‘Our Children No Longer Need to Worry About Our Cognitive Decline’
‘Our Children No Longer Need to Worry About Our Cognitive Decline‘

What one family learned from living through dementia and why they decided to take action.
When dementia affects a family, the impact often extends far beyond the person who receives the diagnosis. Many people begin to worry about cognitive decline, wondering whether it is an inevitable part of ageing or whether there is anything they can do to reduce their risk.In this story, Peter shares how watching his mother develop dementia changed the way he and his wife thought about ageing, why they decided to take a more proactive approach to their brain health, and how that decision ultimately gave their children something they hadn’t expected: peace of mind.
Most people do not start thinking seriously about dementia until it touches someone they love. Yet every day in the UK, around 790 people receive a dementia diagnosis, the equivalent of seven double-decker buses full of families beginning a journey they never expected to take.
Why One Family Decided Not to Worry About Cognitive Decline
For Peter and his family, dementia was not something they read about in the news or encountered through awareness campaigns. It arrived at their front door.
As his mother’s dementia progressed, the family witnessed first-hand how profoundly the condition could affect daily life. For a period, she lived with Peter and his wife, giving them a close-up view of the challenges, heartbreak, and uncertainty that often accompany cognitive decline.
Their children were young when their grandmother first became unwell and were old enough to witness much of what followed. They saw the gradual changes in her memory, independence, and ability to live the life she had once enjoyed. Like many families affected by dementia, they adapted as best they could, but experiences like these leave their mark.
Should You Worry About Cognitive Decline if Dementia Runs in Your Family?
At first, the family’s focus was entirely on supporting a much-loved mother and grandmother. Then, as they watched dementia unfold over many years, the children naturally started asking questions about the future. What would happen to their parents? Was this simply what ageing looked like? Could anything be done to reduce the risk of dementia?
For Peter, this became one of the most difficult parts of the journey.
“It wasn’t fair that they should have this burden so young.”
When his mother died in 2016, he and his wife found themselves reflecting on everything the family had been through. They knew there were no guarantees when it came to health and ageing, but they also felt increasingly uncomfortable with the idea of simply hoping for the best.
Instead, they made a decision. Rather than focusing on what they could not control, they would focus on what they could.
“We decided to do something about it. We wanted to keep our physical and cognitive health together for as long as possible.”
That decision marked the beginning of a journey that continues today.
What to Do Instead of Worrying About Cognitive Decline
Peter’s interest in health had not appeared overnight.
Years earlier, they had discovered Patrick Holford’s work and become increasingly interested in nutrition and healthy ageing. Like many people, they had spent years trying to understand how food, lifestyle, and everyday habits influence long-term wellbeing.
Dementia, however, gave that interest a new urgency, as brain health was no longer an abstract topic. It had become deeply personal.
Instead of feeling powerless, they wanted to understand more about the factors associated with cognitive decline and, more importantly, what practical steps they could take to support healthy brain ageing. This led them to Food for the Brain’s educational resources, the Cognitive Function Test, and DRIfT biomarker testing.
They were not looking for guarantees or predictions about the future. They wanted a clearer understanding of where they stood and, perhaps more importantly, what they could actually do about it.
Measuring What Matters
The first steps? Understanding where they actually stood.
After years of watching dementia affect someone they loved, they wanted more than good intentions. They wanted a clearer picture of their current health and a better understanding of where they should focus their efforts.
The Cognitive Function Test provided one piece of that picture. Having first completed the assessment many years ago, Peter returned to it years later with a renewed interest in dementia prevention and healthy ageing. His score improved from 51 to 73.
The score itself was only part of the story. What mattered more was having a way to check in on how things were going. After everything the family had been through, it felt reassuring to have something tangible to measure rather than simply wondering whether their efforts were making a difference.
