The Antioxidant Edge: Measuring and Protecting Your Brain’s Resilience Against Ageing
(Originally posted in IHCAN magazine. Written by Patrick Holford, edited by Carol Ludlam)

What is really going on as we age? What contributes to the wrinkles, stiffer joints, slower cognitive function and other health problems?
It begins with the brain.
Your brain consumes more energy than any other organ, burning either glucose or ketones. This combustion creates oxidants that age your brain. The ability to rapidly extinguish these oxidants, which ultimately age your brain and body, is what helps you live longer with less wrinkles, more flexible joints, healthier blood vessels and organs, especially your brain, which has 400 miles of blood vessels.
—
Top level prevention factors
Keeping oxidants down is perhaps the single most important thing you can do for vascular health. Vascular dementia, for example, is strongly associated with the amount of oxidation, determined by antioxidant intake from fruit and vegetables on the one side and smoking and pollution for example, on the other. Those in the top quarter of Total Antioxidant Capacity (TAC) in their diet halve their risk, in a study of 2,716 people over age 60 (1).
Additionally, critical antioxidants such as vitamin C and vitamin E, if supplemented together, reduced the risk of developing Alzheimer’s by as much as two-thirds, whilst taking either cut risk by a quarter in a study of 4,740 elderly residents of Cache County, Utah (2). Another study shows that ‘either a high vitamin E or C intake showed a trend of attenuating risk by about 26 per cent’, according to China’s leading prevention expert Professor Jin Tai Yu of Fudan University in Shanghai, making these nutrients ‘grade 1’ top level prevention factors (3).
Vitamin C, which is water based and protects you against smoke and pollution, and vitamin E, which is fat based and protects you from burnt and fried fats, including sunburn, are in the bloodstream outside of cells. Inside cells, especially brain cells, is the most potent antioxidant of all, which is glutathione.
—
Glutathione is the Master Intracellular Antioxidant
Nutritionists have been measuring red cell glutathione (GSH) for decades as an indicator of a person’s antioxidant capacity. GSH is the most important antioxidant and free radical scavenger that is found to be decreased in the brains of people with a wide range of mental and neurological illnesses from schizophrenia (4) to dementia (5, 6).
However, the problem with just measuring glutathione is two-fold. Firstly, since it oxidises so rapidly, it has to be ‘fixed’ immediately to avoid any degradation to its oxidised form glutathione disulfide (GSSG). Testing of glutathione levels is therefore usually dependent on going to a lab for blood to be drawn and then immediately tested or fixed, to limit any oxidation. The reliability of glutathione measurements, unless done under strictly controlled conditions such as these, may be questionable due to the rapid oxidation once blood is taken.
—
The Glutathione Index (GSH/GSSG) is the best measure of antioxidant status
Additionally, it is the amount of ‘spent’ or oxidised glutathione (GSSG) that reflects the extent of oxidative stress a person is under. Think of glutathione as the water in the fire engine. It gets rapidly used up keeping your brain protected. The ‘spent’ or oxidised glutathione (GSSG), much like steam, then has to be cooled to reload the fire engine. This recycling is done by vitamin C and an enzyme called Glutathione Reductase (GR), returning Glutathione back to its fully loaded ‘reduced’ form. Another enzyme, Glutathione Peroxidase (GP), is involved. GR is riboflavin (vitamin B2) dependent and GP is selenium dependent.

Dr Konrad Kowalski, the Food for the Brain’s analytic chemist, explains: “Reductions in GR enzyme levels in patients with dementia are well established. GR levels alone are therefore a fairly good biomarker of dementia.” However, the mere presence of the enzyme does not guarantee its high activity. GR needs to consume NADP molecules to function properly. As shown by Irene Martinez de Toda et al 2019 data, patients with dementia have a reduction in both the enzymes (GR and GP) that recycle glutathione. Thus, in general it can be said that the glutathione metabolism (recycling) loop in those with dementia ‘spins’ much slower than in healthy patients.
“The advantage of our measurement of the Glutathione Index (GSH/GSSG) is therefore, that it shows changes in GR activity, not only due to higher/lower GR gene activity but also due to the absence of the reaction cofactor NADP.”
