The Attention Deficit Disaster: Managing ADHD in Adults
Attention-Deficit Hyperactivity Disorder (ADHD) is not just an issue to address with our children. Many adults are finding themselves diagnosed with this brain disorder and conventional medicinal support is limited.
Why are we struggling to focus and concentrate OR focus on one specific task at a cost to our health, relationships and other essential life activities (known as hyperfocus)?
We can see how this, if not managed, can be problematic for children and the impact it can have on their learning and confidence but what if you are an adult who has recently realised that your brain works and struggles differently to those around you? (If you are interested in supporting your child’s brain then join our Smart Kids & Teens programme here.)
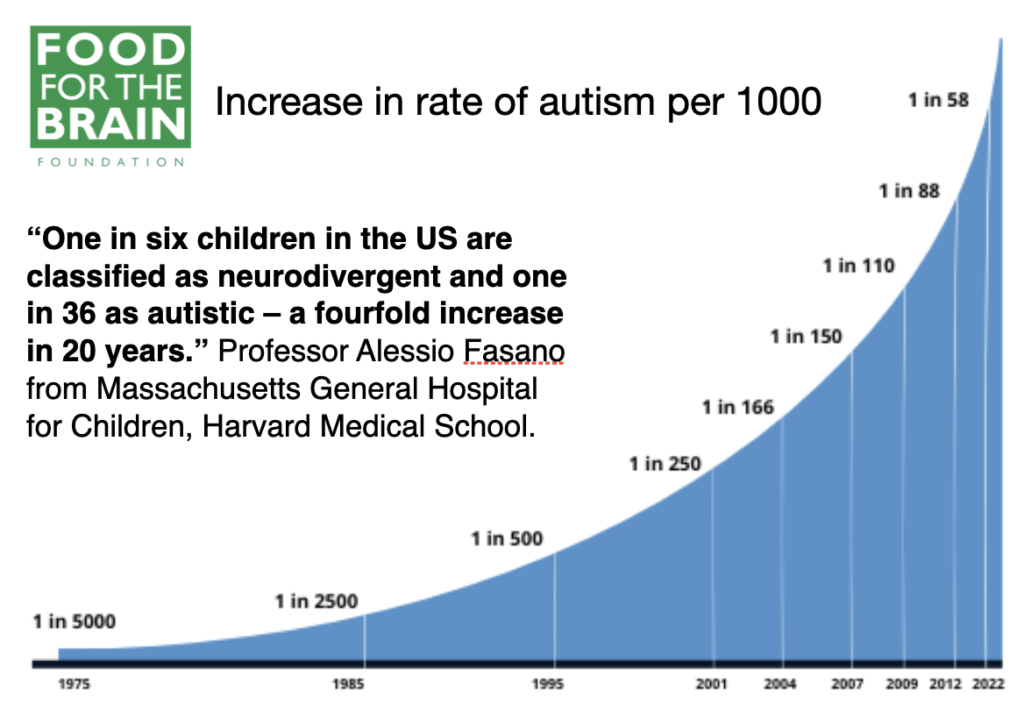
The incidence of neurodevelopmental disorders like Attention-Deficit Hyperactivity Disorder (ADHD) and Autism Spectrum Disorder (ASD) has surged in recent years and both are classified as neurodivergent conditions (along with other conditions like learning disabilities, attention-deficit and anxiety disorders, obsessive-compulsive disorder and Tourette’s syndrome).
In the UK and the USA, the rise in diagnoses has been significant, prompting questions about underlying causes and potential solutions. While there may be a familial aspect, we know ‘it is not in the genes’. So, why are we facing this attention deficit disaster?
—
The Attention Deficit Disaster in Adults
ADHD is not confined to childhood; many adults continue to experience its symptoms, which can significantly impact their personal and professional lives. Also, many parents discover this about themselves as they go through the process of getting their child diagnosed.
Common symptoms of adult ADHD include:
- Inattention: difficulty sustaining attention during tasks, making careless mistakes, not listening when spoken to directly, and being easily distracted (1,2).
- Hyperfocus: paradoxically, some adults with ADHD can become intensely focused on tasks they find stimulating or rewarding, often to the exclusion of other activities (3).
