
Myths about Alzheimer’s – from amyloid drugs to genes
The Myth of Genes
Before Hippocrates people blamed the gods for various diseases. Today people often assume ‘it’s in the genes’. If a person’s parent gets Alzheimer’s, or if Alzheimer’s occurs in one’s family that way of thinking often leads to the belief there’s nothing you can do about it. This is a major reason why some people don’t do our Cognitive Function Test to start the journey towards dementia-proofing your diet and lifestyle because they ‘don’t want to know’.
The reality is quite different. There are three causative genes for Alzheimer’s (APP, PSEN1, PSEN2). [1] So less than one in a hundred cases of Alzheimer’s is caused by genes.
Other genes may predispose or push you in that direction, but don’t cause. For example, having a variation of the ApoE gene, called ApoE4 gene, if expressed, may account for 4 to 6% of the inheritability of risk.[2]. Genes are instructions that make proteins. The APOE gene is involved in making a protein that helps carry cholesterol and other types of fat in the bloodstream.
Think of a gene like a programme on your computer. The programme could be turned on or off. The ApoE4 gene can be turned on, or expressed, or turned off. In truth, they are more like a dimmer switch and can be turned up (upregulated) or turned down (downregulated). An example of this is the BRCA gene. If a woman has this they are more likely to get breast cancer. But half do and half don’t. Why? Because the environment your genes are exposed to can turn up or turn down the gene’s expression. In the case of BRCA, soya turns it down, while cow’s milk turns it up. This is called ‘epigenetics’. Epi means ‘upon’ so is about things that act upon the gene.
So, if you are one of the 15% of people born with the ApoE4 variation of this gene this could increase your risk by a maximum of 4%. However, we are learning that eating “a low-glycemic index diet with a ketogenic option, specific Mediterranean-style food choices, and a panel of seven nutritional supplements”quoting a recent investigation called ‘Precision Nutrition for Alzheimer’s Prevention in ApoE4 Carriers’ [3] may well mitigate this risk by turning down the negative gene effect. The nutrients include B vitamins, vitamin D2 and K2, omega-3 DHA, and the antioxidant quercetin (red onions are a rich source) and resveratrol (in red grapes and wine). Every one of these diet factors are part of our recommended ways to reduce your risk that you’ll learnt about when you do the Cognitive Function Test.
11 other genes may account for up to 7.8% of the inheritability of AD.[4] Gene studies are suggesting that genes could account for a third of one’s inherited risk or predisposition. In other words, if you had all the wrong genes (excluding causative genes) and did none of the healthy things that dampen them down, you could be up to 33% more likely to get AD.
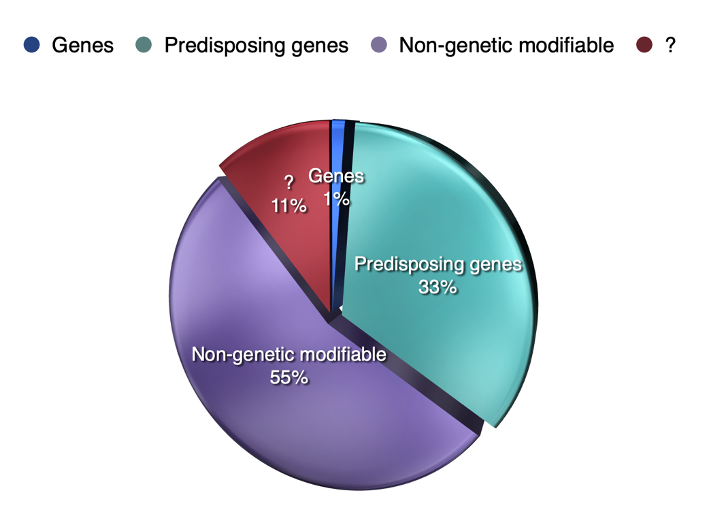
Remember, at least half (50%) of risk is attributed to things you can change. So you diet and lifestyle is much more important than genes. That means – surprise, surprise – that Alzheimer’s is another disease, like diabetes and heart diseases and also arthritis that is driven by a breakdown in your metabolism caused by sub-optimum nutrition and lifestyle. They have similar causes with the knock effect targeting different organs, be it your arteries, your joints, your brain or your blood sugar control. What that means is that when you reduce your Dementia Risk Index, which is the questionnaire you’ll complete when doing the Cognitive Function Test enabling us to personalise your prevention advice, you’ll be protecting not just your brain, but your body too.
