium is one of three elements created during the Big Bang event that gave rise to the universe 13.8 billion years ago, and nowadays it’s mostly found in igneous rocks.
Because lithium predates all life on Earth, it’s perhaps no surprise it plays a role in human biology. While lithium doesn’t seem to be a truly “essential” nutrient (1) as it isn’t indispensable for any one biological process, lithium’s mood-stabilising actions have long been recognised. Specifically, lithium has primarily been used to help patients with bipolar disorder avert swings into sleepless mania. Despite its clinical utility, lithium has arguably been stigmatised due to its association with mental illness, its side effects at high doses, and perceptions that it’s an outdated drug with superior, more modern alternatives – a perspective that frankly defies reality. Some astute individuals have understood lithium’s greater promise for years; however, lithium was recently thrust back into the spotlight.
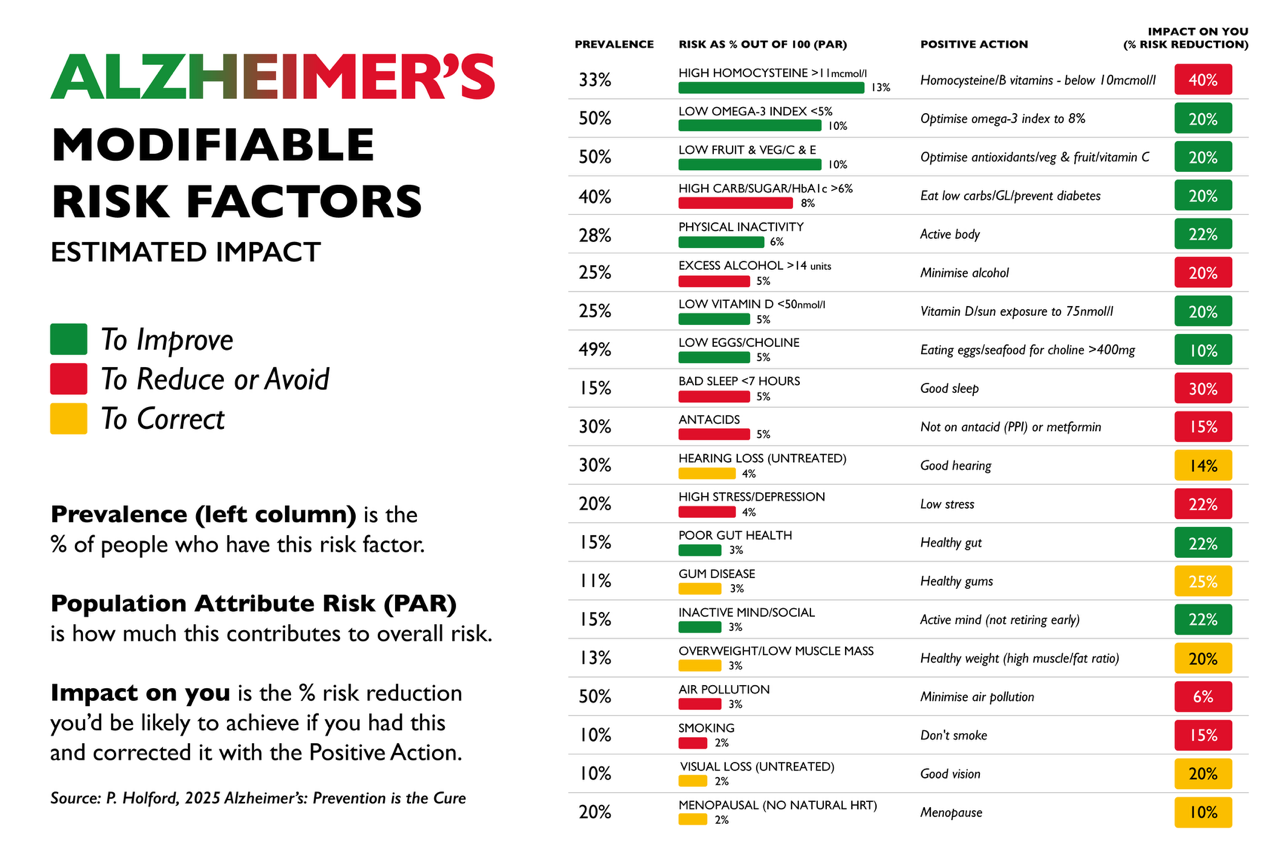
A recent high-profile publication showing promise of lithium in mitigating Alzheimer’s in the prestigious journal Nature (2) means we are finally waking up to just how interesting and helpful lithium can be.