- Disorganisation: chronic issues with organising tasks and activities, often leading to missed deadlines and forgotten appointments (4).
- Time Management Problems: struggling to manage time effectively, leading to procrastination and difficulty completing tasks (5).
- Impulsivity: making hasty decisions without considering the long-term consequences, interrupting others, and difficulty waiting for their turn (6).
- Emotional Dysregulation: experiencing intense emotions, such as frustration or anger, and difficulty managing stress (7,8).
—
It looks different for men and women…
ADHD can present differently in men and women, which often leads to underdiagnosis or misdiagnosis in women. Here are some key differences:
- Inattention vs. Hyperactivity: women are more likely to exhibit inattentive symptoms, such as disorganisation, forgetfulness, and difficulty focusing. In contrast, men often display more hyperactive and impulsive behaviours, like restlessness and acting without thinking (9,10).
- Emotional Symptoms: women with ADHD may experience higher levels of emotional dysregulation, including mood swings, anxiety, and depression. Men are more likely to exhibit externalising behaviours, such as aggression and conduct problems (11,12).
- Coping Mechanisms: women tend to develop coping strategies that mask their symptoms, such as becoming perfectionists or overworking to compensate for their inattentiveness. This can delay diagnosis and treatment (13).
- Social Consequences: women with ADHD often face significant social consequences, including challenges in maintaining relationships and social isolation. Men, however, may struggle more with academic and behavioural issues in school settings (14,15).
—
Start at the very beginning of brain development…
The adult brain begins at conception, making maternal nutrition crucial.
As well as avoiding alcohol and smoking during pregnancy we know from a study of 11,875 pregnant women there is a clear relationship between the amount of seafood consumed by a pregnant woman and their child’s development. The less seafood consumed, the worse the child’s social behaviour, fine motor skills, communication and social development, and verbal IQ. (16)
In addition, a lack of vitamin A during pregnancy, another nutrient rich in seafood, can affect brain development and lead to long-term or even permanent impairment in the learning process, memory formation, and cognitive function. (17)
Plus, there is folic acid. A mother’s folate intake predicts the child’s performance in cognitive tests at the age of nine to ten (18) and the higher a baby’s B-vitamin status, the higher their cognitive function at the age of 25. (19) Supplementing mothers-to-be with folic acid (400mcg/day) during the second and third trimesters of pregnancy is associated with better cognition in their children at the age of three and better word reasoning and IQ (verbal and performance) at seven.(20)
Nothing can be built properly in the brain without healthy methylation and methylation requires folate (which is reflected by a low homocysteine level). Raised homocysteine is a well-known predictor of miscarriage and pregnancy problems, which is why we recommend that no woman attempts pregnancy until her homocysteine level is below 7 mcmol/l.
While we have learned that a homocysteine level above 11 means increased brain shrinkage, even a homocysteine level of above 9 during pregnancy predicts more problems, specifically withdrawn behaviour, anxiety, depression, social problems and aggressive behaviour in the child at the age of six. (21)
So looking back at your childhood development might help you to understand your adult brain. How well nourished was it? Did you get adequate folate, vitamin A and consume seafoods as a child?
Our hope is some of the deficit in brain function can be recovered by providing all brain-dependent nutrients at an optimal level and see what happens.
What would happen if you started to eat more fish and seafood? Here is some of the science:
- Lower DHA concentrations are associated with poorer reading ability, poorer memory, oppositional behaviour and emotional instability. (22)
- Several studies have shown increased aggression in those with low omega-3 DHA and EPA, and giving more omega-3 reduces aggression.(23)
- Improved IQ and sleep quality: a study of 541 Chinese schoolchildren found that fish consumption predicted sleep quality and that those who ate the most fish had the highest IQ – 4.8 points higher than those who ate none. Improved sleep quality, linked to fish intake, was correlated with IQ. (24)
—
Other Essential Nutrients for Brain Health
The brain needs nourishing, especially in childhood as it is growing and developing rapidly, but also as adults.