“As a result, dementia patients have a lower potential to dynamically fight free radicals and will have a worse GSH/GSSG, which we call the Glutathione Index (7). The worse the ratio the worse a person’s cognitive function is likely to be. It’s a bit like having a direct measure of how fast your brain is ageing. Patients with dementia have a reduction in glutathione and its ability to be recycled (8). This ratio, the Glutathione Index, is a biomarker for many diseases, including both type 1 and 2 diabetes, liver cirrhosis, multiple sclerosis and Alzheimer’s disease.” says Dr Konrad Kowalski, who has developed this test for us.
One of the biggest challenges in developing the Glutathione Index, which is a home test kit involving a pin prick of blood dripped onto a dry blood spot card, is that the conventional DBS cards didn’t provide enough stability for the rapidly oxidising GSH, so we developed a method that instantly ‘fixes’ the sample for a guaranteed 12 week stability from taking the sample.
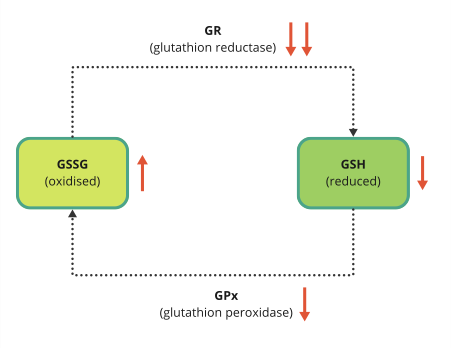
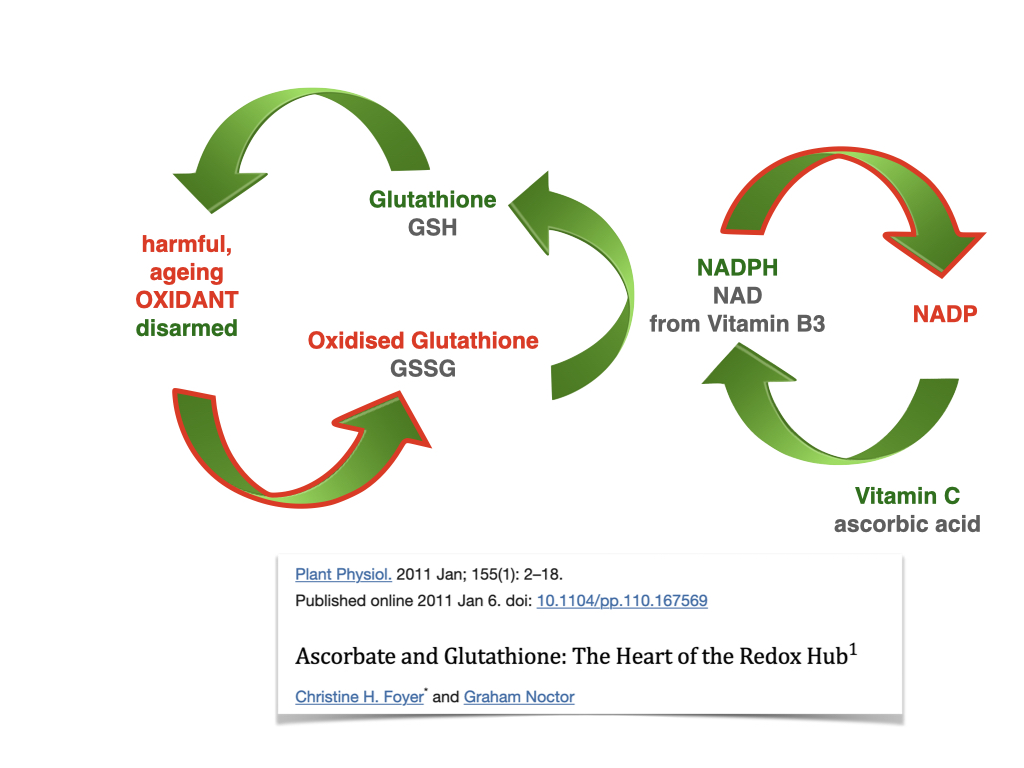
The red arrows indicate reduced or increased activity in dementia patients
So we want people to both measure their Glutathione Index and complete our validated Cognitive Function Test along with the follow-on Dementia Risk Index questionnaire, which calculates an ‘antioxidant’ domain score.