Could lithium help prevent or treat dementia?
Research into lithium effect on brain health goes back longer than many realise. Several studies have associated lithium use with reduced risk of dementia (3), and scientists have also considered lithium as an adjunct treatment for patients who already have dementia. An experiment (4) on Alzheimer’s disease patients found that supplementing just 300 mcg lithium (as carbonate) per day for 15 months prevented deterioration in cognitive function, which continued to decline in people taking a placebo. While not all research has reported such positive effects, the early evidence is encouraging, and discrepancies between studies might be explained by variables such as discrepant lithium forms and doses.
Returning to the 2025 publication that caused such a stir, the researchers undertook a range of experiments to try to decipher lithium’s effects. First, when they looked at levels of metals in the brains of cognitively healthy adults, people with mild cognitive impairment, or individuals with Alzheimer’s, they found higher levels of lithium in a part of the brain key to processes such as planning and decision making in the cognitively healthy. They also explored the effects of adding lithium orotate, a salt of lithium, to the drinking water of mice genetically engineered to develop a condition similar to familial Alzheimer’s, the aggressive, early-onset form of the disease that runs in families. Compared with the lithium-free condition, even very low doses of lithium orotate dramatically reduced the characteristic misfolded brain proteins that occur in Alzheimer’s, also potentially allaying cognitive decline. Promisingly, lithium also exerted similar protective effects in “wild type” mice. These mice lack the genetic changes that cause early-onset Alzheimer’s, making them a better model for most people.
Does Lithium Extend Lifespan? What the Evidence Suggests
My interest in lithium is tentative evidence from the last couple of decades positively associating intakes with lifespan. This link has been shown in the general population, but there’s also the intriguing finding that people medicated with lithium for psychiatric conditions live longer than their peers taking alternative medications (5). Some of lithium’s effects on mood might mediate the relationship between higher lithium intake and longer life. Tragically, suicide is a common driver of deaths in young adults, and studies of large groups of people have linked higher lithium intakes with lower suicidality (6), which by itself would extend lifespan a little. However, the effects of lithium on mood might not be the whole story, and scientists who study the biology of ageing (geroscientists) have started to test whether lithium extends lifespan in non-human animals.
So far, the jury is out, for while lithium has been found to extend life in yeast, roundworms, and flies (7, 8 ,9), it didn’t do so in mice, although male mice consuming lithium did seem to have better body composition and blood sugar control (10). Again, perhaps lithium form, dose, and age of use matter though. Overall, lithium certainly doesn’t seem to hurt lifespan, and it might prove modestly beneficial for healthspan (let’s define this as days of life free from disease or disability) and lifespan in a subset of people – but more research needs to be done.
How Lithium Supports Brain Cells and Mood Stability
Regarding how lithium supports mood stability and protects the brain against degeneration (11), as usual, we’re not sure. Most of the relevant research has used the equivalent of very high lithium doses, but I’ll mention a few mechanisms that have substantial empirical support.
Lithium can enter cells through sodium channels, and by competing with sodium and magnesium it can reduce activity of enzymes activated by these other minerals. Perhaps the best-accepted instance of this is lithium’s inhibition of glycogen synthase kinase-3β, an enzyme so named because, among other actions, it reduces activity of an enzyme that synthesises the storage form of carbohydrate, glycogen. This, plus inhibition of other key enzymes, such as inositol monophosphate, set in motion changes in the expression of myriad gene networks involved in brain health, including enhancing clearance of dysfunctional cells and hence improving regulation of proteins in the brain, reducing brain inflammatory responses and hence collateral damage, and promoting the neuroplastic processes needed to remodel the brain to thrive in the dynamic environments in which we live.
