
The Science behind our Cognition Tools
What is the basis of the Cognitive Function Test? How do I know it is an accurate assessment of my cognitive function?

In 2011 we (Dr Celeste de Jager & Catherine Trustram-Eve) created a digital online Cognitive Function Test used to assess cognitive health and screen for MCI and dementia and made it available, for free, online having validated it the standard cognitive function test used in memory clinics. To date over 370,000 have taken the test demonstrating huge appetite for this sort of tool.
The Cognitive Function Test measures the critical aspects that indicate risk: episodic memory, attention and executive function.
Decline in these aspects of cognition, plus an accelerated rate of brain shrinkage, are the hallmarks of cognitive impairment.
The Cognitive Function Test is available for use by research groups needing an accurate assessment of cognitive function such Weill Cornell Medicine in New York.
For more information on our Cognitive Function Test, the domains tested, how we computerised and validated it and the supporting science research click here.
What is the basis of the Dementia Risk Index questionnaire. How do I know it is an accurate assessment of my risk?
In 2018 we introduced a risk factor questionnaire and commenced a research project to inform the building of an interactive, effective means of changing key diet and lifestyle behaviours to reduce risk and asked University College London and NHS researchers to test it, and explore barriers and weaknesses to increase compliance and behaviour change. They reported that 88% found in useful and 37% made diet or lifestyle changes as a result. Our goal is to substantially improve these percentages.[1]
Numerous studies investigating the ‘population attributable risk’ have attributed around half of the risk to modifiable risk factors – that is things you can change. This was the conclusion in a statement from an international group of 111 scientific and medical dementia experts from 36 countries world leading dementia experts, and thus is, theoretically, preventable.[2] This evidence was presented in the G8 summit on dementia in London in December 2013. Just one in 100 cases of Alzheimer’s are caused by mutations in genes (presenilin, APP) which account for a most of the familial, early onset cases. [3] At the time the consensus group stated that it is possible right now to cut the number of people who will develop Alzheimer’s by a fifth. But if all known modifiable risk factors are targeted this could reduce the incidence of dementia by a third.
The questions that make up the Dementia Risk Index cover eight domains of known risk. This risk has been established in various systematic reviews and meta-analyses of studies [4] [6] [7] [8] [9] [10] [11]. For example, Scientists at the US National Institutes of Aging found that risk factors for Alzheimer’s that account for most cases are high homocysteine (22% of risk) which is lowered by B vitamins, lack of seafood/omega-3 (22%) active lifestyle (32%) and low educational attainment (24%) and mid-life smoking (22%).[12] The most comprehensive meta-analysis of 396 studies by Professor Jin-Tai Yu, a member of our Scientific Advisory Board, found “10 with Level A strong evidence (education, cognitive activity, high body mass index in late-life, hyperhomocysteinaemia, depression, stress, diabetes, head trauma, hypertension in midlife and orthostatic hypotension) and 9 with Level B weaker evidence (obesity in midlife, weight loss in late life, physical exercise, smoking, sleep, cerebrovascular disease, frailty, atrial fibrillation and vitamin C).” Knowing, however, that something is a risk factor does not mean you can change your risk. For example, having had a head trauma increases you risk but is not something that you can change. Professor Yu’s study noted that ‘homocysteine lowering treatment [with B vitamins] seems the most promising intervention for Alzheimer’s disease prevention, in agreement with a recent report.’[13]
The Dementia Risk Index (DRI) covers only factors you can change, from diet to lifestyle. Having the ApoE4 gene increases your possible risk but you cannot change it, although you can modify even that risk by making positive changes to your diet and lifestyle.
The DRI organises these risk factors into eight domains. Smoking and vitamin C, for example, is an aspect of the ‘antioxidant’ domain. Excess weight is an aspect of the ‘low carbs & GL’ domain. Sleep, depression and stress are aspects of the ‘sleep and calm’ domain.
