Brain Health And Vegan Eating: What It Means For Long Term Cognitive Health
Veganuary, a movement encouraging people to adopt a vegan diet for the month of January, has become a cultural ritual ethical environmental marketed as healthy, yet when it comes to brain health and vegan eating the story is more complex.
But nutrition does not respond to ideology.
For many people, Veganuary is a short-term experiment. For others, it becomes a long-term way of eating. The question most rarely asked is also the most uncomfortable:
What happens to the brain when all animal foods are removed from the diet?
And more importantly, is that compatible with long-term cognitive health?
To answer this question, we need to evaluate Veganuary in light of what we know about optimum nutrition for the brain – particularly the vital role of omega-3 fatty acids, B vitamins, choline and other essential nutrients.
Modern neuroscience is unequivocal. Nutrients such as omega-3 DHA, vitamin B12, choline, iron, zinc, and vitamin D are not optional for brain function. They are structural, metabolic, and protective. Remove their primary dietary sources without replacing them precisely, and the brain pays the price.
Omega-3 DHA: The Brain’s Cornerstone Fat
The brain is 60% fat, and omega-3 fatty acids, particularly DHA (docosahexaenoic acid), are critical for its structure and function. DHA makes up the bulk of neuronal membranes, enabling communication between brain cells, memory retention, and overall cognitive performance [1]. Research consistently shows that DHA deficiency correlates with reduced cognitive ability, mood disorders, and increased risk of neurodegeneration [2].
Animal foods, particularly oily fish, are the richest sources of preformed DHA. On a vegan diet, the main plant-based source of omega-3 comes in the form of ALA (alpha-linolenic acid), found in flaxseeds, walnuts, and chia seeds. However, the conversion of ALA to DHA in the human body is remarkably inefficient – typically less than 5% [3]. Without preformed DHA from marine sources or supplementation with algae-derived DHA, vegans are likely to fall short of their brain’s DHA needs.
Studies reveal that populations consuming more fish, such as the Japanese, have far lower incidences of dementia and mental decline compared to Western nations, where fish intake is minimal. A meta-analysis confirmed that higher omega-3 levels correlate with a lower risk of cognitive decline [4]. For individuals adopting a vegan diet without supplementing DHA, there’s a real risk of impairing brain function over time.
(Want to know if you’re getting enough omega-3 fatty acids in your diet? The only way to truly know is to test your serum omega-3 level – order your at home test kit today).
Vitamin B12: The Brain’s Energy Catalyst
Vitamin B12 is not a “nice to have” micronutrient. It is a neurological necessity. Found almost exclusively in animal products such as meat, fish, and dairy, it plays a crucial role in maintaining brain function, energy metabolism, and protecting against neurological damage. It is essential for methylation, a process that keeps homocysteine levels in check. Elevated homocysteine has been shown to shrink brain volume and accelerate cognitive decline [5].
A lack of B12 results in pernicious anemia, brain fog, memory loss, depression, and even irreversible nerve damage. Worryingly, B12 deficiency is common among vegans who do not supplement or consume fortified foods. Even those who attempt to rely on plant-based sources of B12, such as spirulina or fermented foods, often don’t realise that these contain inactive analogues of B12 that are not bioavailable to humans [6].
For long term vegans, the failure to address B12 through supplementation could lead to symptoms of mental fatigue, reduced concentration, and mood imbalances in the short term, while increasing the risk of dementia in the long run.
(This is why we offer our DRIfT 5-in-1 at-home blood test, so you can easily check your omega-3, homocysteine, vitamin D, HbA1C, and glutathione levels from the comfort of your own home while contributing to our research and charitable work).
Vitamin B12: The Brain’s Energy Catalyst
Choline rarely features in plant-based nutrition conversations. It should.
An often-overlooked nutrient, it is another brain-essential compound predominantly found in animal foods like eggs, liver, and fish. It is the precursor to acetylcholine – a neurotransmitter essential for memory, learning, and mental clarity. Without adequate choline, cognitive performance can take a significant hit, especially in the aging brain [7].
Eggs, for example, are one of the richest sources of dietary choline. However, for individuals participating in Veganuary, eggs are off the table. While small amounts of choline can be found in soybeans, quinoa, and cruciferous vegetables, meeting the brain’s daily requirements is nearly impossible without animal foods or supplementation. Emerging research suggests that a low choline intake may even contribute to neuroinflammation and a higher risk of Alzheimer’s [8].
Vitamin D: The Sunshine Hormone
Vitamin D, a hormone as much as a vitamin, is vital for mental health, cognition, and neuroprotection. Deficiency in vitamin D has been linked to depression, brain aging, and increased dementia risk. During winter, when Veganuary occurs, obtaining sufficient vitamin D is already challenging for most individuals living in northern latitudes.
While vitamin D can be found in small amounts in mushrooms exposed to UV light, it is primarily found in oily fish, egg yolks and fortified dairy – all of which are absent in a vegan diet. If Veganuary participants fail to supplement with vitamin D3, they risk worsening mood, memory, and overall mental resilience during the winter months [9].
Iron and Protein: The Overlooked Trio
Beyond omega-3, B12, and choline, a vegan diet also increases the risk of deficiencies in iron, zinc, and high-quality protein – all critical for brain health. Heme iron, found in meat, is far more bioavailable than non-heme iron from plants. Iron deficiency is associated with brain fatigue, poor concentration, and low mood [10].
Protein is equally important for maintaining neurotransmitter balance and brain structure. While it is possible to obtain sufficient protein on a vegan diet through lentil, legumes, tofu etc, doing so requires intention and planning. Without adequate protein, mood and energy levels can decline rapidly.
Is There a Brain-Friendly Vegan Path?
While the standard Veganuary approach – removing animal products without careful planning – could pose clear problems to brain health long term, a well-supplemented vegan diet can be brain-friendly. It encourages more fruit and vegetables, legumes, lentils, nuts and seeds, and (hopefully) a more whole-food approach.
(Our founder, Patrick Holford, personally eats a ‘Pegan’ diet – a hybrid of vegan and pescatarian – eating only fish and eggs in terms of animal products.) To summarise, a brain-friendly diet can be vegan, pescatarian, or omnivorous. The common denominator is not ideology. It is nutritional sufficiency.
The best way to know that your dietary choices are supporting your brain health is by testing and tracking. We offer our FREE Cognitive Function Test here and our at home pin prick blood test kits that you can purchase here
Become a Friend & join the COGNITION Program: Support our mission with a small monthly donation and receive tailored steps to improve your brain resilience and track your progress.
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
The Only Person Who Can Change the Mental Health Crisis is YOU
By Catherine Verner
That’s why we want to say a heartfelt THANK YOU for being a CITIZEN SCIENTISTspreading the word and encouraging more people to make the brain-saving changes we champion at Food for the Brain.
From Humble Beginnings to a Global Movement
Two decades ago, the idea that nutritional and lifestyle choices could alter the trajectory of cognitive health was seen as a far-fetched notion. Back then, cognitive decline was considered inevitable. The idea was drowned out by entrenched beliefs and outdated medical paradigms that focused more on reactive treatments than addressing root causes.
At Food for the Brain, we dared to challenge conventional thinking. We envisioned a future where prevention takes centre stage. Our mission became clear;: to empower you with the knowledge and tools to take charge of your brain health, shape your future, and unlock your cognitive potential.
Thus began a journey that has grown into a global movement for building cognitive resilience and brain health.
Citizen Scientist Badge
—
Prevention is the Only Viable Way Forward
The truth is, prevention has been sidelined in healthcare. Instead, healthcare systems are geared toward managing symptoms, dominated by pharmaceuticals, while underlying causes remain unaddressed.
The evidence is clear: proactive steps – like improving your nutrition, staying active, managing stress, and prioritising sleep – can prevent or significantly slow cognitive decline. At Food for the Brain, you are helping to prove that prevention is real, achievable, and essential.Through our COGNITION Programme, we identify and address the modifiable risk factors for conditions like Alzheimer’s and cognitive decline. If you haven’t started your journey yet, now is the time to act.
The Power of You: Citizen Scientist in Action
This progress has been possible because of you – our dedicated Citizen Scientists. By the end of 2024, more than 450,000 free Cognitive Function Tests have been completed worldwide. That’s extraordinary—and it’s thanks to you!
Your commitment drives our work forward. This isn’t the result of one team, but the collective effort of thousands across 70+ countries.
Every time you take a test, complete a questionnaire, or share your experience, you’re contributing to something bigger than yourself. You are part of a groundbreaking, people-powered movement that is changing how brain health is understood, measured, and protected. The data you provide doesn’t just sit in a database—it fuels new research, shapes prevention strategies, and strengthens our ability to fight cognitive decline globally. Because of you, we are shifting the narrative from hopelessness to empowerment. Together, we are proving that your brain health—and the health of millions—is not left to chance. You’re not just participating; you’re leading the way.
And today, we’re ready to go even further.
A New Frontier: The COGNITION Biobank
We are thrilled to announce the creation of theCOGNITION Biobank—a pioneering resource advancing cognitive health research.
Why does this matter? With the global cost of dementia projected to reach $2.8 trillion by 2030, it’s clear that prevention must be prioritised. For governments and healthcare systems to take action, they need hard facts.
Thanks to nearly half a million participants like you, the COGNITION Biobank integrates data from Cognitive Function Tests, health and lifestyle questionnaires, and biomarker results. This allows researchers to explore the links between nutrition, exercise, sleep, mental stimulation, and cognitive health.
Imagine researchers discovering that something as simple as adding omega-3s, improving sleep, or managing stress could cut dementia risk in half. Now picture thousands of people across the globe applying that knowledge to transform their futures. This is the power of the COGNITION Biobank. It’s not just data – it’s hope, answers, and a global step forward. Your contributions today are fuelling discoveries that could rewrite the future for your children, grandchildren, and people around the world. You’re not only helping yourself; you’re helping millions.
The Biobank is already one of the most comprehensive anonymised databases of its kind. This is where prevention meets action. Your participation drives real, global change. Your data is safe. At Food for the Brain, we take rigorous measures to ensure all contributions remain fully anonymised, adhering to GDPR and HIPAA standards.
Your Brain, Your Impact: Act Now
Your role in this movement has never been more important. Here’s how you can make a difference:
Join the COGNITION Program: Receive tailored steps to improve your brain resilience and track your progress.
Become a Friend: Support our mission with a small monthly donation and be part of the solution.
Share Your Story: Have you seen a positive change? Inspire others. Share your message by emailing Cath at research@foodforthebrain.org.
Spread the Word: Encourage your friends, family, and colleagues to take the test and join this global initiative. Order the Citizen Science Action pack here
Citizen Scientist Pack
—
Together, we’re proving that prevention works.
Your brain matters.
Your actions matter.
Let’s pioneer the future of brain health—together.
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
Depression, now the leading cause of disability globally, affects millions. According to the World Health Organization, it represents a significant disease burden, particularly in high-income countries (1). With a staggering 100 million antidepressant prescriptions issued annually—a 70% increase in five years—it’s clear that something is going wrong in our modern western world (1).
Thankfully, nutrition and lifestyle changes provide science-backed ways to boost our mood naturally.
Depression manifests through persistent feelings of hopelessness, low energy, disrupted sleep, and even physical changes such as weight loss or gain (2). The root causes can be multifactorial—psychological stress, biochemical imbalances, or nutritional deficiencies.
But here’s the good news: you can take simple, practical steps to nourish your brain, boost serotonin, and improve your mood naturally.
—
7 Ways to Boost Mood and Brain Function
—
1. Increase Your Omega-3 Fats
Your brain is 60% fat, and omega-3 DHA and EPA are critical for its structure and function. Countries with high fish consumption have lower depression rates. A study from Harvard Medical School found that EPA, specifically, has potent antidepressant effects.
A meta-analysis published in Psychopharmacology Bulletin found that higher omega-3 intake reduces depressive symptoms by 53%. Omega-3 helps build brain cell membranes and boosts serotonin receptor function, which improves mood and cognition.
What to do: Eat oily fish like salmon, sardines, and mackerel at least twice a week or supplement with high-dose omega-3 fish oil. Aim for 1,000–2,000 mg of EPA and DHA combined daily (4, 5, 6).
—
2. Optimise Your B Vitamins and Lower Homocysteine
The little-known amino acid, homocysteine, may double your risk for depression if levels are elevated. This toxic by-product accumulates when you’re deficient in B6, B12, and folic acid, impairing brain chemistry.
Studies by Professor David Smith from Oxford show that lowering homocysteine can dramatically slow brain shrinkage and improve mood. Which is why we now offer at home homocysteine test kits so you can monitor your own level and prevent disease (7,8,9).
What to do: Eat leafy greens, whole grains, and fortified foods. Test your homocysteine and aim for levels below 7 μmol/L. Supplement with a methylated B complex (20 mg B6, 500 μg B12, and 400 μg methylfolate).