Here are some of the essential nutrients you may want to focus on to optimise your brain:
Vitamin A: can affect brain development and lead to long-term or even permanent impairment in the learning process, memory formation, and cognitive function. (17)
Vitamin D: low vitamin D levels in childhood are related to behaviour problems in adolescence (25) and are significantly linked to a higher risk of dementia and cognitive decline. (26, 27, 28)
Chromium, copper, zinc, and magnesium: children with ADHD tend to have lower levels of zinc, chromium, and magnesium, with some having low levels of copper (29). One study found a higher copper to zinc ratio in neurodivergent children compared to neurotypical children, predicting the degree of ADHD (30). Zinc supplementation has been shown to improve memory and attention spans in ADHD (31). Additionally, magnesium deficiency is common in ADHD, and supplementation has been linked to reduced hyperactivity (32). Deficiencies in these minerals can contribute to symptoms of ADHD and other neurodevelopmental disorders.
So are we Neurodivergent or Neurodeficient?
In the chart below are the most common characteristics in those with autistic spectrum disorder by the US Center for Disease Control and Prevention
I’ve added a column for the nutrients, when deficient, that have been shown to induce these symptoms.
| COMMON ASD CHARACTERISTICS | ASSOCIATED DEFICIENCY |
| Avoids eye contact | Vitamin A, Omega-3 DHA |
| Delayed language skills | Omega-3 DHA, Hcy/B vitamins, vitamin A |
| Delayed movement skills | Omega-3 DHA, Hcy/B vitamins, vitamin A |
| Delayed cognitive or learning skills | Omega-3 DHA, Hcy/B vitamins, vitamin A |
| Hyperactive, impulsive, and/or inattentive behaviour | Omega-3 DHA, Hcy/B vitamins, dysglycemia (sugar), additives eg MSG) |
| Epilepsy or seizure disorder | Omega-3 DHA, Hcy/B vitamins, dysglycemia (sugar), magnesium |
| Unusual eating and sleeping habits | Food intolerance, sugar, magnesium, zinc, tryptophan, |
| Gastrointestinal issues (for example, constipation) | Food intolerance (eg coeliacs), gut dysbiosis, zinc |
| Unusual mood or emotional reactions | Omega-3 DHA, Hcy/B vitamins, dysglycemia (sugar), additives eg MSG), food intolerance, iron |
| Anxiety, stress, or excessive worry | Omega-3 DHA, Hcy/B vitamins, dysglycemia (sugar), vitamin C |
| Lack of fear or more fear than expected | Omega-3 DHA, Hcy/B vitamins, dysglycemia (sugar), vitamin C |
—
—
Ending your sweet tooth…
It’s not just about specific nutrients, the amount of sugar you consume has a big impact on your brain health.
Too many carbs and ultra-processed foods are bad for anyone at any age, as is too much sugar. They are linked to children’s mental health issues relating to symptoms of ADHD (33) and autism and adult anxiety and depression, (34) and strongly linked to increased risk of age-related cognitive decline, dementia and Alzheimer’s.
Going back to childhood, even the glycemic load of a mother’s diet predicts a massive four-fold risk of anxiety in toddlers, with five times more impulsivity in boys, and four times as many sleeping problems, while girls have 15 times the likelihood of anxiety in those in the top third for glycemic load. (35)
So while you probably already know it, reducing sugar is imperative to your brain health.

—
Gut health & food intolerances
Dr Alessio Fasano, who is both Professor of Paediatrics at Harvard Medical School and Professor of Nutrition at Harvard’s Chan School of Public Health, thinks something is going wrong in the gut, with many ASD children reporting gut problems, including diarrhoea, constipation, belching and excessive flatulence and dysbiosis indicated by an abnormal pattern of gut bacteria. (36)
Professor Fasano’s research finds that neurodivergent guts show high levels of zonulin, which can lead to leaky gut. (37) The gluten in wheat makes the zonulin levels go up.
Opioid-like wheat and milk proteins have been found in the urine samples of those with ASD, making these foods especially ‘addictive’. This was the discovery of researchers at the Autism Research Unit at the University of Sunderland, headed by Paul Shattock, now known as ESPA Research. They developed successful strategies for helping children with autism known as the Sunderland Protocol. (38)
—
The four drivers of ADHD
Optimum nutrition has a big role to play in helping ameliorate negative symptoms of neurodivergence.