Is amyloid a cause or consequence?
There’s a few things that are different in the brains of those who develop Alzheimer’s. They have high levels of homocysteine (see later), neurofibrillary tangles, and an increasing deposition of amyloid-B proteins leading to what’s often called ‘amyloid plaque’. Research has also identified P-tau proteins which leads to the build up of these neurofibrillary tangles, which is one of the hallmarks of Alzheimer’s. But are these high amyoid or p-tau protein levels the cause or the consequence? It’s like saying is the scarring in your damaged arthritic joint the cause of your arthritis or the consequence? Homocysteine is high in the sites of brain decay. It is, itself, capable of damaging neurons (brain cells). When there is an increase in P-tau and amyloid there is a corresponding increase in homocysteine.
To understand what homocysteine is read the article ‘The H factor’ but, in brief, there’s a vital process going on in your brain called ‘methylation’. If you’ve watched the 1 minute film ‘how to keep building brain cells’ you’ll know that the membrane of these neurons includes the omega-3 fatty acid DHA, enriched in fish, a component of phospholipids, . Formation of certain key phospholipids enriched in omega-3 fatty acids involves methylation. There’s a multitude of methylation reactions in your brain and body every few seconds. If you’re not doing methylation well your blood homocysteine goes up. Raised homocysteine, an indicator of disrupted methylation, is associated with raised neurofibilliary tangles (and p-tau) [5] and, to a lesser extent with raised amyloid proteins [5] [6]. Read the p-tau delusion for more on this marker for Alzheimer’s.
Methylation depends having enough of certain B vitamins in your bloodstream. Thus taking the right B vitamins in the right amounts lowers homocysteine (see The H Factor) and has been shown to reduce brain shrinkage in those with pre-dementia (mild cognitive impairment or MCI) by up to 73%.
So, while amyloid, found in over 90% of the brains of those with Alzheimer’s [7], as is homocysteine, can be used to help diagnose will lowering amyloid or p-tau help treat the disease? In terms of blood markers high homocysteine and low total cholesterol (below 4.1 mmol/l) were found to be the best predictors of dementia.[8] Cholesterol is an essential part of the structure of neuronal membranes. Statin (over) use is associated with cognitive dysfunction.
All amyloid protein lowering drugs have essentially failed
A number of studies showing amyloid in the brains of those with Alzheimer’s have helped spawn more than 300 trials of drugs to lower amyloid protein, at an estimated research cost of $42.5 billion [9] These amyloid-lowering drugs have been tested on an estimated 185,000 participants.
Back in 2021 the last hope was a drug called Aducanumab. In March 2019, when Biogen announced they were halting their Phase 3 clinical trial of the drug since it showed no benefit, the New York Times reported “An Alzheimer’s Treatment fails: we don’t have anything now. More than 300 failed trials. With high hopes, drugs to fight brain plaques were tested in people genetically destined to develop dementia. The drugs failed.” A British Medical Journal researcher got hold of the results of 14 trials of these drugs, given to a total of 4,596 patients, but found no significant effect on cognition despite lowering brain beta-amyloid levels. The true extent of the failure of these drugs is likely to be much worse but researchers attempting to pool all of 34 ‘phase 3’ clinical trials were denied access to 20 of them. [10]This is the same old story that has occurred with so many drugs, hiding the worst results to get the drug licensed to sell and to maximise profits.