—
“B vitamins are brain-makers; without them, key neurotransmitters like serotonin can’t be synthesised” – Patrick Holford, Upgrade Your Brain.
—
3. Fuel Your Brain with Serotonin Precursors
Serotonin, your “happy hormone”, is made from tryptophan, an amino acid found in protein-rich foods like fish, poultry, beans, and eggs. For some, tryptophan conversion to serotonin is impaired due to poor digestion or low stomach acid, common with age and stress.
Supplementing with 5-HTP can bypass these barriers. Clinical studies show 5-HTP compares favourably with SSRIs in treating depression (10, 11, 12, 13).
What to do: Include tryptophan-rich foods daily and consider a 5-HTP supplement (100–200 mg twice daily). Always consult your doctor if combining with antidepressants.
Maintaining stable blood sugar levels is essential for mood regulation, as uneven glucose supply to the brain can lead to irritability, fatigue, and depressive symptoms. Diets high in refined carbohydrates and sugar contribute to these fluctuations and are linked to poor mood and an increased risk of depression. A study of 3,456 adults found that individuals consuming diets rich in processed foods had a 58% greater risk of depression, whereas those eating whole foods experienced a 26% reduced risk (14, 14, 16).
Refined sugars also deplete mood-enhancing nutrients like B vitamins, essential for energy production, and divert chromium, which is vital for glucose regulation. Adopting a low glycaemic load (GL) diet, avoiding caffeine and alcohol, and focusing on whole foods, fruits, and vegetables can help stabilise blood sugar levels and improve mood.
What to do: Follow a Low-GL diet with whole foods, low-GL carbs, and protein at every meal. Avoid sugar, caffeine, and alcohol .
5. Boost Your Vitamin D Levels
The “sunshine vitamin,” vitamin D, is essential for mood regulation. Research shows a 40% lower incidence of depression in those with adequate vitamin D. Alarmingly, over 60% of the UK population is deficient during winter (17, 18, 19, 20).
What to do: Get tested and aim for levels above 75 nmol/L. Supplement with 2,000–3,000 IU daily in winter months.
—
6. Include Chromium to Combat Atypical Depression
If you suffer from atypical depression—characterised by weight gain, fatigue, and carbohydrate cravings—you might benefit from chromium. Studies show chromium supplementation can improve mood scores by up to 83% (21, 22, 23).
What to do: Include whole grains and vegetables or supplement with 600 mcg of chromium picolinate daily.
—
7. Bring on the Sunshine and Movement
Exercise and sunlight have a direct effect on serotonin levels and mood. Regular exercise boosts brain-derived neurotrophic factor (BDNF), which helps build new brain cells and connections】.
What to do: Aim for 30 minutes of exercise daily and sun exposure for 15 minutes, when safe.
—
Key Action Plan
Eat oily fish twice weekly or supplement omega-3s with at least 1,000 mg EPA and DHA.
Test and lower homocysteine with B6, B12, and folic acid supplements.
Try 5-HTP to boost serotonin naturally.
Follow a Low-GL diet to stabilise blood sugar.
Supplement vitamin D during winter. Find out more about dose here.
Add chromium for atypical depression.
Exercise regularly and get sensible sun exposure.
—
—
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
References
World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates. WHO; 2017.
Brown G, et al. Social support, self-esteem and depression. Psychol Med. 1986;16(4):813-31.
Hibbeln JR. ‘Fish consumption and major depression’. Lancet, vol 351(9110), pp. 1213 (1998)
M. Peet and R, Stokes, Omega 3 Fatty Acids in the Treatment of Psychiatric Disorders Drugs, vol 65(8), pp. 1051-9 (2005)
S Kraguljac NV, Montori VM, Pavuluri M, Chai HS, Wilson BS, Unal SS (2009) Efficacy of omega-3 Fatty acids in mood disorders – a systematic review and metaanalysis. Psychopharmacology Bulletin 42(3):39-54
Hibbeln JR. Fish consumption and major depression. Lancet. 1998;351(9110):1213.
Coppen A, Bailey J. Folic acid and affective disorders. J Affect Disord. 2000;60(2):121-30.
Taylor MJ, Carney SM, Goodwin GM, Geddes JR. Folate for depressive disorders. Cochrane Database Syst Rev. 2003;(2):CD003390.
Smith AD, Refsum H. Homocysteine, B vitamins, and cognitive impairment. Annu Rev Nutr. 2016;36:211-39.
Poldinger W et al. A comparison of 5-hydroxytryptophan and fluvoxamine. Psychopathology. 1991;24(2):53-81.
E. Turner, Serotoninalacarte: Supplementation with the serotonin precursor 5-hydroxytryptophan.’ Pharmacology&Therapeutics (2005) [article in press].
W. Poldinger et al. A functional-dimensional approach to depression: serotonin deficiency and target syndrome in a comparison of 5-hydroxytryptophan and fluvoxamine, Psychopathology vol 24(2), pp. 53-81 (1991)
Associate editor: K.A. Neve ‘Serotonin a la carte: Supplementation with the serotonin precursor 5-hydroxytryptophan’ ErickH. Turner a,c,d,*, Jennifer M. Loftis a,b,c, AaronD. Blackwell a,b,e Pharmacology & Therapeutics(2005) www.elsevier.com/locate/pharmthera
Akbaraly TN, Brunner EJ, Ferrie JE, et al. Dietary pattern and depressive symptoms in middle age. Br J Psychiatry. 2009;195:408–13.
Benton D, Owens DS, Parker PY. Blood glucose influences memory and mood in an everyday setting. Biol Psychol. 1982;14(1-2):129–35.
Christensen L. Psychological distress and diet – effects of sucrose and caffeine. J Appl Nutr. 1988;40(1):44–50.
Lansdowne AT, Provost SC (1998): Demonstrates that vitamin D3 supplementation enhances mood in healthy subjects during winter.
C. Wilkins et al. (2006): Links vitamin D deficiency to low mood and poorer cognitive performance in older adults.
A. Nanri et al. (2009): Discusses the association between vitamin D levels and depressive symptoms across seasonal changes.
R. Jorde et al. (2008): Shows that vitamin D supplementation alleviates depressive symptoms in overweight and obese individuals
Lifting Depression – The Chromium Connection by Dr Malcolm McLeod (Basic Health Publications):
J. R. Davidson et al, Effectiveness of chromium in atypical depression: a placebo-controlled trial, Biol Psychiatry, vol 53(3), pp. 261-4 (2003)
Docherty, J et al, ‘A Double-Blind, Placebo-Controlled, Exploratory Trial of Chromium Picolinate in Atypical Depression’. Journal of Psychiatric Practice. Vol 11(5), pp. 302-314, (2005)
Holford P. Upgrade Your Brain. HarperCollins; 2024.
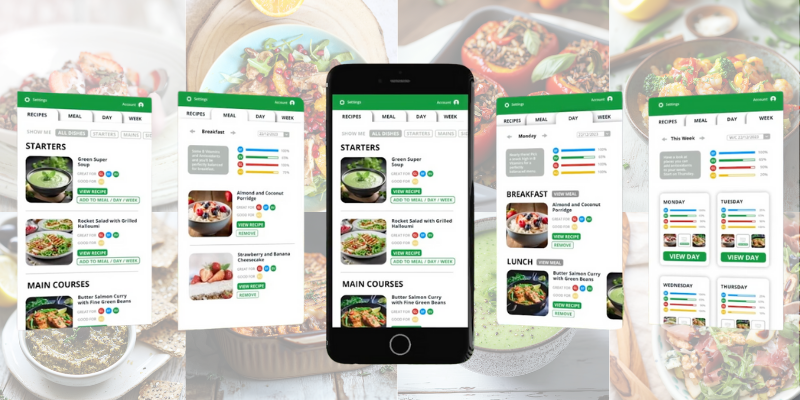
It not only provides easy meals, from breakfasts to snacks, main meals, and desserts but each recipe is designed to ‘dementia-proof’ your brain.
Launched this week, the recipes are based on extensive research which has identified the four critical qualities of meals that link to better mood, memory and mental energy, banishing brain fog and forgetfulness. These essential components are: a good quantity of brain fats, slow releasing carbs (Low GL), antioxidants and B-vitamins.
Each recipe is scored accordingly and if you choose something missing or low on one of these critical components, you can then choose a recipe higher in it next time and it will add to your daily and weekly meal score bar so you can clearly see your progress and adapt what you’re eating, to hit the brain friendly zone.
These are all easy to make, tried and tested recipes that will not only help you get out of the recipe rut but also educate, motivate and energise you in the process.
—
It won’t just help your brain health…
And the extra good news? What’s good for the brain is good for the body.
A recent study from the UK Biobank data shows that increased intake of omega-3 from fish oils reduces the risk of 35 diseases. “As far as fish is concerned, we say ‘SMASH it – S for salmon, M for mackerel, A for anchovies, S for sardines and H for herring or kipper. But many people don’t know how to make delicious food with fish.
The Upgrade Your Brain Cook App has lots of delicious recipes from breakfasts to desserts, snacks and main meals, each with brain-friendly attributes.
Each recipe prioritises:
Antioxidant-rich dishes to neutralise oxidative stress, a major contributor to brain aging. Are you stuck in a recipe rut, cooking the same limited meals over and over again?
Low sugar (GL-friendly) options to help stabilise blood sugar and support healthy weight management.
Brain-fat friendly ingredients to provide the right fats such as omega-3 for cognitive function.
B-vitamin rich meals to support energy, methylation, and homocysteine levels—key factors in maintaining brain health.
—
Here’s an example of a ‘perfect’ day.
Once you’ve picked a dish from the App, it shows you what to eat next to tick the box for these four brain-friendly requirements for a perfect day. This sample menu, for example, is low in GL and high in brain fats. This is important as anything below 45 GLs helps you to lose weight, and foods high in brain fats give you extra credit for the next day.
The Upgrade Your Brain Cook App also lets you tailor recipes to your dietary preferences (e.g., dairy-free, gluten-free, plant-based) while ensuring your meals are both delicious and scientifically designed to promote brain health.
There are lots of delicious and easy to make recipes to suit everyone from vegans to meat eaters and those who choose to avoid gluten or other food intolerances such as:
Coconut & Almond Porridge
Chicken Satay Skewers with Peanut-lime Dipping Sauce
Crispy Chickpea & Kale Snack Bowl
Spiced Salmon Burger with Sweet Potato Fries & Slaw
Thai Fish Cakes with Satay Dipping Sauce
Tofu-Quinoa Poke Bowl
Avo-Edamame Hummus with Flaxseed Crackers
Chaat Masala Chickpeas
Cherry Sorbet
Pineapple-Watermelon-Pomegranate Fruit Platter
and many more.
Wendy is a case in point “I lost 6 stone, reversed my diabetes and my energy came back following these principles. My memory and mood are transformed. I love this App. It makes healthy eating doable and fun. The recipes are fantastic and easy to make.”
The recipes, devised by nutritionist and chef Kim Close and Fiona McDonald Joyce (author of five recipe books) are all tried and tested, firm favourites and let you adapt even something like burger and fries into a brain-friendly recipe such as ‘Spicy Salmon Burgers with Coleslaw and Sweet Potato Fries’while still being absolutely delicious.
—
Here is a sample recipe:
The Upgrade Your Brain Cook App Spicy Salmon Burgers with Coleslaw and Sweet Potato Fries (serves 4)
Ingredients:
4 salmon fillets (about 150g each), skin removed
2 tbsp Cajun seasoning
200g cabbage, shredded
1 carrot, shredded
50g mayonnaise
1 tbsp apple cider vinegar
2 sweet potatoes, cut into fries
2 tbsp olive oil
Salt and pepper to taste
Instructions:
Preheat your oven to 200°C. Toss sweet potato fries with 1 tbsp olive oil and season with salt. Spread on a baking sheet and bake for 25-30 minutes, turning halfway, until crispy.
Pulse the salmon in a food processor until finely chopped. Transfer to a bowl, add Cajun seasoning, and form into four burger patties.
Heat the remaining olive oil in a pan over medium heat and cook the salmon burgers for 3-4 minutes per side, until cooked through.
For the coleslaw, mix the shredded cabbage and carrot with mayonnaise and apple cider vinegar. Season with salt and pepper.
Serve the spicy salmon burgers with coleslaw and sweet potato fries on the side.
Air Fryer Instructions: Preheat the air fryer to 200°C. Cook the sweet potato fries in the basket for about 15-20 minutes until crispy. Then, cook the salmon burgers for 10-12 minutes until they are fully cooked. Serve as above.
Upgrade Your Brain Cook App Chef Kim Close says:
“I wholeheartedly believe that nutritious food can, and should be, really delicious. We are passionate about creating recipes that look and taste fantastic! With this App, you can cook these recipes for yourself and your family and see how healthily they score. Each recipe helps people to upgrade their nutritional knowledge, cookery skills and enjoy brain-healthy, delicious meals.”