Alongside cognitive testing, they also began monitoring several biomarkers associated with brain health through DRIfT testing and implementing the guidance they were given along the way. The results showed encouraging changes across a number of areas:
Key Changes Over Time
| From | To | |
| Cognitive Function Test | 51 | 73 |
| Homocysteine | 11.9 µmol/L | 7.16 µmol/L |
| HbA1c | 5.5% | 5.1% |
| Omega-3 Index | 7.69% | 10.3% |
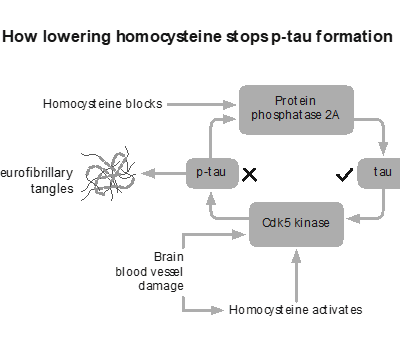
His homocysteine level proved particularly useful information. Although he had already made a number of dietary and lifestyle changes, his levels remained higher than he would have liked, hovering at around 12 µmol/L across several tests. Regular testing allowed him to identify the issue, make further adjustments, and see how his body responded over time. After introducing vitamin B12, his homocysteine eventually reduced from 11.9 µmol/L to 7.16 µmol/L.
Without testing, he would never have known that this important marker remained elevated, as it is not something you can feel. Equally, without repeating the test, he would never have known whether the changes he made were having the desired effect. never have known whether the changes he made were having the desired effect.
Lifestyle Changes That Reduced Their Worry About Cognitive Decline
There was no single intervention that transformed their health overnight. Instead, they gradually reshaped the way they lived. Ultra-processed foods disappeared from the shopping trolley, wheat was removed from the diet, fermented foods became a regular feature at mealtimes, and targeted supplements were added where testing suggested they might be beneficial. Alongside this, they stayed physically active, walked regularly, and continued to challenge themselves mentally through activities such as completing The Times crossword.
Like many people who successfully improve their health over the long term, they did not follow a perfect plan or look for a magic solution. They focused on making changes they could sustain and enjoy, building habits that fitted naturally into the life they wanted to lead in retirement.
In many ways, their experience reflects what the research increasingly tells us about brain health: it is rarely one single intervention that matters most, but the cumulative effect of multiple factors working together over time, from nutrition and exercise to sleep, metabolic health, social connection, and lifelong learning.
The Difference It Made
Over time, they began to notice subtle shifts. Their thinking felt clearer, they felt more optimistic about ageing, and they gained confidence from seeing improvements in some of the markers they were tracking. Yet perhaps the biggest change was not physical at all. For years, dementia had been something that happened to their family. Now, instead of feeling defined by that experience, they felt they were actively shaping what came next.
The conversations within the family began to change, too. Their children and their children’s partners became more interested in brain health, nutrition, and prevention, turning what began as one family’s experience of dementia into a wider conversation about healthy ageing. Rather than seeing cognitive decline as an inevitable part of getting older, the family started to see it through a different lens, one that recognised the role informed choices can play in supporting long-term brain health.
When asked what has mattered most, Peter does not talk about biomarkers, supplements, or cognitive test scores. He returns instead to the concern that first motivated him and his wife to take action. Watching their grandmother’s decline had left a deep impression on the children, who naturally worried about what the future might hold for their parents. Those concerns did not disappear overnight, but they gradually eased as they saw their parents taking positive action, learning more about brain health, and making it a priority.
Reflecting on everything that had changed, Peter felt one thing stood out above all the others. He said “our children no longer need to worry about our cognitive decline.”
For Peter, that is the result that matters most.
Want to understand your own brain health?
Peter’s experience is not really about a test score, a supplement, or a blood result. Those were simply tools that helped him and his wife better understand their health, make informed decisions, and feel more confident that they were moving in the right direction.
At its heart, this is a story about a family who experienced dementia first-hand and decided not to leave the future entirely to chance. It is about protecting independence, preserving memories, staying connected to the people we love, and approaching later life with greater confidence and optimism.
At Food for the Brain, we believe more people deserve the opportunity to do the same. As a research and education charity, our mission is to make dementia prevention and optimal brain health possible by translating the latest science into practical, accessible actions that people can take today. Through research, education, testing, and behaviour-change programmes, we help people understand their brain health and take positive action while there is still time.
Whether you are simply curious about your brain health or looking for ways to reduce your risk, you can get started by:
-
Taking the free Cognitive Function Test and tracking your progress over time.
-
Exploring DRIfT biomarker testing to gain deeper insight into key areas of brain health.
-
Becoming a FRIEND of Food for the Brain and gaining access to the COGNITION programme, educational webinars, group coaching and ongoing support








")