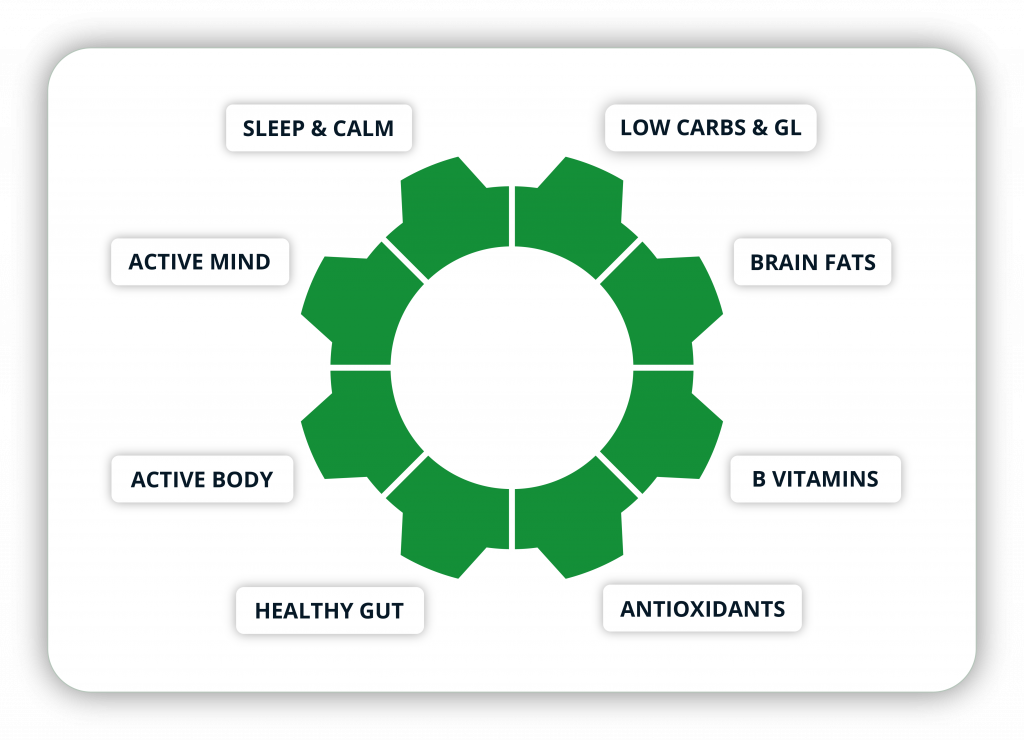
Based on the available evidence the DRI assigns a percentage of overall modifiable risk to each domain as follows, adding up to 100%:
Active Body 15%
Active Mind 10%
Sleep & Calm 10%
Glycemic Load 15%
Antioxidants 10%
Brain Fats 17%
B Vitamins 18%
Gut Health 5%
In essence, having the highest possible score, 100%, means you are doing everything we know of to increase your risk. It does not mean your risk of developing dementia is 100%. Conversely, if you score 0% you are doing everything you can to reduce your risk but it doesn’t necessarily mean you are risk free. Given that approximately 50% of risk is attributed to these modifiable risk factors theoretically you can increase or decrease your risk by 50%. However, one study found that those doing all the right dietary things reduce their risk by 86 to 90%.[14] How could this be possible if only 50% of risk is attributed to things we can change? The remaining 50% is made up of things you can’t change, like head injury, or poor early life education or predispose genes that increase your risk such as ApoE4, which increase your risk. But what if none of those apply to you? Then, all your risk might be under your control. Also, even predisposing genes can be dampened down by what you eat and how you live.
The battery of questions within each domain are weighted such that some questions are more important than others. Most questions are on a scale of five answers.
The Dementia Risk Index questionnaire is part of ongoing research since its validity can only be truly established once thousands of people have completed it, made or not made changes, and either developed dementia or not. Our first research objective is to see how the DRI correlates with the CFT, which is an actual measure of cognitive function, therefore a good indicator of dementia risk since a decrease in cognitive function is the main diagnostic criteria. We want to know, across different age ranges, if people who score low or high on the DRI score low or high on the CFT. Also, if a person lowers there DRI does there CFT improve, or the rate of loss of function over years reduce.
