By Patrick Holford

Raised homocysteine, the best indicator of your ‘methylation’ ability, is not only causal for Alzheimer’s disease but probably also for strokes and several other diseases in the 100 diseases for which homocysteine is a biomarker.
However, homocysteine is easily measured and is also easily optimised. It is most directly lowered by vitamin B12, folate and B6. There are other nutrients that also help, but these B vitamins are the most essential.
If you’re new to understanding why improving methylation lowers homocysteine, this film will give you an idea of what’s going on thousands of times every second in your brain and body. Watch it below.
—
—
This further exploration into some close-up details regarding homocysteine comes from lengthy articles I’ve read which have made things too complicated and often inaccurate; such as people being either over- or under-methylated, and folic acid being the devil incarnate and other such things. So, I thought I’d clarify some misconceptions floating around the world of nutritional therapy.
—
It is a toxic amino acid, an intermediary made from the essential amino acid methionine in your proteinous food, en route to make S-Adenosyl Methionine (SAMe) which juggles methyl groups (CH3) as a methyl donor/acceptor and as the master of the brain and body’s orchestra, with several billion such reactions every minute. And that’s only half the story.
There is no good reason to want homocysteine in your blood because it damages arteries. But if you had absolutely none that would be weird. It would be like having no garbage in your house at all and none in the bins. Now, you don’t want to accumulate garbage, but you’ve always got a rubbish bin on the go.
While a homocysteine level above 11 mcmol/l is strongly associated with accelerated rate of brain shrinkage and is probably also an appropriate reference point for increasing stroke and cardiovascular risk, problems can occur in children if their mothers had a level above 9 mcmol/l during pregnancy. In one study cognitive decline seemed to increase from 8 mcmol/l. In another study chromosomal damage to genes occurs above a level of 7.3 mcmol/l. My best guess, having seen hundreds of clients, is that having a homocysteine between 4 and 7 mcmol/l is probably optimal, with older people in their 80’s or 90’s often struggling to keep below 9 despite doing the right things.
—
—
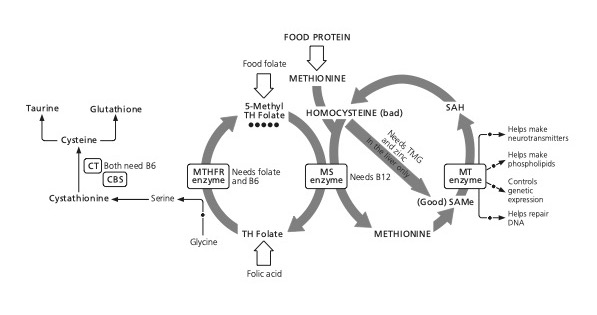
Can homocysteine be too low? I think this answer is ‘possibly’. Having a level below 4 is rare in and of itself. Even rarer is for someone to have a level below 4 and a problem. Why could too low be a problem? The second part of the story is that homocysteine can be turned into glutathione, the master antioxidant via the ‘sulphuration’ pathway, through the interaction of B vitamins on homocysteine in the presence of glycine (a sulphur container amino acid). This involves an enzyme, CBS (cystathionine beta synthase) which is dependent on vitamin B6.
Theoretically, if there wasn’t enough homocysteine, then this pathway for making glutathione would be in short supply. Such a finding has been shown in some children with autism, but it is very rare. And how would you know that the very low homocysteine, below 4 mcmol/l, was a bad thing, leading to less glutathione? I’d test the person’s glutathione or, more accurately, their Glutathione Index. Think of glutathione as the good guy, made from recycling rubbish, and homocysteine as the bad guy.
If both were low I’d be thinking ‘where is the log jam’? You can see in the diagram above that the cheap, stable, inexpensive folic acid should turn into TH Folate, then, via the action of the MTHFReductase enzyme, into 5-methylfolate, or reduced, fully loaded folate, used in the body and brain in a thousand ways. But we must also note that CBS enzyme, dependent on vitamin B6 (itself dependent on zinc to be ‘activated’) must be fully functional. This pathway, if working properly, would naturally create glutathione, the body and brain’s master antioxidant.