All proceeds help our mission, charitable work and research on what really prevents dementia.
Thank you for reading!
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
After a lifetime dedicated to pioneering nutrition and mental health, Patrick Holford—founder of the Institute for Optimum Nutrition (ION) and the visionary behind Food for the Brain—will be stepping down as CEO in 2025 (but will remain very much involved). Over the past 40 years, Patrick’s radical and impactful work has included establishing ION, writing 47 books translated into 30 languages, and building Food for the Brain into a global force for mental health support and prevention.
To mark this milestone, we’re delighted to share this exclusive interview with Patrick Holford by Simon Martin Editor of IHCAN magazine. From humble beginnings—selling self-published books from the back of a battered Skoda—Patrick’s mission has transformed into a fast growing, global research and education charity, changing lives by promoting prevention and optimal nutrition to address the increasing prevalence of mental health challenges.
Discover Patrick’s journey, his insights, and what’s next for his enduring legacy.
—
SIMON MARTIN: Let’s start at the end, with your latest project – preventing Alzheimer’s. Did you get interested in Alzheimer’s because you’re worried about it yourself, or because you saw where things were going?
PATRICK HOLFORD: Some years ago, I realised we knew what to do to prevent all these chronic diseases, and it HAS to be prevention. And as much as I love the whole mission where I started from, creating the profession that could then theoretically work with doctors and lots of people, the issue is, “How do you do prevention on a big scale?”
I’ve pondered that for many years. And then I thought Alzheimer’s might be a very good place to start, although ten years ago, “Alzheimer’s is preventable” was a radical statement. But I figured it would become the number one fear and the number one killer and the number one health cost. Since it is, in essence, irreversible – once you’ve got holes in your brain – you’ve got to think about prevention.
I also rather loved the homocysteine research, which was pure functional medicine or optimum nutrition. In other words, we’re not all the same, sometimes you have to test. The use of nutrients to reverse a process is very clear in the world of homocysteine, and in fact arguing that case, which is also the case for B12, opens up the door for supplements, which, of course, is a bête noir for the medical establishment. They’re very happy to talk about a bit of diet and exercise, but the concept that one might actually have to take a supplement, and that it might in fact even work better than a drug, is a big paradigm shift. So I decided to focus on Alzheimer’s prevention. In truth, when you look at it, the eight drivers, as we organise the data, are just as applicable to diabetes or heart disease or anything else.
SM: I was reading the news this morning and the Daily Mail had two “health” stories. One was a “Probiotics will kill you” type headline on a complete mess of a case report where doctors had given a bacterial pill to someone who was seriously ill with a number of overlapping diagnostic labels, and he died. Then they decided to feature a new study that claims that everything from turmeric to ashwagandha can give you liver disease. I mean – it’s 2024, and they’re still at it.
So as we celebrate ION’s 40th, part of the history we should look at is how often we’ve been first with stuff, from supplements, to probiotics to junk food – or ultra-processed foods as they call them now – and orthodox medicine is still catching up. With Alzheimer’s, of course, we’re ahead again.
But let’s rewind to the start. I was upset to realise that I don’t have a picture of our first meeting, which was when I was editor of Here’s Health, so must have been around 1980. I think you were working for Green Farm at the time.
PH: My first awakening really was at Green Farm through Brian and Celia Wright, who had some very interesting ideas about nutrition.
I was studying psychology at York university, and even then I was very interested in consciousness and mental health. I didn’t really have nutrition on the map, and so I was really learning from them. When I left university, two things happened. One was I was introduced to the book by Dr Carl Pfeiffer called Mental and Elemental Nutrients…
SM: I still have a copy on my shelf. PH:…which is really brilliant. And then I was introduced to the research of Dr Abram Hoffer. I didn’t realise at the time, but his double-blind trials on high-dose niacin in the ‘50s were the first ever on a nutrient in the history of psychiatry. I’d already dabbled in various forms of psychotherapy and I was thinking of going in that direction and by whatever quirk of fate, York university was doing quite a lot of research into schizophrenia. I remember at the time saying, “Could we meet one please?” But that didn’t seem to be on the agenda.
—
Where the interest in mental health began…
SM: What do you mean – “meet one”?
PH: Could we meet someone suffering from schizophrenia. Because I had got into construct theory, which is to do with the fact that when we talk about depression, for example, what you mean by depression and what I mean are very different things. They’re constructs. So in my holidays, I was volunteering in alcohol addiction centres. I joined a group for heroin addicts who had a choice of going to prison or going into this sort of reform school. So I went to work there, and I met schizophrenics; I just wanted to know the nature of the beast, so to speak. And around that time, I bumped into Brian and Celia, who I invited to give a talk for us. We were very into neurochemistry at York. I wasn’t so interested, but it gave me a good background in neurotransmitters and all that sort of thing. So it was that perfect storm of Carl Pfeiffer, Abram Hoffer, studying schizophrenia, learning neurochemistry, that got me excited.
Somewhere around about 1980 or so, I’d set up a health food shop in High Wycombe called the Better Health Shop, and a little room in the back called the Better Health Clinic. I called myself a nutrition consultant and I had a three-month waiting list. I developed a questionnaire, which was sort of the beginning of the questionnaire that nutritionists or nutritional therapists use today. Then I had a few people approach me saying they’d like to study to do what I was doing.
Also around that time, I remember suddenly having this realisation – perhaps all these diseases, like diabetes and heart disease, mental illness and so on, maybe they’re all a function of sub- optimum nutrition!
Right then I decided to set up an institute, or a college or whatever.
—
It started with orthomolecular medicine…
SM: Where were you getting your inspiration from at that point?
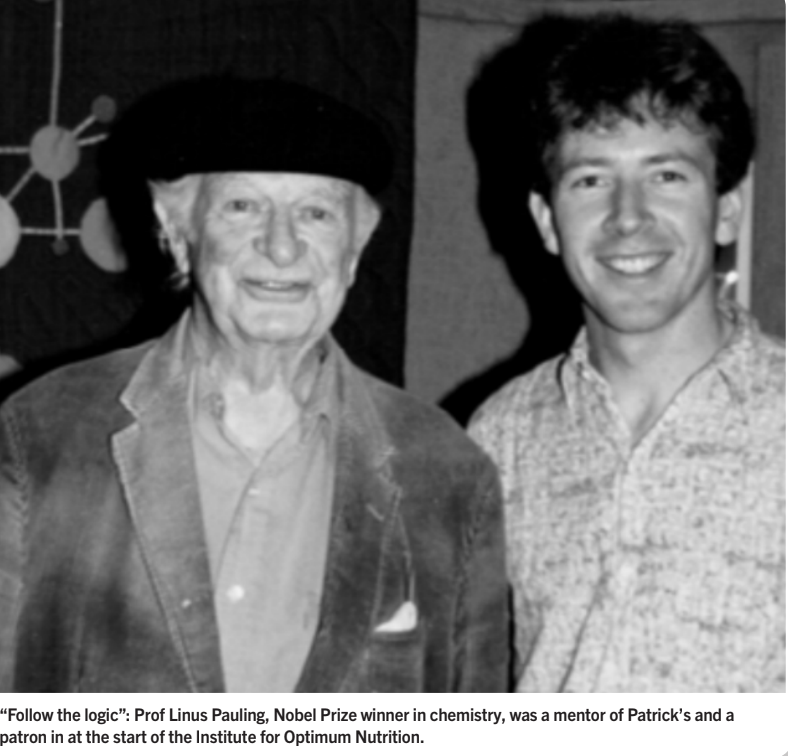
PH: I was well into the whole concept of orthomolecular medicine – the right molecules – which was really the creation of Prof Linus Pauling and Abraham Hoffer. Pauling had published the seminal paper in 1968, originally on orthomolecular psychiatry.
SM: The paper that starts: “The functioning of the brain is affected by the molecular concentrations of many substances that are normally present in the brain. The optimum concentrations of these substances for a person may differ greatly from the concentrations provided by his normal diet and genetic machinery”.
PH: I didn’t really realise it at the time, but this concept is totally in parallel with Darwin. In every edition of The Origin of Species he said that there were two driving forces for evolution: one was “conditions of existence”, and the other was natural selection. Of the two, he said, conditions of existence is the more important. If you think about it logically, natural selection doesn’t kick in until the conditions of existence change.
Prof Michael Crawford made me aware of that, with the simple question of how did we become human? Given that our genome is only 1.4% different from a chimp and that brain size in chimps and gorillas hasn’t changed at all, and ours did… the logic is it had to be a change in the conditions of existence.
He pointed out that in 1900 to get into the Army you only needed to be five foot tall. The Industrial Age diet with its refined flour and sugar and all the rest of it happened to ignore protein as we moved away from “standard” eating to man-made eating. But with the discovery of the importance of protein and going to work on a good British breakfast etc, effectively we go from five foot to six foot in a matter of 50 years.
The point that he was making is that conditions of existence, when they change – epigenetics, in effect – this works very, very fast.
The power of changing the conditions of existence is extraordinary. So whether you call it orthomolecular, or optimum nutrition or functional medicine – Jeff Bland also was a student of Linus Pauling – we’re talking the same language, and what we’ve learned is that when you create that perfect “conditions of existence” – environment – and nutrition is a big part of that, it works fast, and you can see extraordinary recovery from disease processes.
In the early days, there I was with this questionnaire and I’m a Nutrition Consultant. I’ve trained in quite a few other things as well – massage, reflexology, Bach flower remedies, kinesiology and this and that, but I found the nutrition was really working, so I cut my hair, and I got a suit and a room somewhere off Harley Street.
This is pre-ION, about 1981, and I remember a woman coming in saying, “I have systemic lupus erythematosus and Sjögren disease”. I said, “How do you spell it? What is it?” I told her, “I don’t really know about your condition, but I know about optimum nutrition”. And she got better.
And then on the same day, somebody came in with post-epidemic myalgic encephalomyelitis. I said to myself, “You think you’ve got a problem? The last one had SLE and Sjögren’s!” And he got better as well! So I grew the confidence that if you create that, “conditions of existence”, things can get better.
SM: There’s a pattern here that I’ll explore later to do with both logical thinking and your ability to tap into expert advice that I think explains a lot of your success – and the success of ION.
But as an example, you had double Nobel Prize winner Prof Linus Pauling on board early on?
Patrick launching COGNITION in China
—
Back in the 80’s when nutritional therapy didn’t exist…
PH: Yes, and another influential person around that time was Prof Derek Bryce-Smith at the University of Reading. He was a genius organic chemist, who effectively got lead out of petrol. I worked with him on his campaign, and he had also got into trace elements, zinc, selenium, manganese and so on, in the context of women who were having miscarriages and deformed babies and so on.
At the time, you had to go through a formal process to be able to register an institute, and Derek Bryce-Smith was one of the key signatories for that and was the first patron of the Institute for Optimum Nutrition. Prof Pauling was the second.
SM: Staying with the “origin story” for now…I well remember the 1980s, because obviously nutritional therapy as a profession didn’t exist. In the Here’s Health office we were regularly visited by Pearl Coleman, who lived nearby and was pushing us all to learn about the new field of allergy. At that time, there wasn’t a single specialist clinic in the NHS for allergy. Pearl championed Dr Richard Mackarness, who was single-handedly pioneering “clinical ecology” at Basingstoke Hospital until he was closed down.
[Mackarness, it’s worth saying, wrote Eat Fat and Grow Slim – a low-carb, keto, “Stone Age” program in, wait for it, 1958!]
The late great Leon Chaitow had just started writing for Here’s Health and was trying to introduce his naturopath-osteopath colleagues to supplements. In the magazine we railed against junk foods, promoted a wholefood diet and campaigned for organic gardening and farming. Our classified ads were the main source for people looking for a nutritional practitioner – and we vetted their qualifications. And that was the extent of what was going on with what we would now call nutritional therapy. There were just these oddball characters, with all due respect to Pearl, who were fanatical about this nutrition thing. It was very much a specialist, minority interest. So along you come and start an institute. Did you have from the start a big vision for what this would become?
PH: There was a big vision. And we had 73 students sign up for the Nutrition Consultants Diploma Course in the first year, so it didn’t start small!
Around then I had a very important meeting with Dr Stephen Davies and the journalist Geoffrey Cannon.
SM: Stephen Davies was amazing. He had a photographic memory and as a result his presentations on nutrition were mind-blowing. We did feature him and his colleague Dr Alan Stewart. They were “conventional” medics who had woken up! They came out with their book Nutritional Medicine in 1987.
PH: The essence of the conversation was, how do we make change happen? How do we bring this nutrition into existence in a significant way?
Geoffrey’s view was that nothing would change until you change the establishment, the major organisations. Stephen Davies said, “This is evidence-based medicine, and therefore it should be done by doctors”.