Only then can we look at specific domains, and even specific questions, to see which specific changes makes the biggest difference to cognitive function and future risk for dementia. Our aim, with funding is to do this research and improve the predictive accuracy of the DRI. With that goal in mind we have Dr Kristina Curtis, from the centre for Behaviour Change at UCL, our expert in Digital Behaviour Change Interventions that promote effective engagement.
What is the basis of COGNITION? How do I know that following the advice given will reduce my risk?
In 2018 we introduced a risk factor questionnaire and commenced a research project to inform the building of COGNITION an interactive, effective means of changing key diet and lifestyle behaviours to reduce risk and asked University College London and NHS researchers to test it, and explore barriers and weaknesses to increase compliance and behaviour change. They reported that 88% found in useful and 37% made diet or lifestyle changes as a result. Our goal is to substantially improve these percentages.[15]
We hope that the positive, personalised, interactive, educational, encouraging journey through each domain, giving clear and doable actions, starting with a person’s weakest domains, with the support group for people to share what works and ask questions, will substantially increase both the number of people who make positive changes, and the number of changes they make, reflected in a lower DRI score. As more people join we will be able to find out, and as we find out what works and what doesn’t COGNITION will be adapted accordingly. We also keep abreast of other studies that aim to change behaviour to learn from them what does and doesn’t work.

Will making these changes lessen risk? That is why we are tracking your DRI and your cognitive function, reassessing your cognitive function every six months. Other research groups will also examine our anonymised data in an international collaboration to learn what really works. For example, we hope to run the CFT/DRI on several thousand people who know their vitamin D levels. Do those with higher vitamin D levels have better cognitive function? Studies show that this is likely to be the case.
To further evolve the science of dementia prevention our Scientific Advisory Board consists or top exerts in each domain, from Emeritus Professor David Smith, who research giving B vitamins showed up to 73% less brain shrinkage[16] or Dr William Grant, who focusses on vitamin D. Others focus on the role of sugar and metabolic disorders and dementia (Dr Robert Lustig); and the role of diet, fruit and vegetables high in antioxidants and polyphenols (Jeremy Spencer, Professor of nutritional biochemistry at the University of Reading). Dr David Vazour, from the University of East Anglia is an expert in the gut, health and the brain. Dr Simon Dyall, from the University of Roehampton, is the Director of the International Society for the Study of Fatty acids and Lipids – think omega-3. Associate Professor Dr Thomas Wood, from the University of Washington, advises us on an active lifestyle, while Dr Phuong Leung is an expert in keeping your mind active and its effects on dementia. The can see the existing evidence for each of the 8 domains here
The science, and art, of helping people change their diet and behaviour to reduce future risk of dementia is constantly evolving and in its relative infancy. We hope to stay at the leading edge of the application of the science for your benefit and will share the results of our research with the community of Friends of Food for the brain and COG-NITION users. Please also note that the vast majority of COG-NITION encourages you to make also reduce risk of other diseases, both mental and physical, including diabetes and heart disease. Thank you for being part of our research community.
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices.
Please support our research by becoming a Friend of Food for the Brain.
References
[1] M. Bird, C. Cooper, F. Patel, C. Copeman, J.L. Stansfeld, G. Charlesworth, E. Aguirre, The psychological determinants of making lifestyle and dietary behaviours after using an online cognitive health tool and its associated recommendations for protective cognitive health behaviours,The European Journal of Psychiatry,Volume 35, Issue 3,2021,Pages 145-https://doi.org/10.1016/j.ejpsy.2021.02.001.