However, is 2022, a similar drug, Lecanemab, managed to get a statistical difference in the Clinical Dementia Rating (CDR). [11] While statistically significant, the results were clinically meaningless – less than half a point drop in an 18 point Clinical Dementia Rating. Also, one in five got brain bleeding or swelling. According to Oxford University’s Professor Emeritus of Pharmacology, David Smith “The study is statistically convincing but clinically not significant. A mean difference of 0.45 in the CDR score would not be noticeable by the patient or carer in my view.” Both B vitamin and omega-3 studies have done much better than this both in reducing the CDR and improving other measures of cognition, and in reducing the rate of brain shrinkage. The rate of brain shrinkage reduction of this kind of drug is 2% compared to up to 73% less shrinkage with B vitamins in those with sufficient omega-3. [12] We believe this theory is a red herring. Targetting amyloid deposits in the brain is misguided.
High homocysteine and low cholesterol predict Alzheimer’s
The best blood test predictors for the risk of Alzheimer’s is not your level of amyloid but having a high homocysteine or a low cholesterol level, concludes a study of almost five thousand older people [9]. Having a homocysteine level above 11mcmol/l or a cholesterol level below 4mmol/l (155mg/dl in US measures) predicts risk. Of these homocysteine is the most important marker with twenty years of consistent evidence (read The H Factor report).
In the film ‘how to keep building brain cells’ you’ll see that those brain fats – omega 3 DHA and phospholipids – are effectively held in place by cholesterol. One quarter of all the cholesterol in your body is in your brain. So it should not be surprising that if a person is given cholesterol lowering drugs either at too high a dose or when their cholesterol level is normal, this can drive cholesterol levels too low, and this is associated with cognitive dysfunction. Too much or too little cholesterol in the blood is bad for you.
Unlike amyloid-lowering drugs homocysteine-lowering B vitamins have been shown to virtually stop any further memory shrinkage and, in those with sufficient omega-3 blood levels, reduce brain shrinkage by 73% [10], compared to 2% for the best amyloid drug, and in one trial after a year on B vitamins the pre-dementia participants with raised homocysteine levels, had a clinical dementia rating of zero. [read The H Factor report for the full story] So, why are B vitamins not being promoted? Being natural they can’t be patented. Without a patent there just isn’t the means to make sufficient profit for the pharmaceutical industry.
Why a drug cure is unlikely
Alzheimer’s, like those other ‘metabolic’ diseases of the 21st century – diabetes, cardiovascular disease and obesity– is primarily caused by sub-optimum nutrition and lifestyle. As such they are ‘foodable’ but not ‘drugable’. Diseases like diabetes, high blood pressure and arthritis can be ‘managed’ with medication but it makes sense to tackle the root cause of these problems.
While hypertension (high blood pressure) is a strong risk factor for Alzheimer’s, and having high blood pressure is bad news for the brain’s blood vessels and supply of nutrients (cerebrovascular dementia is the second most common form of dementia) will lowering it with medication reduce Alzheimer’s risk? Maybe – trials are under way.
Diabetes is also a risk factor for dementia. Medication for type-2 diabetes (metformin or insulin) help stabilise blood sugar, which helps reduce symptoms and complications, but it doesn’t reverse the disease. Does the medication reduce risk for dementia? Maybe – trials are under way. We will keep you informed.
Our advice is not to wait for a miracle drug around the corner but do something to change your nutrition and your lifestyle now. The exact same changes that reduce dementia risk also reduce risk for diabetes and cardiovascular disease. Don’t put all your eggs in the ‘drug’ basket, but do put eggs, fish, whole fresh food in your shopping basket, plus some B vitamins.
Alzheimer’s is not reversible but is preventable
Unlike type-2 diabetes, obesity and high blood pressure, which are potentially reversible, especially the earlier you start to make changes, Alzheimer’s dementia, which is two thirds of dementia diagnoses, is diagnosed by shrinkage in the central ‘hippocampal’ area of the brain because brain cells have died. This is not reversible. However, in older people without a dementia diagnosis, improving nutrition has been shown to promote healthier brain tissue in under 6 months.
That is why you would be a fool to wait until your cognitive function is going rapidly downhill and then make changes. In fact, subtle changes in cognition can be detected on a Cognitive Function Test often thirty years before a diagnosis. That is why we encourage you to check your cognitive function now, take action on those of the 8 domains where your risk is highest, and re-take your Cognitive Function Test every year to monitor how the changes you make are improving or preserving your cognitive function. Then you are in control and can dementia-proof your diet and lifestyle.