My view was it wasn’t going to happen like that. I thought that if we could create a profession of nutrition consultants who could work with doctors, doctors could refer to them, and then we might have a chance. So that was the function of the new profession, and I am so delighted that it’s taken off!
SM: I don’t remember you doing much marketing, but the thing just grew and grew.
PH: One thing that was important with the Institute is that rather than me teaching everything, I decided to get the best people I knew on each topic. Within a couple of years we would have, on average, five or six professors lecturing in a year. Prof Crawford came, and Dr Neil Ward, professor of analytical chemistry at the University of Surrey. The students rated every lecturer on content and delivery, and that was the basis of improving the education.
SM: And then you started writing…
—
Selling books from the back of a Skoda.
PH: Before I started ION I’d been selling supplements. I bought myself a cheap Skoda and whizzed around the land and sold Brian and Celia’s herbal and nutritional products. But when I asked if I could either buy in some shares or have a pay rise, they fired me.
I lived in a cottage in Burwash that I rented, and I didn’t have a phone, but there was a phone box. And I didn’t have a typewriter, but the neighbour had one. And the owner of the farmhouse wouldn’t let me use the address for a business, but the village greengrocer would.
Even though I’d been fired from Green Farm, they gave me a good wholesale distributor rate. So I wrote an advert ,which was incredibly successful, with the headline: “Don’t waste your money on vitamins”. And there were three action points: 1, “Read this book” – which didn’t exist; 2, “Ring the nutrition telephone service; and 3, “Buy these products”. So I thought I’d better write a book!
A friend did a drawing, and I went to a printer and said, “I’ve got £1,000. How much would it cost to print 10,000?” And he said, £3,000. And I said, “Well, if I give you £1,000 in 30 days and £1,000 in 60 days, 90 days, do we have a deal?” He said yes, so I had 10,000 books printed, jumped in my Skoda, and just drove around the UK. I’d knock on radio shows, and sometimes I’d give a talk – to six people, or maybe even 20 or 30 if I was lucky – and sold 8,000 copies. And then Thorson’s turned up and said they’d like to publish my Whole Health Manual, and they went on to sell a quarter of a million. So that provoked a lot of interest about the training, as well.
SM: Did you rename it as The Optimum Nutrition Bible, because that title gets mentioned most often in our In Practice section when we ask what book first inspired practitioners?
PH: The first one came out in 1981 and when Thorson’s republished it in ‘82 or ‘83 it did catalyse a bit of a revolution. And then in ‘85 or so I published Optimum Nutrition, and a few other books – The Fat Burner Diet was one of the early ones, one of the first on a low GI diet, and then The Optimum Nutrition Bible – which everyone remembers the most – in 1997. I wrote that when I left ION, which is when I went into a mad writing frenzy when I was released from running the Institute.
SM: So the growth of ION was really fuelled by you and your Skoda and selling books. People read the book and decided they wanted to know more.
PH: Yes, I remember getting an article in Cosmopolitan or an article here and there, and gradually the whole thing evolved – not without you know, “troubles”. There were troubles along the way. I’m sure we remember a few of them…
SM: And here we are with “the” book just translated into Chinese and about to hit a market of umpteen millions…but what’s your current book count?
PH: It’s 48 books in more than 30 languages.
SM: You always amaze me that you not only have great ideas, whether it’s ION, Food for the Brain or the Alzheimer’s campaign, but you’re incredibly productive. What’s the secret?
PH: I think it’s because I see where things are going. I’m not really a good manager, and I get bored quite easily. But when I have a strong sense of where something is going, I get focused on that. I’m very bad at the past. I got 8% in my history exam, but I did well in maths and economics.
So yes, there’s a sort of perseverance. When an idea forms in my mind that I think has got arms and legs, I just keep going. What I’ve certainly learned in relation to books, and also in life, is to totally absorb myself in a subject. And work hard. So when I’m writing a book, I’m up at 5am and I’ll always do three hours before the day begins.
I wrote The Optimum Nutrition Bible in six weeks. Not many of my books have taken more than two months. The essence is – and we saw this recently with my latest book, Upgrade Your Brain,- also the campaign – it was a purposeful, two-month campaign, just do everything – conferences, lectures, interviews, just make as much noise as you possibly can in a very short period of time to get a quantum leap. You cannot get a shift in an organisation or in a concept just by working nine to five, hoping it will steadily change. There needs to be some sort of burst.
I remember the concept of “natural highs”: I was giving a lecture at a conference in LA and met Dr Hyla Cass, associate professor of psychiatry at UCLA. I was a bit bored, and so was she. And those words dropped out of the sky. I mean literally. What? Why do we humans like to be, sometimes stimulated, sometimes chilled, sometimes concentrating, sometimes connected?
What’s the nature of those different states and how do they relate to chemistry?
We worked on that book, and out of that came supplements – Brain Food, Chill Food, Mood Food, and so on. Conceptually this was very early on and a bit radical for the health food industry. No one wanted to run with it, so I did it myself and then later they caught on. And it just amazed me that we had to wait more than a decade until the idea that you could have supplements, nutrients, and actually support your brain function, caught on.
So yes, it’s having an idea that I think has merit, and doing it and sticking with it until eventually it starts to get traction.
SM: That sounds fine, and I can understand that for the odd book and the odd project: you get an idea, you intuit that something’s going to happen with it, and you devote this burst of time to it, and just keep repeating that. But ION, 48 books and who knows how many other projects later and you’re still applying that same model. So why aren’t you a shrivelled husk of a human being by now?
PH: Well I am a bit more shrivelled! But I also I love that – and this has been so true with Food for the Brain and the charity – it’s the people that have come forward to get involved…
SM: So you get help?
PH: No question. If an idea is good.
In a sense, it’s all about raising consciousness. I should say that what’s always floated my boat is expanding my awareness, my consciousness of something. The effect of my lectures – and I think this is also true with most of the books – it’s not about the content, it’s about somehow inducing a big “Aha!” in someone that wakes them up to the idea that they are definitely the architects of their own brain’s destiny.
We’ve seen that so often in nutrition. For example, once somebody gets a cold or flu and takes a gram an hour of vitamin C, and experiences a different flight path, they never look back.
The other point in answer to that question is that I met Linus Pauling a couple of times in
the US, and had lots of interactions with him before he died. And it was a very seminal moment when he said, “Patrick, follow the logic; it’s the logic that counts”. He said to not worry about the randomised control trials – they come later. That was really important. So I trusted the logic of things, and I trusted conditions of existence, and I trusted the power of nutrients.
—
Mentored by double Nobel Prize winner & involving the great minds of our time
SM: So people are attracted to what you’re doing and they step in. But explain this. you’ve got your psychology degree and you’ve invented yourself as a nutrition consultant, and then you decide to go and connect with a double Nobel Prize winner. How do you do that? Because you seem to have a capacity to not only reach out to people, but to get them interested in what you’re doing.
PH: Well we didn’t have emails, we had to write letters. I wrote to Linus Pauling, I wrote to Abram Hoffer. I said I’d like to visit, and I jumped on a plane, I went there, and we connected. That’s how I learned. I found someone whose ideas were excellent, like Prof Michael Crawford, for example, and I wrote to them, went to meet them, and so on. So many of these scientists are humanitarians – they want their work to be shared. And so many have been phenomenally patient with me, directing my ability to accurately turn their science into something that the public can understand.
But I think they often really enjoy the questions. And they’ve enjoyed the desire to put it in the public domain, because quite a few are not that good in the public domain, but they know it’s important. So it’s not a title that exists, but it’s a communicator role. You’re also very much there. And it’s perhaps easier to put the hat on you and say “journalist”, but it amazes me how these people, these scientists, spend decades of their life in minute details, struggling to get grants, often extremely badly paid, and hoping that it will make a difference. And the old belief was, if it’s published in a journal, it will make a difference, but we now know that that is not true. So yes, it’s not difficult to reach these people, if you’re on the same track and you ask decent questions.
SM: And you get them involved, how?
PH: Well now we have emails and it’s easier.
I just read a beautiful paper from a lovely professor at the University of Maryland on two cases of severe autism, reversed – loved your report in IHCAN on that. So I dropped him an email, and I explained the concept of everything we’re doing and said, “I’d love to talk”. He got back to me and said,“I adore what you’re doing. I’ve checked it out. It’s totally in alignment, let’s talk”. So he’s on board because we’re launching COGNITION for smart kids and teens next year.
SM: It’s telling that they don’t dismiss you because you’re some kind of popular nutrition guru – they take you seriously. Would you say that’s again down to the quality of the questions you ask? I’m plugging away at this because, as you mentioned, your career has not been without some pushback, to put it mildly, and this seems to indicate a new appreciation, not necessarily for you personally, but for nutritional therapy as a serious endeavour in general.
Experts in the Alzhiemers Prevention Group
PH: Well it’s just bringing people together – they tolerate me! I do ask interesting questions sometimes, but we have these Zoom meetings, and people love them – and they disagree with each other. Recently I did a brain fat think tank and then an anti-antioxidant, anti-ageing brain think tank, and I get three scientists together, and I pose questions, and the best ones are quite “Vulcan”; they’re happy to say “I don’t know of any evidence for that” – unlike GPs, who seem to be trained to never say “I don’t know” – and they love the exchange.
It’s just about the science. It’s about the logic. It’s the old Linus Pauling line of “follow the logic”. It doesn’t really seem to be so relevant what my qualifications are as such. And you know, I’m not writing a letter to the Lancet.
I always thought professors talk to professors more, and doctors talk to doctors more, and so on. But no, it’s very rare that somebody doesn’t respond. And that’s what I also thought was so lovely about optimum nutrition, is that it isn’t a fixed thing. It can mutate, it can change as we learn more. It doesn’t have to be quite so static.
Sometimes supplements are my focus, but I think the important point is what Pauling and Hoffer did, to suggest the use of nutrients at amounts bigger than you can eat in order to reverse a disease process – that was a paradigm shift. And that’s why I can agree with many people who are big into diet and sugar and organic and this, that and the other, but it’s amazing how often people just shut down on the concept that a nutrient might be necessary to supplement.
The wonderful thing with Alzheimer’s and homocysteine and so on is, if your homocysteine is raised, you need 500mcg of B12 and it will come down. Well, you won’t do that with 10mcg. David Smith wrote a beautiful thing, which is the charity’s statement on supplements, that basically says the requirement is whatever corrects the disease.
—
Genetics is like a weak light.
SM: With nutrigenomics and DNA tests and all the rest of it, we can now individualise our own diet and supplement regime. Or do you not buy into that?
PH: I’m not dismissing it, but polymorphism is like a weak light, which in the darkness of changing nothing, you can see as increased risk.
People are scared about ApoE4. The other obvious one is MTHFR C677T, so I thought I would just look at the big papers on changing diet, supplements, omegas or B vitamins, and of course they’ve all measured whether there was ApoE4, or not, and MTHFR or not, and then I looked up the results – and the results of the interventions were no different. I only found one study where the “positive” gene test was associated with a difference. We’re not denying that MTHFR C677T, if you have it, increases your risk of dementia, schizophrenia, depression. It increases your risk, but not that much. It’s 4-6%. Everyone gets a bit messed up with absolute and relative risk, and suddenly the headline says more like 30%.
So yes, knowing the genetics is useful. But don’t get too hung up on it. Change your diet, take some supplements etc – the significance fades away.
More interesting are situations like the DHFR polymorphism, which means you really can’t use folic acid. It doesn’t work. I’m only just learning that it’s very prevalent in Southeast Asians, but not prevalent in Europeans. And some of the folic acid studies have done better in Europeans and worse in Southeast Asians.
So I think there are, you know, there are some real merits, but I still think “conditions of existence”.
—
Patrick’s own ‘conditions of existence’
SM: What about your own conditions of existence? What’s your own diet and supplement regime if you have one? Mine varies all the time…
PH: Sometimes I call myself a “pegan”, which is a pescatarian pagan vegan! I’m dairy allergic. I think a lot of people coming into nutrition will have had a health problem, and mine was terrible sinus trouble and ear trouble – embarrassing. So I learned that dairy didn’t work for me. I don’t really react to gluten. I don’t have much, but I don’t totally avoid it. And I was fascinated by the work on Kamut Korasan, with every study showing a massive reduction in inflammatory markers. Now that is highly glutinous wheat, right? So it’s not just gluten.
I didn’t eat any meat for 45 years, and now I’m not averse to some, but if I never ate meat, it wouldn’t bother me. I don’t salivate when I see a steak. But I worked out a long time ago, when I was exploring macrobiotics and then vegan, the evidence on omegas was so compelling that I did eat fish.
So I do make a conscious effort in that direction, whether it’s mackerel, or taramasalata, or salmon, but I’m quite fussy about where it comes from. I drink very little alcohol and I never had coffee until I met my lovely wife and she got me “addicted”. We grow our own vegetables and yes they’re organic, biodynamic, zero dig or whatever, but we’re working with a guy called Dan Kittredge of the Bio-Nutrient Research Institute, who has analysed thousands and thousands of plants, and the nutrient variation, for example, antioxidants in carrots, is 40-fold, and you can’t predict the antioxidant level from organic or biodynamic or zero dig.