[2] Smith AD, Yaffe K, ‘Dementia can be prevented: Statement supported by international experts’, Journal of Alzheimer’s Disease 38 (2014) 699–703
[3] Bekris L et al, ‘Genetics of Alzheimer disease’ Journal of Geriatric Psychiatry and Neurology 2010, 23(4) 213-227
[4] Beydoun M et al, ‘Epidemiologic studies of modifiable factors associated with cognition and dementia: systematic review and meta-analysis’ BMC Public Health 2014, 14:643
[6] Yu JT, Xu W, Tan CC, Andrieu S, Suckling J, Evangelou E, Pan A, Zhang C, Jia J, Feng L, Kua EH, Wang YJ, Wang HF, Tan MS, Li JQ, Hou XH, Wan Y, Tan L, Mok V, Tan L, Dong Q, Touchon J, Gauthier S, Aisen PS, Vellas B. Evidence-based prevention of Alzheimer’s disease: systematic review and meta-analysis of 243 observational prospective studies and 153 randomised controlled trials. J Neurol Neurosurg Psychiatry. 2020 Nov;91(11):1201-1209. doi: 10.1136/jnnp-2019-321913. Epub 2020 Jul 20. PMID: 32690803; PMCID: PMC7569385.
[7] Livingston G, Huntley J, Sommerlad A, Ames D, Ballard C, Banerjee S, Brayne C, Burns A, Cohen-Mansfield J, Cooper C, Costafreda SG, Dias A, Fox N, Gitlin LN, Howard R, Kales HC, Kivimäki M, Larson EB, Ogunniyi A, Orgeta V, Ritchie K, Rockwood K, Sampson EL, Samus Q, Schneider LS, Selbæk G, Teri L, Mukadam N. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020 Aug 8;396(10248):413-446. doi: 10.1016/S0140-6736(20)30367-6. Epub 2020 Jul 30. PMID: 32738937; PMCID: PMC7392084. ; see also Livingstone_LancetCommission2017.pdf
[8] Elwood P, Galante J, Pickering J, Palmer S, Bayer A, et al. (2013) Healthy Lifestyles Reduce the Incidence of Chronic Diseases and Dementia: Evidence from the Caerphilly Cohort Study. PLoS ONE 8(12): e81877. doi:10.1371/journal.pone.0081877
[9] Norton S et al, ‘Potential for primary prevention of Alzheimer’s disease: an analysis of population-based data’, Lancet Neurol 2014;13(8):788-94
[10] Ashby-Mitchell et al. Alzheimer’s Research & Therapy (2017) 9:11 DOI 10.1186/s13195-017-0238-x
[11] Mayer et al.: An Estimate of Attributable Cases of AD and VaD due to Modifiable Risk Factors: The Impact of Primary Prevention in Europe and in Italy Dement Geriatr Cogn Disord Extra 2018;8:60–71
[12]Beydoun M et al, ‘Epidemiologic studies of modifiable factors associated with cognition and dementia: systematic review and meta-analysis’ BMC Public Health 2014, 14:643
[13] Kane RL, Butler M, Fink HA, et al. Interventions to prevent age-related cognitive decline, mild cognitive impairment, and clinical Alzheimer’s-type dementia. Rockville (MD, 2017.
[14] M. Eskelinen et al., Dement Geriatr Cogn Disord Extra 2011
[15] M. Bird, C. Cooper, F. Patel, C. Copeman, J.L. Stansfeld, G. Charlesworth, E. Aguirre, The psychological determinants of making lifestyle and dietary behaviours after using an online cognitive health tool and its associated recommendations for protective cognitive health behaviours,The European Journal of Psychiatry,Volume 35, Issue 3,2021,Pages 145-https://doi.org/10.1016/j.ejpsy.2021.02.001.
[16] Smith AD, Smith SM, de Jager CA, Whitbread P, Johnston C, Agacinski G, et al. Homocysteine-lowering by B vitamins slows the rate of accelerated brain atrophy in mild cognitive impairment. A randomized controlled trial. PLoS ONE. 2010; 5: e12244; de Jager CA, Oulhaj A, Jacoby R, Refsum H, Smith AD. Cognitive and clinical outcomes of homocysteine-lowering B-vitamin treatment in mild cognitive impairment: a randomized controlled trial. Int J Geriatr Psychiatry. 2012; 27: 592-600; and Jernerén F, Elshorbagy AK, Oulhaj A, Smith SM, Refsum H, Smith AD. Brain atrophy in cognitively impaired elderly: the importance of long-chain omega-3 fatty acids and B