As a result of our research where we have tracked these against the person’s blood level of Glutathione Index, enabling us to establish what an optimal level is. This means those boundaries, which we show in colours from green (good), yellow (OK), orange (not good), red (bad) will evolve and become more accurate thanks to you and people like you.
We now know that a desirable level is above 800. Below 500 is an indicator that you need to increase your intake of antioxidants from food and/or supplements, and/or reduce your intake of oxidants from smoking, pollution or fried food. Glutathione is related to the pace of aging and the activity of antioxidant enzymes which are depleted in those with cognition decline. It is also part of your DRIfT (Dementia Risk Index functional Test) score.
This is unique and vital research funded by the people for the people – Citizen Scientists.
—

—
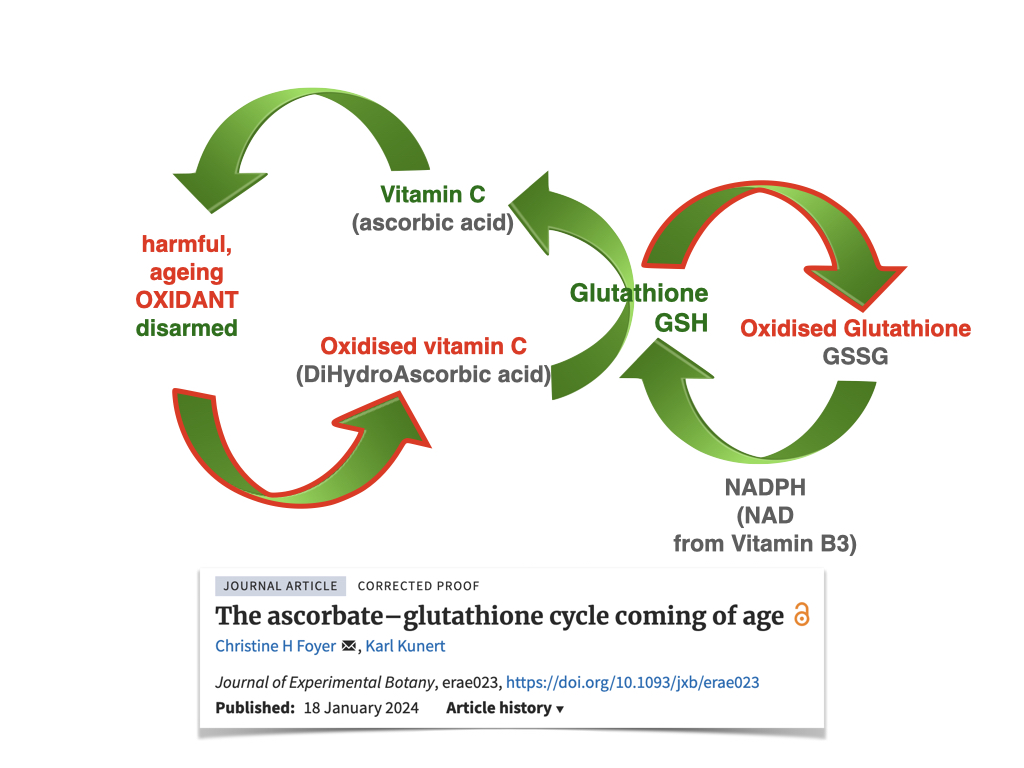
How Glutathione and vitamin C recycle each other
Vitamin C helps ‘reload’ glutathione and glutathione helps reload vitamin C as you’ll see in the figures below. This glutathione – vitamin C cycle is one of the hottest discoveries in anti-ageing science. You’ll see that NADPH, derived from niacin (vitamin B3) and its cousin NAD are involved. Co-enzyme Q10 in its reduced form ubiquinol is also involved and although not shown in this diagram, low levels are also found in those with Alzheimer’s (9).
—
Raising glutathione – the role of NAC
Nutritional therapists have been measuring red cell glutathione and supplementing glutathione or its precursor N-Acetyl-Cysteine (NAC) for decades. However oral GSH supplementation has poor bioavailability largely because it is so rapidly oxidised to GSSG as it disarms free radicals. N-Acetyl Cysteine (NAC), a precursor of glutathione, is therefore often used instead and has been shown to successfully raise plasma glutathione levels, for example, in those with schizophrenia. Anthocyanins also recycle glutathione thus sparing it if supplemented together (12).