SM: What about your supplement regime? Does that change?
PH: I always take a high-strength multi-vitamin, I always take extra vitamin C. I have these strips, because life’s too short to be rattling loads of boxes. Fortunately, the guys that make these make my 100% Health Pack. So I’ve got a high-strength multi, a gram of vitamin C, plus zinc, omegas…and those three I take twice a day, every day, getting that better utilisation over six hours. And in that pack is something called Brain Food, which is phospholipids and a few extra B vitamins. And then I take an AGE Antioxidant, which is alpha-lipoic acid and resveratrol and CoQ10 and all that good stuff.
But where it gets interesting is, we’ve now learned that the amount of vitamin D that’s optimal is whatever gets you at least above 75 nanomoles per litre, or probably 100; and now we learn very clearly that you’ve got to be about 8% on your omega-3 index…so if you’ve got the time and the money, you can check in and see what’s actually working on your body. And then when you start to look at the evidence for DHA, it’s at least 500mg per day, possibly 1000mg milligrams a day.
The other aspect of this optimisation thing – and it comes out of some of those very early concepts of genes interacting with environment – is looking at evolutionary models, such as humans not making vitamin C and so on.
They found this 40,000-year-old complete Homo sapiens remains in the Gower and worked out that at least 20% of his diet was seafood. It’s fair to assume that they were expending two or three times the calories that we do – no Ocado, no home delivery, no cars. Everything was walking, foraging, maybe hunting, collecting wood…and there’s nothing flat in Wales. So if 20% of their diet was marine food, and we imagine that we were coastal, living in estuaries, migrated out of Africa. So let’s assume that was normal, and that’s how our brains grow. We’re expending half of the calories that they were on, then 40% of my diet would have to be marine food to get what they were getting. When you work out how much phospholipids you would be getting, how much choline, how many omegas, how much B12, iodine, selenium…you’re getting to what the nutrient researchers show. So you can approach the question of optimum nutrition from a number of different directions – biochemistry and logic, evolution studies and so on.
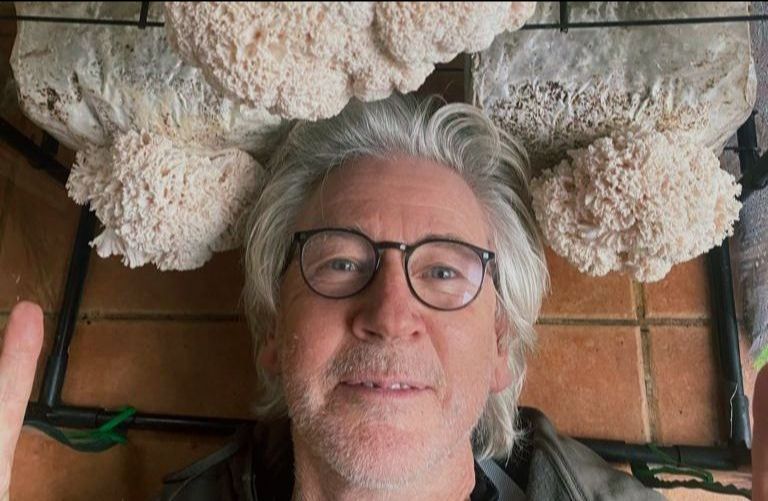
Patrick growing Lions Mane Mushroom.
SM: That is a great connection to make.
PH: I think that I’m just lucky, because I’m 66 and I’ve been studying since I was 18 or so, and a bit like you, there’s barely a day when you’re not reading some paper somewhere or learning something new. And also, because I’ve got my scientists on a network, they send me stuff.
Now you could have a 25-year-old, super bright, straight As and everything, and they have just not had the time to have absorbed all this material. That’s why I say I’m lucky. I’ve got “sensors” that ask “Does that really fit an evolutionary model? And this finding doesn’t really fit with this…”so when everything comes together, you feel very confident about it.
SM: One of the things that stops me writing more books is that I’m aware that as soon as I’ve written one, it’s out of date. You don’t seem to be bothered by that. You just do another book, I guess. Is that how you operate?
PH: The thought of going back and updating my books is a nightmare. Yes, I do it when I’m really embarrassed! I did it with my book on arthritis, and I did it with Improve your Digestion, but there’s not a lot that is “wrong”, it’s just that we discover new things. I’m looking at my book Say No to Cancer. Now, there are some seriously good books out there on cancer, but if someone’s been diagnosed with cancer, they’re in a state of fear and disempowerment. That book is actually empowering. Later on they can get into ketones and whatever, but some of the brilliant, detailed books – if you’ve got hold of that in your first two months of cancer, unless you happen to be that sort of person, you’d just be completely overwhelmed.
I guess if you’re writing books as encyclopaedias, it’s a problem, or is it something that opens up an area? So I’m not so worried about it, but you’re right. I mean, there’s so much stuff coming through, and you must feel quite overwhelmed at times. You do an incredible job making it accessible. I don’t know how you do it.
SM: Well thank you and back at you. As you know, you can be inundated with new material and some of it just “sticks” and you know it’s important and needs a follow-up. You can let the rest go. From your VERY aged perspective then, from the beginnings in the back room to ION and kick-starting a whole profession into existence, where do you think it’s going? What are we doing right? What are we doing wrong? Where would you steer us?
—
Not always the most popular opinions
PH: Funnily enough, in the time since I left ION, there are times when I’ve been flavour of the month, and times when I haven’t been…
SM: Well, that’s a very restrained frame for what the media and certain academics have put you through…
PH: I’ve taken the flack a few times, I think, for the profession. And at that time, most people flee, so you don’t generally get much support. So yes, there’s been a sort of nervousness around ION – for example, in relation to supplements, because of potential attacks or whatever. And I would just say to everyone to, as I do, always follow the logic, follow the science, and be bold and brave, because nutrition is always amazing. The power of nutrition is always amazing.
I love the way that ION has been run over the last several years. It’s really tough to run a charity, and it’s done very, very well.
My intention was simply that people would be really good at what they were doing, and if they were and got really good results, then they would get more clients. They would be successful. But there is still this disempowerment, where we look to the establishment. We want to be recognised by some authority, thus have our degree status or whatever. My personal view is that although that’s a very good thing, it’s secondary.
I believe ION was four times at the point of getting degree status without achieving it (it has now), usually because there are vested interests who do not want nutritional therapy to become mainstream. So there’s a debate as to what extent you change what you’re teaching and learning in order to get some accolade from the establishment, so to speak. And I would say, whatever happens we have to stick to our guns. We have to do what works. We have to do what the science shows. Be like those Vulcans: don’t be persuaded just by opinion.
—
Chromium, homocysteine and methylation
SM: Fads and fashions rather than fundamentals?
PH: I’ve been a little bit shocked, because I have interviewed various people qualified in nutrition for various jobs, and everyone has something to say about the microbiome right now. Yet it’s extraordinary how many know very little about homocysteine and methylation.
And then one of the questions I always ask when I’m interviewing various nutrition therapists in mental health is about the very good work on high-dose chromium being an effective antidepressant. That was shown by a brilliant psychoanalyst professor who had a patient who got better taking chromium, and not from psychoanalysis. So he set up a randomised, placebo-controlled trial. In other words, there are some learnings along the way and some things that have just been forgotten in nutritional therapy and functional medicine.
For example, you’ll find that the homocysteine-methylation thing is quite ignored in America, but not in Scandinavia, and it’s a bit more known in the UK. So you get these geographic differences. And things go into fashion, and then they go out of fashion.
An early influence: the ground-breaking book by Dr Carl Pfeiffer, famous for Pfeiffer’ Law: “For every drug that benefits a patient, there is a natural substance that can achieve the same effect”.
Founder of the Brain Bio Centre, he was one of the first physician-scientists to investigate the biochemical basis of mental disease.
“If there’s a drug that can alter the brain’s biochemistry, there’s usually a combination of nutrients that can achieve the same thing without side-effects”, he wrote.
So yes, I just say stick with the science. Stick with being highly confident in the effectiveness of optimum nutrition.
But then, I watch how it has evolved. It’s fantastic. I mean, it’s an established profession. I think BANT has done an incredible job.
You know, it’s a very active, vibrant and alive community. But one has to know that there are companies who make money because they have products, and they need new products, and they need new tests, and sometimes they have the money for the marketing and all the rest of it, which is fine, because it helps to support the whole industry in one way or another. But you must always have your BS detector turned fully on. Antennae on, not to just get sucked into the latest fad. For example, the blood sugar issue is vital, however you deal with it. The whole methylation-homocysteine thing is vital: I mean, David Smith’s paper showed homocysteine is a marker for more than 100 diseases.
SM: Yes, thanks to you we got that covered in IHCAN – it is a staggering piece of work.
PH: “It’s bigger than you think” sort of thing, right? And then fats are not just omega-3s. And vitamin D – which is a weird one, really, because we put it in the “fat-soluble vitamin” zone.
SM: Even although we should actually be treating it as a hormone…
PH: And even with vitamin D’s effect on COVID, we don’t really know why. It’s got so many potential genetic switches and all the rest of it. But no, I’ve tried to fit it in with the others. It doesn’t fit. And then there are the antioxidants and polyphenols – we finally got the glutathione index test up and running all over the place. That’s really a nice measure, because, you know, people like Dr Tom Levy say, it’s all about oxidation and antioxidants.
SM: So, back to fundamentals, and I know you see the future as “digital” – what does that mean for us?
PH: I worked out quite a few years ago that the only way to affect major change was that it had to be digital, it had to be international, and it had to change people’s behavior. It took a few years for others to buy into that, but then we did this crazy project with the cognitive function test. But almost every day we have 150 people take the test. We’re up to 450,000 people now. My goal is to have data on a million people, which makes us bigger than anything, bigger than UK Biobank, by the end of next year.
SM: So by “digital”, you mean you’ve got to use the internet, apps and tech, rather than flogging books from the back of your Skoda?
PH: Rather than just a book, yes. And I think, also, nutritional therapists have learned that only doing one-on-one consulting is not the way to go. The successful ones tend to have different routes to them – so coaching and sessions and a package that you buy into. And that comes from the whole concept of, how do I change a person’s behavior? If I see them once, and then a month later I see them again, and a month later I see them again – it’s very hard. So what’s the method that creates that behavioural shift?
For myself, I started doing three-day residential workshops called Total Health Transformation, where I saturated people completely in an environment where it wasn’t just nutrition, but if we learned something about food, we then cooked it together, and we’d eat it together.
So it’s how to wake someone up to actually do that. This is all part of ION, too, because it’s also when you realise that it’s not just what you know, but it’s knowing how you actually change behaviour.
So in the time when I was running it, we were learning a lot of psychological techniques, also marketing techniques, knowing that 80% of it was psychological and 20% was about the knowledge about nutrition.
The truth is that for 80% of people, it’s about some very simple things – the fundamentals that we mentioned: blood sugar, antioxidants, fats, methylation. Most problems can be solved with something that we could probably learn in a month or two, and it’s just those extra, difficult cases where you really have to go to a whole, other layer.
—
Future predictions
SM: You see things coming so what’s your prediction for the nutritional therapy profession? The NHS is permanently in crisis and yet many practitioners seem keen to get more involved with GPs and the whole system.
PH: My view is that the NHS-type, conventional medical system is beyond repair, and it will get worse and worse. It’s happening in every country. I also think that the pharmaceutical approach, although it still looks strong, is really, really weak. And we knew from ten years ago when Heather Stein of GSK said the only way they could sustain profits was not from blockbuster drugs, because they didn’t have any, but from vaccines.
Pharma holds up the whole broken system. And all our lovely doctors, like in the Public Health Collaboration, or all the fabulous GPs who are part of groups within the NHS trying to make change happen, say it’s like pulling teeth. It’s just so painful. So people are not getting better, so more and more people are going to look at “What’s my alternative?”, and our job is to provide that and make ourselves available in a way that is accessible, affordable and so on.
SM: What’s the best way to do that?
PH: The important thing is for us to be very good at what we’re doing. But again, I think practices need to go much more digital.
We are in a digital universe. 60% of access to everything is on a mobile device. And it’s no longer about what paper you read and what television program you watch. There’s much more influence these days through podcasts and YouTubes and social media. So it’s just simply understanding how to meet people’s needs – which they’re just not getting from their doctors.
Be available – whatever that means to you. With Zoom, for instance, we can reach people anywhere in the world, and with AI we can have instant translation, “speak” their language and understand them even if they don’t speak English.
We need to just stay on target: what is it we do that really works? What are people’s needs? How do we package what we are doing to be available to people? And people tell people.