Multi-nutrient trials have shown improvements in irritability, hyperactivity and self-harm in children with ADHD.(39) Raised homocysteine and low B12 or folate are associated with greater risk of developing ASD and worse symptoms, (40) creating methylation abnormalities that could explain many of the symptoms. (41) Supplementing homocysteine-lowering B vitamins makes symptoms better. (42)
So to summarise conditions like ADHD may be made worse or contributed to by:
- A high-GL diet, with too much sugar
- A lack of essential omega-3 fats
- A lack of critical nutrients such as B vitamins, zinc and magnesium
- Unidentified food intolerances (read more about how food intolerance can impact the brain here)
—
What you can do
For adults managing ADHD, a holistic approach that incorporates dietary changes and supplementation can be highly effective. Here are some strategies:
- Feed your brain! The food you eat provides the ‘raw material’ for your brain and body. Focus on a diet rich in whole foods, including 3-5 portions of oily fish a week, nuts, seeds, leafy greens, and vegetables, to ensure adequate intake of essential nutrients.
- Add in key nutrients. Consider supplementing with B-vitamins, zinc, magnesium, copper, chromium, and other essential nutrients to address deficiencies and support optimal brain function. Find out more about recommended supplements and dose requirements here
- Test don’t guess. Test your vitamin D, omega-3, and sugar levels, along with your homocysteine, to get accurate data on what you need to focus on or supplement with. Find out more about the accurate, at-home tests here
- Mindful Eating. Pay attention to food intolerances and adopt a low-glycemic load (low sugar) diet to stabilise blood sugar levels and improve cognitive function.
- Complete the Cognitive Function test below to get personalised information on your area of risk and what you can do to mitigate them and upgrade your brain over the next 6 months..
- Reclaim your brain so that your neurodivergence can serve and support you, and no longer create additional struggle in your life.
Thank you for reading!
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices.
Please support our research by becoming a Friend of Food for the Brain.
References
1 Barkley RA. Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. New York: Guilford Press; 2010.
2 Kooij JJS, Bejerot S, Blackwell A, et al. European consensus statement on diagnosis and treatment of adult ADHD: The European Network Adult ADHD. BMC Psychiatry. 2010;10(1):67.
3 Asherson P, et al. Attention deficit hyperactivity disorder in adults: A review of the literature. Nat Rev Neurol. 2012;8(2):93-104.
4 Brown TE. Attention Deficit Disorder: The Unfocused Mind in Children and Adults. New Haven: Yale University Press; 2005.
5 Faraone SV, Biederman J, Mick E. The age-dependent decline of ADHD: A meta-analysis of follow-up studies. Psychol Med. 2006;36(2):159-165.
6 Willcutt EG, et al. Validity of DSM-IV attention deficit/hyperactivity disorder symptom dimensions and subtypes. J Abnorm Psychol. 2012;121(4):991.
7 Shaw P, et al. Emotion dysregulation in attention deficit hyperactivity disorder. Am J Psychiatry. 2014;171(3):276-293.
8 Surman CB, et al. Emotional dysregulation in adult ADHD and response to atomoxetine. J Atten Disord. 2011;15(5):354-368.
9 Quinn PO, Madhoo M. A review of attention-deficit/hyperactivity disorder in women and girls: Uncovering this hidden diagnosis. Prim Care Companion CNS Disord. 2014;16(3):PCC.13r01596.
10. Williamson D, Johnston C. Gender differences in adults with attention-deficit/hyperactivity disorder: A narrative review. Clin Psychol Rev. 2015;40:15-27.
11.Loo SK, et al. Cognition in girls with attention-deficit/hyperactivity disorder: Executive functions, emotion regulation, and comorbidity. J Am Acad Child Adolesc Psychiatry. 2008;47(3):262-274.
12 Babinski DE, et al. A meta-analysis of neuropsychological functioning in posttraumatic stress disorder. Arch Clin Neuropsychol. 2015;30(8):724-743.