NAC has plenty of evidence to support its use as a promoter of glutathione and mental health, thus reducing the brain’s oxidative stress. The latest 2022 review states: “N-acetyl-L-cysteine (NAC) is a compound of increasing interest in the treatment of psychiatric disorders. Primarily through its antioxidant, anti-inflammatory, and glutamate modulation activity, NAC has been investigated in the treatment of neurodevelopmental disorders, schizophrenia spectrum disorders, bipolar-related disorders, depressive disorders, anxiety disorders, obsessive compulsive-related disorders, substance-use disorders, neurocognitive disorders, and chronic pain. Currently NAC has the most evidence of having a beneficial effect as an adjuvant agent in the negative symptoms of schizophrenia, severe autism, depression, and obsessive compulsive and related disorders.” (13) For example a large RCT of 140 participants observed significant improvements on global symptomatology, and general and negative symptoms of schizophrenia in the NAC supplementation (2 g/d; in addition to anti-psychotic medication) group in comparison to the placebo group over a 24 week period (14).
According to Dr Chris Palmer, assistant professor at Harvard Medical School, “Glutathione (GSH), the brain’s primary antioxidant, plays a crucial role in maintaining redox balance (the process of maintaining the balance of reactive oxygen and nitrogen species in cells to maintain homeostasis) . Magnetic resonance studies have provided mixed results regarding GSH levels in schizophrenia patients, with some studies indicating decreased levels in chronic schizophrenia, while others found no significant differences. However, these inconsistencies may be due to variations in disease chronicity, age, and symptom severity among study participants. The findings from these studies suggest several potential therapeutic targets for schizophrenia. Addressing mitochondrial dysfunction, redox imbalance, and impaired energy metabolism could lead to more effective treatments. For instance, N-acetylcysteine (NAC), a precursor to GSH, has shown promise in increasing brain GSH levels and improving symptoms in first episode psychosis patients.”
NAC is so medically effective that it has been classified a medicine, hence not a food, and is no longer available over the counter in the US.
Our Glutathione Index test costs £69 – order it and be a part of this new exciting research, whilst learning how you can protect and upgrade your brain.
It is also available as part of their 5-in-1 DRIfT test also measuring Homocysteine, HbA1c, vitamin D and Omega-3 Index.
—
Actions
- Join COGNITION by becoming a FRIEND to get access to a personalised 6-month program to upgrade your brain
- Join our research and order the single Glutathione test OR the 5 in 1 DRIfT test.
- Take the FREE Cognitive Function Test here
—
Thank you for reading!
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices.
Please support our research by becoming a Friend of Food for the Brain.
References
1 Peng, M., et al. Dietary Total Antioxidant Capacity and Cognitive Function in Older Adults. J Nutr Health Aging (2023).
2 Basambombo LL, Carmichael PH, Côté S, Laurin D. Use of Vitamin E and C Supplements for the Prevention of Cognitive Decline. Ann Pharmacother. 2017 Feb;51(2):118-124. doi: 10.1177/1060028016673072. Epub 2016 Oct 5. PMID: 27708183.
3 Yu JT, Xu W, Tan CC, Andrieu S, Suckling J, Evangelou E, Pan A, Zhang C, Jia J, Feng L, Kua EH, Wang YJ, Wang HF, Tan MS, Li JQ, Hou XH, Wan Y, Tan L, Mok V, Tan L, Dong Q, Touchon J, Gauthier S, Aisen PS, Vellas B. Evidence-based prevention of Alzheimer’s disease: systematic review and meta-analysis of 243 observational prospective studies and 153 randomised controlled trials. J Neurol Neurosurg Psychiatry. 2020 Nov;91(11):1201-1209. doi: 10.1136/jnnp-2019-321913. Epub 2020 Jul 20. PMID: 32690803; PMCID: PMC7569385.
4 Yao JK, Leonard S, Reddy R: Altered glutathione redox state in schizophrenia. Dis Markers 2006, 22(1):83–93 ; see also Gawryluk JW, Wang J-F, Andreazza AC, Shao L, Young LT: Decreased levels of glutathione, the major brain antioxidant, in post-mortem prefrontal cortex from patients with psychiatric disorders. Int J Neuropsychopharmacol 2011, 14(01):123–130.