—
—
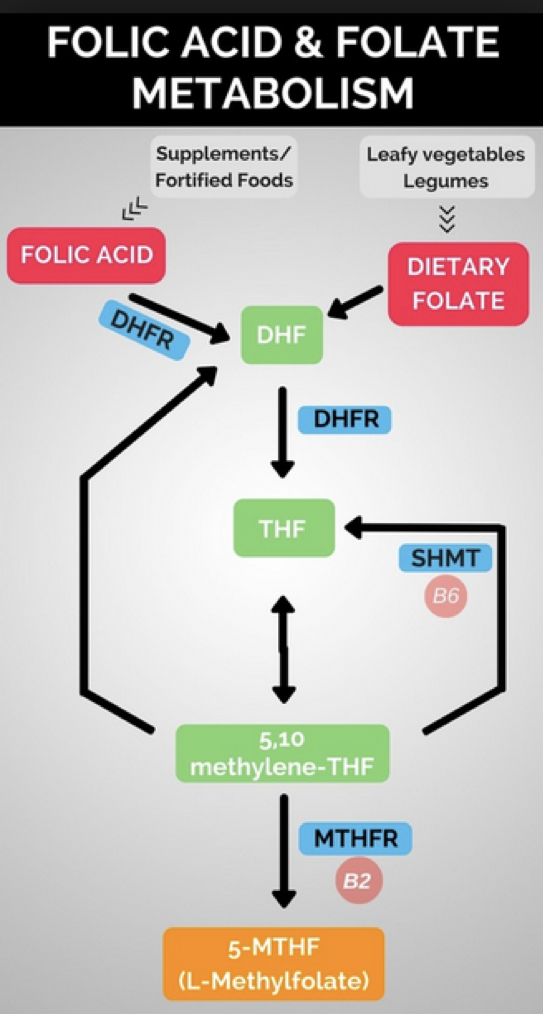
If this pathway is not working effectively, and both homocysteine and Glutathione are low, I’d suspect two ‘faulty’ enzymes. That is either the enzyme DHFR that does the first step in activating folic acid or MTHFR, which does the second step. This is dependent on vitamin B2 (riboflavin).
Enzymes are built from a genetic blueprint. If you inherit a slightly dodgy blueprint, your enzyme factory turns out cheap goods. You might then need a little help from riboflavin (B2) for those who inherited the gene MTHFR677T or TT. We all need B2, but this enzyme won’t work nearly so well if you’re deficient and have this genetic ‘polymorphism’. That is why having MTHFR677T or TT, which is present in about 24% of people (10% in Africans, 34% of Europeans) puts up a person’s risk for Alzheimer’s. But, in studies giving the three main co-factor nutrients – B6, folic acid and B12 – it makes no difference whether or not you have this dodgy gene. Homocysteine still gets lowered. That’s right. Folic acid works, both in combination, and on its own, in lowering high homocysteine and is turned into the activated form methylfolate without a problem. So that suspected enzyme variation, especially if you have enough B12, is not looking so critical. In all studies I’ve seen, where B6, B12 and folic acid is given, the beneficial effect is the same in both those with or without this gene ‘defect’.
—
The second suspect is a variation in the gene that makes the enzyme DHFR. Think of these gene ‘defects’ as resulting in less of the enzyme. As a consequence your body’s biochemistry wouldn’t be able to turn all folic acid into methyl folate. You’d then accumulate UnMetabolised Folic Acid (UMFA for short). Why would that be a problem? Well, folic acid still looks like methylfolate, and enzymes have a lock shaped for the key – that is their co-factor, such as folate. Too much folic acid in the blood could block all those enzyme receptors such that the enzymes don’t work so well, effectively inducing a folate deficiency. The net result in this scenario would be less glutathione.
A good example of how a less effective form of a vitamin can induce a vitamin deficiency in certain circumstances is vitamin B6. Those familiar with vitamin B6 (pyridoxine) know that it has to be turned into pyroxidal-5-phosphate (P5P) to become active, which requires zinc. If you supplement way too much vitamin B6 – 1 gram for example – and especially if you are zinc deficient, the unmetabolized B6 can block B6 dependent enzymes from working and you end up with similar symptoms of neuropathy also reported in those deficient in vitamin B6.
So, too much folic acid – for example over 1 gram – coupled with a dodgy DHFR gene would be bad news inducing something equivalent to folate deficiency. This then raises two questions: how much folic acid is too much? How many people have DHFR gene mutations?