The future is bright, because there’s no lack of supply of unhealthy people! It should be shrinking, but in most areas, it’s growing, and what treatment is available for them is less and less available. If we wind back 15 years, there were blockbuster drugs that were very sexy, and now there aren’t. So our area is getting very messy and no one wants to wait a month to see their GP and then get referred, and then have to wait again for something that’s probably not going to work anyway. Whatever they’re talking about doing with the NHS, it’s just so slow and it’s probably just not going to happen.
SM: So 1978, I’m at Here’s Health, you’re at Green Farm and what are we talking about? Get people to stop eating junk food. Fast forward 46 years and what’s the hot topic? Ultra-processed food. It’s bad for you, apparently. Who knew? It’s frustrating, isn’t it?
PH: I went to one of the Public Health Collaboration conferences, maybe three years ago, and they’d have patient cases up, and for everyone, the answer was a sort of low glycemic load and sort of keto diet. And that was the answer for everything they wanted. Very, very exciting. I was so glad to be hearing this, a bunch of fantastic doctors saying this. But the other side of this is that I was saying this in the 1980s.
SM: Exactly. And did you get credit for it? No.
PH: And the other thing is at this conference, there wasn’t a single mention of micronutrient supplements. Well, there was a talk about the need for “proper studies” where you get a drop in the HbA1C in randomised trials and meta- analyses. And I raised my hand and said, “You know, there have been 28 randomised control trials on chromium that have been meta-analysed, and lowered HbA1C by the amount you’re talking about. Is there any chance, maybe next year, we’ll chat about micronutrients?”
So more and more doctors waking up to low-carb, and in this first wave it’s also no pills or fewer drugs, which is fantastic but the medical profession is still paranoid about nutrient supplementation. And we know that what actually works is to both change the diet and supplement the right nutrients. And that is orthomolecular medicine, that is optimum nutrition, that is functional medicine.
SM: So we have doctors turning on to diet and nutrition, but they won’t do supplements, so we are still about ten years ahead and able to provide science-based recommendations that the public just won’t get anywhere else.
PH: Yes, and this paranoia towards supplements is illustrated by the Lancet Commission totally ignoring homocysteine despite all the evidence because the solution is a supplement.
It also tells you that if you have a Prof Tim Spector or Dr Chris van Tulleken, anyone who comes through has got to nutrition through a medical route. They’ve had implanted in their DNA an anti-supplement bias. And you know, they’re just not processing science. That’s the point. So we have to stick to the science, be confident in the evolution of nutrition and conditions of existence, and just get good at changing people, which means coaching to facilitate behaviour change. We have to empower people because the only person who can change you is you.
—
Actions:
Join COGNITION by becoming a FRIEND to get access to a personalised 6-month program to upgrade your brain
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
It’s been an incredible year for our small charity, which has experienced an amazing growth spurt—expanding tenfold in just two years!
Reaching and helping millions of people to dementia-proof their diet and lifestyle through over 80 seminars, webinars, TV and radio interviews and podcasts worldwide.
—
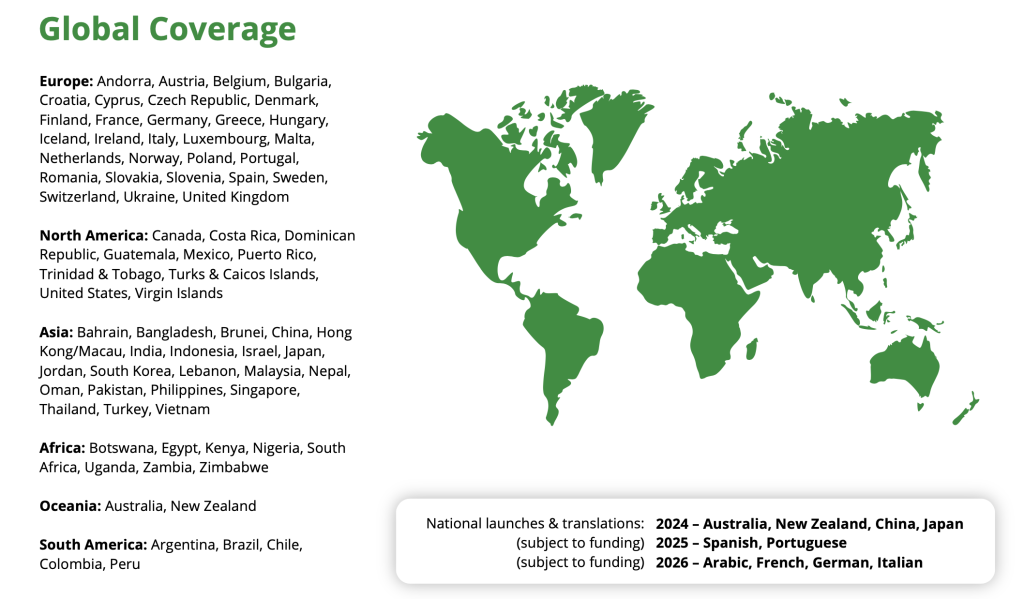
Going global with COGNITION!
Personally, I am exhausted and with my last burst of energy, I headed off to the Far East – China and Japan for the whole of November – to launch the translated Cognitive Function Test to up to 18 million people. Then I’ll collapse on a beach somewhere in Thailand before returning for Christmas!
—
New faces to the small but mighty team!
Meanwhile, we have appointed the wonderful Emma George, a naturopath and experienced project manager, as Managing Director. Emma will take over as CEO in January giving me more time to teach and reach influential groups of people to ‘Upgrade Your Brain’. Emma is supported by an amazing team of highly skilled and committed people. It’s the teamwork that makes the dream work – the shared dream of Food for the Brain, which is educating and empowering people to take control of their mental health.
—
Emma George is an accomplished leader with over 20 years of experience in organisational development, health, and wellbeing. As current Managing Director of the Food for the Brain Foundation, Emma brings her expertise in strategic planning, stakeholder engagement, and project delivery to drive Food for the Brain’s mission of promoting cognitive health through nutrition and lifestyle interventions.
Emma’s career highlights include leading national and European health projects, such as the Welsh Government’s Healthy Working Wales scheme, where she directed a team to assess and enhance workplace health initiatives across the nation. When not at work, Emma enjoys engaging with community projects, and teaching at the School of Naturopathic Nutrition, reflecting her dedication to creating a healthier future for all.
—
Most of the Team in Wales this Summer.
—
The largest independent COGNITION Biobank – research with no profit motive!
None of this could have happened without you, our Citizen Scientists and of course our Friends of Food for the Brain who are 2000+ strong.
It’s because of your willingness to take the test, and share your data (anonymously) that has helped create the largest independent COGNITION Biobank research database and enable real research to help people without a profit motive.
If you haven’t become a FRIEND yet then please do so here. We are completely independent so each FRIEND is helping us make a difference in the world!
—
“I became a FRIEND and joined COGNITION last September because my memory was terrible! My Dementia Risk Index has gone down from a start point of 52.35 to 37.45%! My weight was 12st 2lbs and is now 10st 11 lbs and I’ve really got a handle on keeping sugar intake very low. I have 4 green areas now and I’m very excited about getting my life back and could never have achieved it without the COGNITION Programme.” Janette, 68
—
Want to make a larger donation to help our Smart Kids Programme?
If you’d like to become involved in this radical research revolution, beyond being a FRIEND, email Fran, Head of Donations & Engagement at donations@foodforthebrain. Currently, we need funds to help finish building COGNITION for Smart Kids through the SPONSA Donna campaign.
Meanwhile, as the Festive Season approaches, we have quite a few exciting things coming your way:
What’s happening this Christmas at Food for the Brain?
The Christmas DRIfT 4 in 1 discount! Get your family or community to become Citizen Science researchers this festive season – order the test kit here and use code XMAS10 to save 10% internationally.
Looking for a stocking filler? Then the Upgrade Your Brain Book is the perfect gift – order here.
For test kits and the book, order before 16th December for Christmas delivery
Thank you for reading!
Food for the Brain is a not-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
(Originally posted in IHCAN magazine. Written by Patrick Holford, edited by Carol Ludlam)
What is really going on as we age? What contributes to the wrinkles, stiffer joints, slower cognitive function and other health problems?
It begins with the brain.
Your brain consumes more energy than any other organ, burning either glucose or ketones. This combustion creates oxidants that age your brain. The ability to rapidly extinguish these oxidants, which ultimately age your brain and body, is what helps you live longer with less wrinkles, more flexible joints, healthier blood vessels and organs, especially your brain, which has 400 miles of blood vessels.
—
Top level prevention factors
Keeping oxidants down is perhaps the single most important thing you can do for vascular health. Vascular dementia, for example, is strongly associated with the amount of oxidation, determined by antioxidant intake from fruit and vegetables on the one side and smoking and pollution for example, on the other. Those in the top quarter of Total Antioxidant Capacity (TAC) in their diet halve their risk, in a study of 2,716 people over age 60 (1).
Additionally, critical antioxidants such as vitamin C and vitamin E, if supplemented together, reduced the risk of developing Alzheimer’s by as much as two-thirds, whilst taking either cut risk by a quarter in a study of 4,740 elderly residents of Cache County, Utah (2). Another study shows that ‘either a high vitamin E or C intake showed a trend of attenuating risk by about 26 per cent’, according to China’s leading prevention expert Professor Jin Tai Yu of Fudan University in Shanghai, making these nutrients ‘grade 1’ top level prevention factors (3).
Vitamin C, which is water based and protects you against smoke and pollution, and vitamin E, which is fat based and protects you from burnt and fried fats, including sunburn, are in the bloodstream outside of cells. Inside cells, especially brain cells, is the most potent antioxidant of all, which is glutathione.
—
Glutathione is the Master Intracellular Antioxidant
Nutritionists have been measuring red cell glutathione (GSH) for decades as an indicator of a person’s antioxidant capacity. GSH is the most important antioxidant and free radical scavenger that is found to be decreased in the brains of people with a wide range of mental and neurological illnesses from schizophrenia (4) to dementia (5, 6).
However, the problem with just measuring glutathione is two-fold. Firstly, since it oxidises so rapidly, it has to be ‘fixed’ immediately to avoid any degradation to its oxidised form glutathione disulfide (GSSG). Testing of glutathione levels is therefore usually dependent on going to a lab for blood to be drawn and then immediately tested or fixed, to limit any oxidation. The reliability of glutathione measurements, unless done under strictly controlled conditions such as these, may be questionable due to the rapid oxidation once blood is taken.
—
The Glutathione Index (GSH/GSSG) is the best measure of antioxidant status
Additionally, it is the amount of ‘spent’ or oxidised glutathione (GSSG) that reflects the extent of oxidative stress a person is under. Think of glutathione as the water in the fire engine. It gets rapidly used up keeping your brain protected. The ‘spent’ or oxidised glutathione (GSSG), much like steam, then has to be cooled to reload the fire engine. This recycling is done by vitamin C and an enzyme called Glutathione Reductase (GR), returning Glutathione back to its fully loaded ‘reduced’ form. Another enzyme, Glutathione Peroxidase (GP), is involved. GR is riboflavin (vitamin B2) dependent and GP is selenium dependent.
Dr Konrad Kowalski, the Food for the Brain’s analytic chemist, explains: “Reductions in GR enzyme levels in patients with dementia are well established. GR levels alone are therefore a fairly good biomarker of dementia.” However, the mere presence of the enzyme does not guarantee its high activity. GR needs to consume NADP molecules to function properly. As shown by Irene Martinez de Toda et al 2019 data, patients with dementia have a reduction in both the enzymes (GR and GP) that recycle glutathione. Thus, in general it can be said that the glutathione metabolism (recycling) loop in those with dementia ‘spins’ much slower than in healthy patients.
“The advantage of our measurement of the Glutathione Index (GSH/GSSG) is therefore, that it shows changes in GR activity, not only due to higher/lower GR gene activity but also due to the absence of the reaction cofactor NADP.”
“As a result, dementia patients have a lower potential to dynamically fight free radicals and will have a worse GSH/GSSG, which we call the Glutathione Index (7). The worse the ratio the worse a person’s cognitive function is likely to be. It’s a bit like having a direct measure of how fast your brain is ageing. Patients with dementia have a reduction in glutathione and its ability to be recycled (8). This ratio, the Glutathione Index, is a biomarker for many diseases, including both type 1 and 2 diabetes, liver cirrhosis, multiple sclerosis and Alzheimer’s disease.” says Dr Konrad Kowalski, who has developed this test for us.
One of the biggest challenges in developing the Glutathione Index, which is a home test kit involving a pin prick of blood dripped onto a dry blood spot card, is that the conventional DBS cards didn’t provide enough stability for the rapidly oxidising GSH, so we developed a method that instantly ‘fixes’ the sample for a guaranteed 12 week stability from taking the sample.