13 Skogli EW, et al. Emotional lability in children and adolescents with attention deficit/hyperactivity disorder (ADHD): Clinical correlates and familial prevalence. J Affect Disord. 2013;145(2):241-249.
14 Grevet EH, et al. Gender differences in prevalence of symptoms of attention deficit and hyperactivity disorder in adults. Rev Bras Psiquiatr. 2005;27(1):21-24.
15 Solanto MV, et al. The prevalence of sluggish cognitive tempo in psychiatric outpatients with ADHD, anxiety, and mood disorders. J Atten Disord. 2017;21(8):666-674.
16 Hibbeln JR, Davis JM,] Steer C, Emmett P, Rogers I, Williams C, Golding J. Maternal seafood consumption in pregnancy and neurodevelopmental outcomes in childhood (ALSPAC study): an observational cohort study. Lancet. 2007 Feb 17;369(9561):578-85. doi: 10.1016/S0140-6736(07)60277-3. PMID: 17307104.
17 Z.Liu Behav Neurol. 2021 Dec 7;2021:5417497
18 Veena SR, Krishnaveni GV, Srinivasan K, Wills AK, Muthayya S, Kurpad AV, Yajnik CS, Fall CH. Higher maternal plasma folate but not vitamin B-12 concentrations during pregnancy are associated with better cognitive function scores in 9- to 10- year-old children in South India. J Nutr. 2010 May;140(5):1014-22. doi: 10.3945/jn.109.118075. Epub 2010 Mar 24. PMID: 20335637; PMCID: PMC3672847.
19. Qin B, Xun P, Jacobs DR Jr, Zhu N, Daviglus ML, Reis JP, Steffen LM, Van Horn L, Sidney S, He K. Intake of niacin, folate, vitamin B-6, and vitamin B-12 through young adulthood and cognitive function in midlife: the Coronary Artery Risk Development in Young Adults (CARDIA) study. Am J Clin Nutr. 2017 Oct;106(4):1032-1040. doi: 10.3945/ajcn.117.157834. Epub 2017 Aug 2. PMID: 28768650; PMCID: PMC5611785.
20 McNulty H, Rollins M, Cassidy T, Caffrey A, Marshall B, Dornan J, McLaughlin M, McNulty BA, Ward M, Strain JJ, Molloy AM, Lees-Murdock DJ, Walsh CP, Pentieva K. Effect of continued folic acid supplementation beyond the first trimester of pregnancy on cognitive performance in the child: a follow-up study from a randomized controlled trial (FASSTT Offspring Trial). BMC Med. 2019 Oct 31;17(1):196. doi: 10.1186/s12916-019-1432-4. PMID: 31672132; PMCID: PMC6823954.
21 Roigé-Castellví J, Murphy M, Fernández-Ballart J, Canals J. Moderately elevated preconception fasting plasma total homocysteine is a risk factor for psychological problems in childhood. Public Health Nutr. 2019 Jun;22(9):1615-1623. doi: 10.1017/S1368980018003610. Epub 2019 Jan 14. PMID: 30636652; PMCID: PMC10261079.
22 Montgomery P, Burton JR, Sewell RP, Spreckelsen TF, Richardson AJ. Low blood long chain omega-3 fatty acids in UK children are associated with poor cognitive performance and behavior: a cross-sectional analysis from the DOLAB study. PLoS One. 2013 Jun 24;8(6):e66697. doi: 10.1371/journal.pone.0066697. Erratum in: PLoS One. 2013;8(9). doi:10.1371/annotation/26c6b13f-b83a-4a3f-978a-c09d8ccf1ae2. PMID: 23826114; PMCID: PMC3691187.