Interestingly, the kinds of high lithium doses used to treat bipolar also support body clock function and sleep, which often go awry before mental illness sets in. Lithium has been shown to influence the body clock at several levels of organisation, from individual cells to people’s rest-activity timing (12), shifting the sleep-wake cycle earlier, making the cycle more regular, and increasing its amplitude. High doses also tend to deepen sleep (13), and deep sleep is a key player in mood regulation and brain maintenance processes, such as waste clearance. (Incidentally, a big part of why appropriate exercise is so good for the brain is that it tends to deepen sleep.) Again, we’re talking about large doses here though.
How Much Lithium Do You Need – and Is Supplementation Safe?
Several factors make it difficult to give clear recommendations regarding lithium intakes.
Firstly, none of us really have any idea how much lithium we regularly consume. Lithium intakes vary enormously between populations, based partly on the physical geography of where people live (over half the world’s lithium is concentrated in Argentina and Chile). This affects how much lithium gets into local drinking water and food. Even then, in much of the world people drink water and eat food that doesn’t come from nearby. Next, your lithium intake would ideally map to your bodily lithium status and needs, and we don’t have good proxies for these at present. There’s also the fact that lithium comes in different salts. Lithium carbonate is most widely used in psychiatry, followed by lithium citrate. However, there’s experimental evidence that lithium orotate is more bioavailable than both, and this superiority of orotate was born out by the recent Nature publication, albeit for different reasons (related to reduced lithium uptake by amyloid). Finally, lithium is used as a medication and is quite tightly regulated in some parts of the world. The salt we know most about (carbonate) is therefore off limits for most of us, although given the early promise of lithium orotate, that might be no issue.
I’m not a medical doctor and recommend running the supplements you take by a qualified medical professional – just bear in mind that most medical doctors know very little about nutrition and supplementation. I would consider a dose of up to 1 mg elemental lithium per day to be reasonable, provided it’s from a reputable manufacturer. People not very familiar with lithium doses might think of some of the adverse effects of high dose lithium intakes, which can include kidney toxicity. To be clear, my suggestion is well below the amount of lithium consumed from diet alone in much of the world, which most people have never thought twice about.
I have no affiliation with either, but both Swanson and Life Extension sell low- or trace-dose lithium orotate, and the data I’ve seen suggest their products are high quality and contain what they claim they do. (In fact, there’s been research (14) showing the Swanson low-dose lithium orotate product raises brain lithium in adults.) Part of the difficulty here is that, in my opinion, the lithium doses in many supplements might be higher than is ideal. Based on the work on trace dose lithium use in dementia, plus the apparent higher bioavailability of lithium orotate (15), I think 300 to 400 mcg lithium orotate is an excellent starting point. That dose is more than conservative yet should be sufficient to be beneficial, and my approach to supplementation is generally to choose the lowest dose shown to have the effects you’re after.
Parting words
In summary, while lithium is not an essential micronutrient, the human brain seems to thrive when it has enough lithium. To ensure you’re providing your brain with what it needs, a lithium supplement providing a trace dose (less than 5 mg elemental lithium) each day seems to be a reasonable, safe way to ensure this. If you’re interested in learning more about lithium, in 2024 I interviewed Dr Becci Strawbridge, an expert in low-dose lithium. The conversation is available on all major podcasting platforms. It’s also on YouTube here.
Note: These words are solely the opinions of the author. (He used no large language models to help write this article.)