The red arrows indicate reduced or increased activity in dementia patients
So we want people to both measure their Glutathione Index and complete our validated Cognitive Function Test along with the follow-on Dementia Risk Index questionnaire, which calculates an ‘antioxidant’ domain score.
As a result of our research where we have tracked these against the person’s blood level of Glutathione Index, enabling us to establish what an optimal level is. This means those boundaries, which we show in colours from green (good), yellow (OK), orange (not good), red (bad) will evolve and become more accurate thanks to you and people like you.
We now know that a desirable level is above 800. Below 500 is an indicator that you need to increase your intake of antioxidants from food and/or supplements, and/or reduce your intake of oxidants from smoking, pollution or fried food. Glutathione is related to the pace of aging and the activity of antioxidant enzymes which are depleted in those with cognition decline. It is also part of your DRIfT (Dementia Risk Index functional Test) score.
This is unique and vital research funded by the people for the people – Citizen Scientists.
—
—
How Glutathione and vitamin C recycle each other
Vitamin C helps ‘reload’ glutathione and glutathione helps reload vitamin C as you’ll see in the figures below. This glutathione – vitamin C cycle is one of the hottest discoveries in anti-ageing science. You’ll see that NADPH, derived from niacin (vitamin B3) and its cousin NAD are involved. Co-enzyme Q10 in its reduced form ubiquinol is also involved and although not shown in this diagram, low levels are also found in those with Alzheimer’s (9).
—
Raising glutathione – the role of NAC
Nutritional therapists have been measuring red cell glutathione and supplementing glutathione or its precursor N-Acetyl-Cysteine (NAC) for decades. However oral GSH supplementation has poor bioavailability largely because it is so rapidly oxidised to GSSG as it disarms free radicals. N-Acetyl Cysteine (NAC), a precursor of glutathione, is therefore often used instead and has been shown to successfully raise plasma glutathione levels, for example, in those with schizophrenia. Anthocyanins also recycle glutathione thus sparing it if supplemented together (12).
NAC has plenty of evidence to support its use as a promoter of glutathione and mental health, thus reducing the brain’s oxidative stress. The latest 2022 review states: “N-acetyl-L-cysteine (NAC) is a compound of increasing interest in the treatment of psychiatric disorders. Primarily through its antioxidant, anti-inflammatory, and glutamate modulation activity, NAC has been investigated in the treatment of neurodevelopmental disorders, schizophrenia spectrum disorders, bipolar-related disorders, depressive disorders, anxiety disorders, obsessive compulsive-related disorders, substance-use disorders, neurocognitive disorders, and chronic pain. Currently NAC has the most evidence of having a beneficial effect as an adjuvant agent in the negative symptoms of schizophrenia, severe autism, depression, and obsessive compulsive and related disorders.” (13) For example a large RCT of 140 participants observed significant improvements on global symptomatology, and general and negative symptoms of schizophrenia in the NAC supplementation (2 g/d; in addition to anti-psychotic medication) group in comparison to the placebo group over a 24 week period (14).
According to Dr Chris Palmer, assistant professor at Harvard Medical School, “Glutathione (GSH), the brain’s primary antioxidant, plays a crucial role in maintaining redox balance (the process of maintaining the balance of reactive oxygen and nitrogen species in cells to maintain homeostasis) . Magnetic resonance studies have provided mixed results regarding GSH levels in schizophrenia patients, with some studies indicating decreased levels in chronic schizophrenia, while others found no significant differences. However, these inconsistencies may be due to variations in disease chronicity, age, and symptom severity among study participants. The findings from these studies suggest several potential therapeutic targets for schizophrenia. Addressing mitochondrial dysfunction, redox imbalance, and impaired energy metabolism could lead to more effective treatments. For instance, N-acetylcysteine (NAC), a precursor to GSH, has shown promise in increasing brain GSH levels and improving symptoms in first episode psychosis patients.”
NAC is so medically effective that it has been classified a medicine, hence not a food, and is no longer available over the counter in the US.
Our Glutathione Index test costs £69 – order it and be a part of this new exciting research, whilst learning how you can protect and upgrade your brain.
It is also available as part of their 5-in-1 DRIfT test also measuring Homocysteine, HbA1c, vitamin D and Omega-3 Index.
—
Actions
Join COGNITION by becoming a FRIEND to get access to a personalised 6-month program to upgrade your brain
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
References
1 Peng, M., et al. Dietary Total Antioxidant Capacity and Cognitive Function in Older Adults. J Nutr Health Aging (2023).
2 Basambombo LL, Carmichael PH, Côté S, Laurin D. Use of Vitamin E and C Supplements for the Prevention of Cognitive Decline. Ann Pharmacother. 2017 Feb;51(2):118-124. doi: 10.1177/1060028016673072. Epub 2016 Oct 5. PMID: 27708183.
3 Yu JT, Xu W, Tan CC, Andrieu S, Suckling J, Evangelou E, Pan A, Zhang C, Jia J, Feng L, Kua EH, Wang YJ, Wang HF, Tan MS, Li JQ, Hou XH, Wan Y, Tan L, Mok V, Tan L, Dong Q, Touchon J, Gauthier S, Aisen PS, Vellas B. Evidence-based prevention of Alzheimer’s disease: systematic review and meta-analysis of 243 observational prospective studies and 153 randomised controlled trials. J Neurol Neurosurg Psychiatry. 2020 Nov;91(11):1201-1209. doi: 10.1136/jnnp-2019-321913. Epub 2020 Jul 20. PMID: 32690803; PMCID: PMC7569385.
4 Yao JK, Leonard S, Reddy R: Altered glutathione redox state in schizophrenia. Dis Markers 2006, 22(1):83–93 ; see also Gawryluk JW, Wang J-F, Andreazza AC, Shao L, Young LT: Decreased levels of glutathione, the major brain antioxidant, in post-mortem prefrontal cortex from patients with psychiatric disorders. Int J Neuropsychopharmacol 2011, 14(01):123–130.
5 Torres LL, Quaglio NB, de Souza GT, Garcia RT, Dati LM, Moreira WL, Loureiro AP, de Souza-Talarico JN, Smid J, Porto CS, Bottino CM, Nitrini R, Barros SB, Camarini R, Marcourakis T. Peripheral oxidative stress biomarkers in mild cognitive impairment and Alzheimer’s disease. J Alzheimers Dis. 2011;26(1):59-68. doi: 10.3233/JAD-2011-110284. PMID: 21593563
6 Park SA, Byeon G, Jhoo JH, Kim HC, Lim MN, Jang JW, Bae JB, Han JW, Kim TH, Kwak KP, Kim BJ, Kim SG, Kim JL, Moon SW, Park JH, Ryu SH, Youn JC, Lee DW, Lee SB, Lee JJ, Lee DY, Kim KW. A Preliminary Study on the Potential Protective Role of the Antioxidative Stress Markers of Cognitive Impairment: Glutathione and Glutathione Reductase. Clin Psychopharmacol Neurosci. 2023 Nov 30;21(4):758-768. doi: 10.9758/cpn.23.1053. Epub 2023 Jul 14. PMID: 37859449; PMCID: PMC10591176.
7 Park SA, Byeon G, Jhoo JH, Kim HC, Lim MN, Jang JW, Bae JB, Han JW, Kim TH, Kwak KP, Kim BJ, Kim SG, Kim JL, Moon SW, Park JH, Ryu SH, Youn JC, Lee DW, Lee SB, Lee JJ, Lee DY, Kim KW. A Preliminary Study on the Potential Protective Role of the Antioxidative Stress Markers of Cognitive Impairment: Glutathione and Glutathione Reductase. Clin Psychopharmacol Neurosci. 2023 Nov 30;21(4):758-768. doi: 10.9758/cpn.23.1053. Epub 2023 Jul 14. PMID: 37859449; PMCID: PMC10591176.
8 Martínez de Toda I, Miguélez L, Vida C, Carro E, De la Fuente M. Altered Redox State in Whole Blood Cells from Patients with Mild Cognitive Impairment and Alzheimer’s Disease. J Alzheimers Dis. 2019;71(1):153-163. doi: 10.3233/JAD-190198. PMID: 31356205.
9 J. Frontiñán-Rubio et al. Molecular and Cellular Neuroscience 92 (2018
10 Witschi A, Reddy S, Stofer B, Lauterburg B: The systemic availability of oral glutathione. Eur J Clin Pharmacol 1992, 43(6):667–669.
11 Lavoie S, Murray MM, Deppen P, Knyazeva MG, Berk M, Boulat O, Bovet P, Bush AI, Conus P, Copolov D, Fornari E, Meuli R, Solida A, Vianin P, Cuénod M, Buclin T, Do KQ: Glutathione precursor, N-acetyl-cysteine, improves mismatch negativity in schizophrenia patients. Neuropsychopharmacology 2008, 33(9):2187–2199.
12 Ohlenschlager G,Treusch G, patent number: 5925620 International Classification A61K 3800 for synergistic action of anthocyanidins and glutathione
13 Bradlow RCJ, Berk M, Kalivas PW, Back SE, Kanaan RA. The Potential of N-Acetyl-L-Cysteine (NAC) in the Treatment of Psychiatric Disorders. CNS Drugs. 2022 May;36(5):451-482. doi: 10.1007/s40263-022-00907-3. Epub 2022 Mar 22. Erratum in: CNS Drugs. 2022 Apr 28;: PMID: 35316513; PMCID: PMC9095537.
14 Berk M, Copolov D, Dean O, Lu K, Jeavons S, Schapkaitz I, Anderson-Hunt M, Judd F, Katz F, Katz P, Ording-Jespersen S, Little J, Conus P, Cuenod M, Do KQ, Busha AI: N- acetyl cysteine as a glutathione precursor for schizophrenia—a double-blind, randomized, placebo-controlled trial. Biol Psychiatry 2008, 64(5):361–368.
If you think that Alzheimer’s or dementia is caused by amyloid plaques in the brain, or tangles of nerves (called neurofibrilliary tangles) associated with p-tau, you have been successfully conned.
But you would not be alone.
There is a vast sleight of hand going on that remarkably continues to hijack research into true causes and potential cures for Alzheimer’s despite a mountain of evidence to the contrary.
How did this all start…
Let’s start at the beginning. Some people get increasingly severe cognitive decline. This affects about one in ten older people. We call this dementia. Some people with dementia, on scanning their brains, have big gaps in the central part of the brain, which is used to diagnose that dementia as Alzheimer’s disease due to the clear evidence of ‘pathology’ – something wrong in the brain that amounts to death of significant amounts of brain cells in critical areas. So, here we have two clear diagnostic criteria: Firstly, a loss of cognitive function which is what we test at foodforthebrain.org with our Cognitive Function test. Secondly, a loss of actual brain, which is diagnosed by a type of brain scan of the central or medial part of the brain which was first developed by the team at Oxford University, headed by Professor David Smith, a member of our Scientific Advisory Board.
—
What causes Alzheimer’s?
So, then the question is what causes it? There is no evidence, that it is caused by deposits of amyloid protein or amyloid plaque, in the brain. About 30% of older people have plaques in their brains without dementia. About 15% of those with dementia don’t have amyloid plaques. Having amyloid plaques doesn’t cause dementia. Mice with amyloid plaques behave normally. Even a head full of plaques only results in mild memory problems. Many of us have plaques in our brain and remain completely healthy.
What happens if you ‘treat’ amyloid plaques? Blocking the enzymes that make amyloid have made people worse, not better, despite lessening the amyloid burden. Vaccinating animals to remove the plaques doesn’t change anything to do with dementia, but it does reduce the amyloid. The anti-amyloid vaccine injections in humans have been equally ineffective despite lowering the amyloid burden in the brains of those injected.
The pharmaceutical companies running these failed trials have pushed and pushed until they could just about get a significant difference in the rate of degeneration of patients versus placebo on questionnaires equivalent to less than half a point change on an 18 point scale. No-one got better. Quite a few got worse, with brain bleeding and swelling. A few died as a consequence. But still drug agencies, paid for by the drug industry, dished out licences. In the UK the watchdog NICE said the evidence wasn’t good enough and recommended the National Health Service not to give anti-amyloid treatment – at about £50,000 a patient per year.
In scientific terms the trials added evidence to the mountain already existing that amyloid deposits don’t cause Alzheimer’s because lowering it doesn’t stop the disease process, doesn’t improve cognitive powers in any meaningful way and doesn’t slow down brain shrinkage. In fact, if anything, it accelerates the main physical measure of brain shrinkage. In the last anti-amyloid trial, donanemab, those on the amyloid treatment had considerably more brain shrinkage than those on the placebo.
—
The unhealthy obsession
You would think that the whole field would get the message by now, stop funding this dead end and explore other avenues. But they were so hoping and invested in the ‘amyloid cascade hypothesis’ that no-one could give up. It’s become an unhealthy obsession.
In the US the Alzheimer’s Association and in the UK the Alzheimer’s Society supported this line of thinking and continue to do so. ‘We are most proud of our contribution to amyloid’, declares the research director of the Alzheimer’s Society.