23 Raine A, Ang RP, Choy O, Hibbeln JR, Ho RM, Lim CG, Lim-Ashworth NSJ, Ling S, Liu JCJ, Ooi YP, Tan YR, Fung DSS. Omega-3 (ω-3) and social skills interventions for reactive aggression and childhood externalizing behavior problems: a randomized, stratified, double-blind, placebo-controlled, factorial trial. Psychol Med. 2019 Jan;49(2):335-344. doi: 10.1017/S0033291718000983. Epub 2018 May 10. PMID: 29743128; see also Choy O, Raine A. Omega-3 Supplementation as a Dietary Intervention to Reduce Aggressive and Antisocial Behavior. Curr Psychiatry Rep. 2018 Apr 5;20(5):32. doi: 10.1007/s11920-018-0894-y. PMID: 29623453; see also Gow RV, Hibbeln JR. Omega-3 fatty acid and nutrient deficits in adverse neurodevelopment and childhood behaviors. Child Adolesc Psychiatr Clin N Am. 2014 Jul;23(3):555-90. doi: 10.1016/j.chc.2014.02.002. Epub 2014 May 27. PMID: 24975625; PMCID: PMC4175558.
24 Liu, J., Cui, Y., Li, L. et al. The mediating role of sleep in the fish consumption – cognitive functioning relationship: a cohort study. Sci Rep 7, 17961 (2017). https://doi.org/10.1038/s41598-017-17520-w
25 Sonia L Robinson, Constanza Marín, Henry Oliveros, Mercedes Mora-Plazas, Betsy Lozoff, Eduardo Villamor, Vitamin D Deficiency in Middle Childhood Is Related to Behavior Problems in Adolescence, The Journal of Nutrition, Volume 150, Issue 1, 2020, pp.140–148, ISSN 0022-3166, https://doi.org/10.1093/jn/nxz185.
26 Jayedi A, Rashidy-Pour A, Shab-Bidar S. Vitamin D status and risk of dementia and Alzheimer’s disease: A dose-response meta-analysis. Nutr Neurosci. 2019 Nov;22(11):750-9. doi: 10.1080/1028415X.2018.1436639.
27 Chai B, Gao F, Wu R, Dong T, Gu C, Lin Q, et al. Vitamin D deficiency as a risk factor for dementia and Alzheimer’s disease: an updated meta-analysis. BMC Neurol. 2019 Nov 13;19(1):284. doi: 10.1186/s12883-019-1500-6.
28 Melo van Lent D, Egert S, Wolfsgruber S, Kleineidam L, Weinhold L, Wagner-Thelen H, et al. Low Serum Vitamin D Status Is Associated with Incident Alzheimer’s Dementia in the Oldest Old. Nutrients. 2023;15(1):61. https://doi.org/10.3390/nu15010061
29 Skalny AV, Mazaletskaya AL, Ajsuvakova OP, Bjørklund G, Skalnaya MG, Chao JC, Chernova LN, Shakieva RA, Kopylov PY, Skalny AA, Tinkov AA. Serum zinc, copper, zinc-to-copper ratio, and other essential elements and minerals in children with attention deficit/hyperactivity disorder (ADHD). J Trace Elem Med Biol. 2020 Mar;58:126445. doi: 10.1016/j.jtemb.2019.126445. PMID: 31869738.
30 This has not been observed in New Zealand; see: https://pubmed.ncbi.nlm.nih.gov/30217770/.
31 Hemamy M, Pahlavani N, Amanollahi A, Islam SMS, McVicar J, Askari G, Malekahmadi M. The effect of vitamin D and magnesium supplementation on the mental health status of attention-deficit hyperactive children: a randomized controlled trial. BMC Pediatr. 2021 Apr 17;21(1):178. doi: 10.1186/s12887-021-02631-1. Erratum in: BMC Pediatr. 2021 May 12;21(1):230. PMID: 33865361; PMCID: PMC8052751.
32 B. Starobrat-Hermelin and T. Kozielec, ‘The effects of magnesium physiological supplementation on hyperactivity in children with attention deficit hyperactivity disorder (ADHD): Positive response to magnesium oral loading test’, Magnes Res, Vol 10(2), 1997, pp. 149-56
33 Farsad-Naeimi A, Asjodi F, Omidian M, Askari M, Nouri M, Pizarro AB, Daneshzad E. Sugar consumption, sugar sweetened beverages and Attention Deficit Hyperactivity Disorder: A systematic review and meta-analysis. Complement Ther Med. 2020 Sep;53:102512. doi: 10.1016/j.ctim.2020.102512. Epub 2020 Aug 16. PMID: 33066852.