About Greg Potter
Greg helps individuals and organisations sustainably improve their health and performance. He does this through developing and popularising innovative businesses and products, coaching, public speaking, consulting, and empowering people through educational resources such as e-books, articles, and courses. Among other roles, Greg is a Sleep Coach at the London Psychiatry Clinic and is Chief Science Officer at Coastline Longevity, where he leads the formulation of supplements to extend healthspan. He also hosts the Reason & Wellbeing podcast and YouTube channel.
Greg’s PhD research spanned sleep, circadian rhythms, nutrition, and metabolism. Highlights of Greg’s career include having this research featured in dozens of international news outlets, including the BBC, Reuters, and The Washington Post; having his writing featured in many newspapers and magazines, including The Metro, Stylist, and Newsweek; coaching a sprinter to four gold medals at the European Championships; and helping athletes break multiple World Records in ocean rowing.
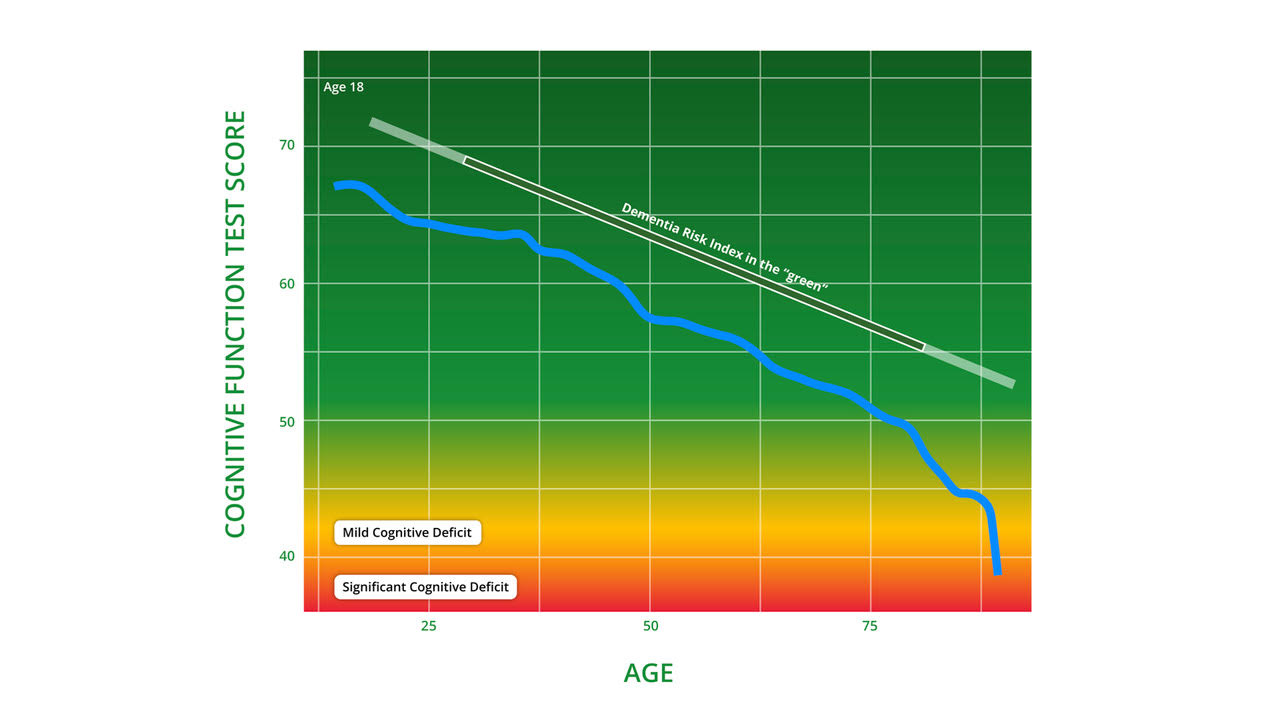
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices.
Please support our research by becoming a Friend of Food for the Brain.
Reference:
8 https://pubmed.ncbi.nlm.nih.gov/17959600/
15 https://pubmed.ncbi.nlm.nih.gov/37356352/