The first answer depends somewhat on the second since those with a ‘bad DHFR gene’ are less able to cope with folic acid. The worse DHFR status is called a double deletion. How common is it? Not common in Europeans. It is very common in Asian ethnicities. These people would be less likely to benefit from folic acid because they can’t activate it. This is exactly what studies have shown. Folic acid lowers homocysteine and improves cognitive function less well in those with this gene polymorphism. Giving these people lots of folic acid will result in lots of unmetabolized folic acid (UMFA) accumulating and blocking real folate enzyme activity. This is effectively a B vitamin deficiency induced by a B vitamin.
While it could be argued that these people shouldn’t really be supplementing any folic acid there is little evidence to show that a lowish amount, let’s say up to 200 mcg in a multi, for example, is likely to be a great cause for concern.
But, especially for DHFR gene defectives, it is so much better to cut to the chase and supplement the activated methyl-folate form of this vitamin or its precursor folinic acid. An example of this is a study on autistic children, which gave folinic acid and tested an indicator of glutathione status. Those children with poorer glutathione status did better. Unfortunately they didn’t test DHFR gene status.
They could have given methylfolate but the trouble with methylfolate is that it is very unstable, until the recent developments of three stable versions of methlyfolate:
Unlike folic acid, originally patented by Roche, but now expired, these other superior methylfolate forms of the vitamin are more expensive and with that comes more marketing muscle to switch buyers and makers of supplements and food fortification from folic acid to methylfolate. Leaving money to one side, it is generally a good idea to switch to methylfolate. It does lower homocysteine and raise red blood cell folate more effectively.
But it is wrong to say that folic acid doesn’t work in lowering homocysteine. It does and especially in the majority of Europeans without the DHFR gene defect. In East Asians I’d be more inclined to give methylfolate.
Methylfolate has been shown to raise folate levels better than folic acid and to lower homocysteine more effectively. In one study, 100µg of methylfolate lowered homocysteine by 14.6% compared to folic acid which lowered it by 9.3% in 24 weeks. In another it both raised red blood cell folate by 30% more than folic acid and it also lowered Hcy by 13.8% compared to 9.9% for folic acid. This means that methylfolate lowers homocysteine 40-50% more than folic acid.
Now, if you’ve had a homocysteine test, which I strongly advise in anyone over 50 or with any of the 100 diseases for which homocysteine is a biomarker, the great news is that almost all homocysteine lowering supplements (see here for more guidance on supplements) only use methylfolate alongside B6, B12, TMG, zinc and NAC or glutathione.
If your level is below 4 mcmol/l AND you have any symptoms that also occur with folate deficiency (those 100 diseases that homocysteine is a biomarker of is a good starting point) then I’d recommend two things:
—
The short answer regarding unmetabolised folic acid is probably yes, it probably is bad for you.
Cancer cells are growing fast and need folates to do so. Having lots of folic acid in your bloodstream, seems to be a problem. Could too much folate in your bloodstream be a problem? Theoretically yes but generally, those eating a high folate diet rich in vegetables for example, have lower risk. But there’s a lot more in vegetables than just folate.
I asked a folate expert, Dr Martin Ullman, regarding the cancer connection. “Folates are micronutrients, and any micronutrients are growth factors for healthy cells but even more for fast growing cancer cells. If there are precancerous conditions, “high” intake of folate may promote the progression to a cancerous condition. On the other hand, regular satisfactory intake of folate (before any precancerous condition) is preventive.”
Perhaps the riskiest scenario would be in those with that dodgy DHFR polymorphism that’s much more common in Asians, combined with a bad diet fortified with folic acid and unable to metabolise it and also with a pre-cancerous condition. Colorectal polyps, potentially pre-cancerous cells, would grow faster with more folic acid.
Also, bear in mind that raised homocysteine is, in any event, bad news for cancer. The majority of cancers are associated with faulty methylation so it’s one of the first things I’d check for. If raised, bring it down with a homocysteine lowering formula containing methylfolate, not folate.
For those who would like to dig even deeper, these papers are most relevant:
Thank you for reading!
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices.
Please support our research by becoming a Friend of Food for the Brain.