34 Haghighatdoost F, Azadbakht L, Keshteli AH, Feinle-Bisset C, Daghaghzadeh H, Afshar H, Feizi A, Esmaillzadeh A, Adibi P. Glycemic index, glycemic load, and common psychological disorders. Am J Clin Nutr. 2016 Jan;103(1):201-9. doi: 10.3945/ajcn.114.105445. Epub 2015 Nov 25. PMID: 26607943.
35 Alick CL, Maguire RL, Murphy SK, Fuemmeler BF, Hoyo C, House JS. Periconceptional Maternal Diet Characterized by High Glycemic Loading Is Associated with Offspring Behavior in NEST. Nutrients. 2021 Sep 13;13(9):3180. doi: 10.3390/nu13093180. PMID: 34579057; PMCID: PMC8469715.
36 Needham BD, Adame MD, Serena G, Rose DR, Preston GM, Conrad MC, Campbell AS, Donabedian DH, Fasano A, Ashwood P, Mazmanian SK. Plasma and Fecal Metabolite Profiles in Autism Spectrum Disorder. Biol Psychiatry. 2021 Mar 1;89(5):451-462. doi: 10.1016/j.biopsych.2020.09.025. Epub 2020 Oct 10. PMID: 33342544; PMCID: PMC7867605.
37 Asbjornsdottir, Birna, et al. “Zonulin-dependent intestinal permeability in children diagnosed with mental disorders: a systematic review and meta-analysis.” Nutrients 12.7 (2020): 1982.
39 Mehl-Madrona L. Journal of Alternative and Complementary Medicine 2017 , 23(7), 526–533.
40 Li B, Xu Y, Pang D, Zhao Q, Zhang L, Li M, Li W, Duan G, Zhu C. Interrelation between homocysteine metabolism and the development of autism spectrum disorder in children. Front Mol Neurosci. 2022 Aug 15;15:947513. doi: 10.3389/fnmol.2022.947513. PMID: 36046711; PMCID: PMC9421079.
41 Antonio Belardo, Federica Gevi, Lello Zolla, The concomitant lower concentrations of vitamins B6, B9 and B12 may cause methylation deficiency in autistic children, The Journal of Nutritional Biochemistry, Volume 70, 2019, Pages 38-46, ISSN 0955-2863, https://doi.org/10.1016/j.jnutbio.2019.04.004; see also James SJ, Melnyk S, Fuchs G, Reid T, Jernigan S, Pavliv O, Hubanks A, Gaylor DW. Efficacy of methylcobalamin and folinic acid treatment on glutathione redox status in children with autism. Am J Clin Nutr. 2009 Jan;89(1):425-30. doi: 10.3945/ajcn.2008.26615. Epub 2008 Dec 3. PMID: 19056591; PMCID: PMC2647708.
42 Rossignol DA, Frye RE. The Effectiveness of Cobalamin (B12) Treatment for Autism Spectrum Disorder: A Systematic Review and Meta-Analysis. J Pers Med. 2021 Aug 11;11(8):784. doi: 10.3390/jpm11080784. PMID: 34442428; PMCID: PMC8400809; see also ref xx below; Adams JB, Audhya T, Geis E, Gehn E, Fimbres V, Pollard EL, Mitchell J, Ingram J, Hellmers R, Laake D, Matthews JS, Li K, Naviaux JC, Naviaux RK, Adams RL, Coleman DM, Quig DW. Comprehensive Nutritional and Dietary Intervention for Autism Spectrum Disorder-A Randomized, Controlled 12-Month Trial. Nutrients. 2018 Mar 17;10(3):369. doi: 10.3390/nu10030369. PMID: 29562612; PMCID: PMC5872787; see also James SJ, Melnyk S, Fuchs G, Reid T, Jernigan S, Pavliv O, Hubanks A, Gaylor DW. Efficacy of methylcobalamin and folinic acid treatment on glutathione redox status in children with autism. Am J Clin Nutr. 2009 Jan;89(1):425-30. doi: 10.3945/ajcn.2008.26615. Epub 2008 Dec 3. PMID: 19056591; PMCID: PMC2647708.