5 Torres LL, Quaglio NB, de Souza GT, Garcia RT, Dati LM, Moreira WL, Loureiro AP, de Souza-Talarico JN, Smid J, Porto CS, Bottino CM, Nitrini R, Barros SB, Camarini R, Marcourakis T. Peripheral oxidative stress biomarkers in mild cognitive impairment and Alzheimer’s disease. J Alzheimers Dis. 2011;26(1):59-68. doi: 10.3233/JAD-2011-110284. PMID: 21593563
6 Park SA, Byeon G, Jhoo JH, Kim HC, Lim MN, Jang JW, Bae JB, Han JW, Kim TH, Kwak KP, Kim BJ, Kim SG, Kim JL, Moon SW, Park JH, Ryu SH, Youn JC, Lee DW, Lee SB, Lee JJ, Lee DY, Kim KW. A Preliminary Study on the Potential Protective Role of the Antioxidative Stress Markers of Cognitive Impairment: Glutathione and Glutathione Reductase. Clin Psychopharmacol Neurosci. 2023 Nov 30;21(4):758-768. doi: 10.9758/cpn.23.1053. Epub 2023 Jul 14. PMID: 37859449; PMCID: PMC10591176.
7 Park SA, Byeon G, Jhoo JH, Kim HC, Lim MN, Jang JW, Bae JB, Han JW, Kim TH, Kwak KP, Kim BJ, Kim SG, Kim JL, Moon SW, Park JH, Ryu SH, Youn JC, Lee DW, Lee SB, Lee JJ, Lee DY, Kim KW. A Preliminary Study on the Potential Protective Role of the Antioxidative Stress Markers of Cognitive Impairment: Glutathione and Glutathione Reductase. Clin Psychopharmacol Neurosci. 2023 Nov 30;21(4):758-768. doi: 10.9758/cpn.23.1053. Epub 2023 Jul 14. PMID: 37859449; PMCID: PMC10591176.
8 Martínez de Toda I, Miguélez L, Vida C, Carro E, De la Fuente M. Altered Redox State in Whole Blood Cells from Patients with Mild Cognitive Impairment and Alzheimer’s Disease. J Alzheimers Dis. 2019;71(1):153-163. doi: 10.3233/JAD-190198. PMID: 31356205.
9 J. Frontiñán-Rubio et al. Molecular and Cellular Neuroscience 92 (2018
10 Witschi A, Reddy S, Stofer B, Lauterburg B: The systemic availability of oral glutathione. Eur J Clin Pharmacol 1992, 43(6):667–669.
11 Lavoie S, Murray MM, Deppen P, Knyazeva MG, Berk M, Boulat O, Bovet P, Bush AI, Conus P, Copolov D, Fornari E, Meuli R, Solida A, Vianin P, Cuénod M, Buclin T, Do KQ: Glutathione precursor, N-acetyl-cysteine, improves mismatch negativity in schizophrenia patients. Neuropsychopharmacology 2008, 33(9):2187–2199.
12 Ohlenschlager G,Treusch G, patent number: 5925620 International Classification A61K 3800 for synergistic action of anthocyanidins and glutathione
13 Bradlow RCJ, Berk M, Kalivas PW, Back SE, Kanaan RA. The Potential of N-Acetyl-L-Cysteine (NAC) in the Treatment of Psychiatric Disorders. CNS Drugs. 2022 May;36(5):451-482. doi: 10.1007/s40263-022-00907-3. Epub 2022 Mar 22. Erratum in: CNS Drugs. 2022 Apr 28;: PMID: 35316513; PMCID: PMC9095537.
14 Berk M, Copolov D, Dean O, Lu K, Jeavons S, Schapkaitz I, Anderson-Hunt M, Judd F, Katz F, Katz P, Ording-Jespersen S, Little J, Conus P, Cuenod M, Do KQ, Busha AI: N- acetyl cysteine as a glutathione precursor for schizophrenia—a double-blind, randomized, placebo-controlled trial. Biol Psychiatry 2008, 64(5):361–368.