References
- Bekris LM, Yu CE, Bird TD, Tsuang DW. Genetics of Alzheimer disease. J Geriatr Psychiatry Neurol. 2010 Dec;23(4):213-27. doi: 10.1177/0891988710383571. PMID: 21045163; PMCID: PMC3044597.
- Heininger, K. (2000), A unifying hypothesis of Alzheimer’s disease. III. Risk factors. Hum. Psychopharmacol. Clin. Exp., 15: 1-70. https://doi.org/10.1002/(SICI)1099-1077(200001)15:1<1::AID-HUP153>3.0.CO;2-1
- Norwitz,N.G.;Saif,N.; Ariza, I.E.; Isaacson, R.S. Precision Nutrition for Alzheimer’s Prevention in ApoE4 Carriers. Nutrients 2021, 13, 1362. https://doi.org/10.3390/ nu13041362
- Ridge PG, Mukherjee S, Crane PK, Kauwe JS; Alzheimer’s Disease Genetics Consortium. Alzheimer’s disease: analyzing the missing heritability. PLoS One. 2013 Nov 7;8(11):e79771. doi: 10.1371/journal.pone.0079771. PMID: 24244562; PMCID: PMC3820606.
- Hooshmand B, Polvikoski T, Kivipelto M, Tanskanen M, Myllykangas L, Erkinjuntti T, Mäkelä M, Oinas M, Paetau A, Scheltens P, van Straaten EC, Sulkava R, Solomon A. Plasma homocysteine, Alzheimer and cerebrovascular pathology: a population-based autopsy study. Brain. 2013 Sep;136(Pt 9):2707-16. doi: 10.1093/brain/awt206. PMID: 23983028; PMCID: PMC3754457.
- Sontag JM, Sontag E. Protein phosphatase 2A dysfunction in Alzheimer’s disease. Front Mol Neurosci. 2014 Mar 11;7:16. doi: 10.3389/fnmol.2014.00016. PMID: 24653673; PMCID: PMC3949405.
- Schindler SE, Bollinger JG, Ovod V, Mawuenyega KG, Li Y, Gordon BA, Holtzman DM, Morris JC, Benzinger TLS, Xiong C, Fagan AM, Bateman RJ. High precision plasma amyloid-β 42/40 predicts current and future brain amyloidosis. Neurology, August 1, 2019 DOI:
- Gong Q, Xie L, Bi M, Yu L. A probability formula derived from serum indicators, age, and comorbidities as an early predictor of dementia in elderly Chinese people. Brain Behav. 2021 Aug;11(8):e2236. doi: 10.1002/brb3.2236. Epub 2021 Jun 26. PMID: 34173349; PMCID: PMC8413781.
- Cummings JL, Goldman DP, Simmons-Stern NR, Ponton E. The costs of developing treatments for Alzheimer’s disease: A retrospective exploration. Alzheimer’s Dement. 2022;18:469–477. https://doi.org/10.1002/alz.12450
- https://www.bmj.com/content/372/bmj.n156/rr
- van Dyck CH, Swanson CJ, Aisen P, Bateman RJ, Chen C, Gee M, Kanekiyo M, Li D, Reyderman L, Cohen S, Froelich L, Katayama S, Sabbagh M, Vellas B, Watson D, Dhadda S, Irizarry M, Kramer LD, Iwatsubo T. Lecanemab in Early Alzheimer’s Disease. N Engl J Med. 2023 Jan 5;388(1):9-21. doi: 10.1056/NEJMoa2212948. Epub 2022 Nov 29. PMID: 36449413.
- Jernerén F, Elshorbagy AK, Oulhaj A, Smith SM, Refsum H, Smith AD (2015). Brain atrophy in cognitively impaired elderly: the importance of long-chain ω-3 fatty acids and B vitamin status in a randomized controlled trial. Am J Clin Nutr. 2015 Jul;102(1):215-21
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices.
Please support our research by becoming a Friend of Food for the Brain.