Why don’t they explore other avenues? It’s partly to do with money. No-one can get research money if they’re not looking at amyloid (or p-tau – more on this in a minute.)
In the UK the Medical Research Council continue to pour good money after bad by making another £20 million available for drug trials. That’s taxpayer’s money backing the wrong horse despite a lousy track record. In the US the National Institutes of Health and the National Institutes of Aging spend vast sums pushing in this fruitless direction. Big pharma spend twice as much as the charities, funded by us taxpayers – probably around $150 billion so far. So, perhaps $250 billion has been spent getting almost nowhere. Sure, we know a lot more about amyloid and tau but are no closer to a ‘cure’.
—
Can you claim to find a cure when you don’t know the cause?
Getting the James Webb telescope into space cost $8 billion. Here we are having spent considerably more than thirty times this and we haven’t even got lift off. I remember when, at the G8 Summit in London in 2013 pharma-funded scientists said ‘within ten years we’ll have a cure. This month, listening to the BBC Radio 4’s ‘Inside Health’ programme on Alzheimer’s, they said exactly the same thing – that magical ten years from now. How can you claim you’ll have a cure when you don’t even know the cause? I predict we’ll be in the same place in ten years if the Alzheimer’s industry don’t quit on amyloid and p-tau.
But it gets worse than this. Despite nothing but evidence to the contrary, based on the completely false notion that ‘Alzheimer’s IS amyloid’ we are being told an amyloid blood test is around the corner. In other words, if you have amyloid blood test but feel completely normal, you’ll likely be told you have ‘pre-clinical Alzheimer’s’ just waiting to happen despite a third of those with amyloid plaques having no problem at all! That’s a conflation upon a conflation.
All this is laid out beautifully in a book by Karl Herrup – Professor of Neurobiology and Investigator at the Alzheimer’s Disease Research Centre at the University of Pittsburg, called How NOT to study a disease – The Story of Alzheimer’s. If you don’t believe what I’m saying, or rightly question it, please read this book. You can find it in our online Bookstore here.
But, so desperate is the medical-pharmaceutical industry to find a treatment and make money that it just can’t give up. It reminds me of the story of Mullah Nasrudin, who is looking at the illuminated ground under a lamp-post. A passer by says ‘what are you looking for?’ The Mullah says ‘I dropped a coin.’ The person says ‘did you drop it around here?’ The Mullah said ‘no, but it’s the only place I can see’.
—
Amyloid does increase the PROBABILITY of getting Alzheimer’s in the future but it doesn’t cause it.
But let’s be clear. This doesn’t mean that having lots of amyloid in your brain doesn’t increase the PROBABILITY of getting Alzheimer’s in the future in much the way that being older also increases the probability of getting Alzheimer’s. But it doesn’t cause it. So ‘curing’ amyloid won’t cure the disease. If you ‘exist for a cure’, as one charity claims, you have a start with a clue as to what’s causing it. Obviously not amyloid.
The same thing is happening with another ‘marker’ in the brain called p-tau, which is associated with having more tangled nerves. Tau is a normal protein that becomes an abnormal, toxic protein called p-tau. The ‘p’ stands for phosphorus or ‘phosphorylated’ because there’s an enzyme that adds on the ‘p’ and another that takes it away. Much like amyloid, having more p-tau increases the PROBABILITY of Alzheimer’s but doesn’t cause it. Many people have raised levels of p-tau (we all have some) with no problems at all.
But, by using the same sleight of hand, £10 million has been put up by the Bill Gates Foundation and people funding Alzheimer’s Research UK, to find the blood test for p-tau (I think they’ve already decided on one called p-tau 217) despite no evidence that p-tau CAUSES Alzheimer’s. No doubt, those with raised p-tau 217 will be told they have ‘pre-clinical dementia’ despite no evidence that they do. Of course, if they had a p-tau lowering drug that actually worked as in reducing dementia risk, that might be excusable but they don’t. However, this sleight of hand may be used to sell drugs that don’t work much like ‘cholesterol’ has been used to sell statins.
My cholesterol is slightly high – I have no disease, no risk factors for heart disease, and there is no evidence that lowering my cholesterol will lower my future risk, but still my doctor wants to prescribe me statins. In any case – two thirds of heart attacks in older people are predicted by high homocysteine – not cholesterol.
The only thing I know that does lower p-tau is lowering homocysteine with B vitamins. Homocysteine, a toxic amino acid also found in those with Alzheimer’s and dementia, promote the enzyme that makes p-tau and blocks the enzyme that clears it from your brain as the diagram below shows.
However, talking of homocysteine, it, unlike amyloid and p-tau, is actually causal. That is, lowering homocysteine with B vitamins, stops the accelerated brain shrinkage, stops the cognitive decline and memory loss. That is consistent with a disease-modifying treatment and possibly the only thing for which the evidence could be said to be causal at this point in time.
That doesn’t mean there won’t be other causes. There are some fruitful avenues that have been explored and show real promise. But they have all largely been ignored because of the unhealthy obsession by pharma, the Alzheimer’s societies and government funding bodies on amyloid and tau. These include oxidation – and the role of antioxidants; inflammation; insulin resistance and glucose control; mitochondrial dysfunction – those are the so-called ‘energy’ factories inside every brain cell. Diabetes and dementia are strongly linked, the first often predicting the second. In truth, both homocysteine, which is a measure of a vital process called methylation, oxidation, insulin resistance and inflammation all affect the mitochondria. One clue for inflammation being involved relates to the finding that those with rheumatoid arthritis using heavy duty anti-inflammatory drugs having less risk for Alzheimer’s. In our model of dementia at Food for the Brain glycation, oxidation, methylation and also the vital role of brain fats which actually build the brain are central. I call them the ‘four horsemen of the mental health apocalypse’. The discovery that the homocysteine lowering B vitamins and omega-3 are co-dependent and, together, dramatically slow brain shrinkage and improve cognitive function light years ahead of ANY amyloid or p-tau treatment to date, is of major importance. Yet, this has been largely ignored by the blinkered Alzheimer’s establishment.
So, next time you are asked to donate to Alzheimer’s charities ask them if any of the money is being spent on amyloid or p-tau. If so, I’d suggest politely declining. If instead they are funding research into oxidation, inflammation, homocysteine, insulin or mitochondrial function, then that’s a much better sign your money might not go down a black hole.
—
Is Alzheimer’s prevention the cure?
But even just focusing on one of these avenues may be misguided. It is based on the current paradigm of medical research – find the thing that is causing the disease then ‘cure’ that. This assumes there is one cause and therefore one treatment. Of course, this is what you need for a drug to make money.
Let’s take homocysteine as an example. Not everyone who develops dementia or Alzheimer’s has high homocysteine. Those who do will reliably develop dementia and lowering it reliably reduces their cognitive decline. So, high homocysteine is a CAUSE, but not the only cause. Insulin resistance leads to diabetes and increases the risk for dementia. So, insulin resistance driven by too much sugar and refined carbohydrates is probably a cause, but not the only one. There isn’t enough evidence yet to declare ‘cause’ but the evidence that exists points that way.
There is a different way of thinking and researching called system-based science. Much like the straw that breaks the camel’s back this approach presumes there are a number of conditions, not just one, that result in a disease such as Alzheimer’s or dementia. After all, a stroke or head injury can be a cause of cognitive decline even if you don’t have high homocysteine or blood sugar problems. (It could be that a potential causal mechanism that ties these together is cerebrovascular dysfunction – disturbed blood supply to the brain. High homocysteine, by the way, increases risk of this by 17-fold).
In my book Upgrade Your Brain, which gives all the reference studies for statements made in this article, I argue that every known risk factor or biomarker for cognitive decline, dementia or Alzheimer’s affects either the structure, the function or the utilisation of the neuronal network and that it is combinations of these that crank up risk and ultimately brain pathology. We will publish a paper on this soon in a scientific journal.
It’s like saying five critical things have to work for your car to move forward and not crash. Tyre pressure good, brakes working, enough gas, oil and water for the radiator to cool the engine. If any one of these is completely broken the car stops or crashes. If two are not working well, such as low oil and low water, the car grinds to a halt. If a car approaches too close (like a potential head injury) and one tyre is quite flat and the brakes aren’t working well, you crash.
We tend to think in this way in nutrition and lifestyle medicine. It’s the combo of insults – high sugar, high fried foods, lack of veg, too much alcohol, smoking, that breaks the camel’s back. That heart attack is the ‘perfect storm’ of several underlying factors.
—
The (unpopular) system-based approach
This systems-based approach isn’t popular in science and very few funders ever put up money to fund this kind of research. Usually, a funder wants to fund one stream of research, possibly a clinical trial of one approach, in the belief that that one factor is the final straw that breaks the camel’s back and a great discovery will be made. The reality is that it is usually combinations of factors that drive risk with the manifestation of the disease itself being the ‘broken back’. Pollution, for example, is a risk factor for dementia…but not in those with good vitamin B6, folate or B12 status, which are the three B vitamins needed for methylation, indicated by lower homocysteine. Methylation is a major mechanism the body uses to detoxify pollutants and toxins.
This is where Food for the Brain’s approach is unique.
By collecting data from people like you who have both taken the Cognitive Function Test and completed the COGNITION questionnaire, and keep doing so, we can look at what drives cognitive function up and down. In other words what breaks the camel’s back or makes it strong. This kind of complex systems-based science has become possible both due to big data gathering such as we are doing, advances in complex statistics, computer power and programming AI algorithms. Our Head of Science, Associate Professor Tommy Wood, is a bit of an expert in this kind of approach to neuroscience.
It is, I believe, the future and why we will probably find no single primary cause for Alzheimer’s, and certainly not amyloid or p-tau, but combinations of diet and lifestyle and other factors that create the tipping point that leads to dementia. Then, we will have the means to prevent this tipping point from ever being reached. In other words, we may discover that prevention is the cure. We hope that you’ll be part of this discovery. By becoming a FRIEND or making a DONATION you help us research what really causes, and prevents Alzheimer’s.
Similarly, if you’re inspired by our mission and would like to support groundbreaking research into the prevention and early detection of cognitive decline, consider investing in the global COGNITION Biobank project. Your contribution will help drive transformative research and create lasting change. To learn more, email us at donations@foodforthebrain.org
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
Why too much fructose is driving dementia, diabetes and brain fog
—
The fruit sugar ‘fructose’ isn’t generally considered a food that’s best avoided. After all, it comes from fruit.
Yet a radical new theory, developed by Richard Johnson, Professor of Nephrology at the University of Colorado, explains how it can trigger various damaging changes in our metabolism that make us more likely to develop chronic conditions such as diabetes, obesity and Alzheimer’s. If doctors better understood this, it could transform the new emphasis on sickness prevention that the government is promising.
—
The science of being ‘fructed’
Professor Johnson has produced what is effectively a biochemical wiring diagram of the connections which fructose turns on and off, that are making an increasing number of people sick. Fructose makes up half of white sugar and most of fructose corn syrup which is the main sweetener in fizzy drinks and ultra-processed foods as well as being the main sugar in fruit, particularly fruit juice.
For instance, the amount of fat stored in the liver increases, driving fatty liver disease, while the cell’s mitochondria, which create the body and brain’s energy molecule ATP, become less productive and blood pressure goes up. The result is that you get fatter, with more brain fog and fatigue and feel less inclined to exercise. Fructose is also a major promoter of diabetes.
Meanwhile an anti-ageing process called autophagy, which would normally clear away used up and damaged mitochondria, the cell’s energy factories, to make room for new ones, is disabled. When fructose crosses the blood-brain barrier into the brain, it is one of the factors causing the brain to form the clumps of amyloid protein found in Alzheimer’s, which is the focus of new drug treatments.
Why on earth does fructose carry out such a blitz on our bodies? Why would the body run a programme that was potentially so lethal?
“It would be wrong to think of fructose as some sort of major toxin, although it becomes neurotoxic in excess,” says Professor Johnson. “Instead, its remarkable range of effects are part of an ancient set of biological programs, which we call the ‘Survival Switch’, that work to prepare animals for hibernation, storing supplies in preparation for times of famine.” This is why fat storage increases and energy drops off producing brain fog. The trouble is we never run out of food or fructose in our modern times.
—
Eat your fruit, don’t drink it.
None of this means that we should avoid fruits, which contain only a small amount of fructose that comes with beneficial fibre that feeds our vital gut bacteria, plus various nutrients. Not so for fruit juice, devoid of fibre. A glass of orange juice is the equivalent of three oranges in terms of fructose, but without the fibre. So, eat your fruit, don’t drink it.
But this does explain why too much blood glucose from regularly eating generous amounts of sugar-laden foods and carbohydrates, is so damaging? The liver turns the excess glucose into fructose with all its knock-on effects. Other substances that can accelerate fructose production are alcohol and salt.
This rise in fructose intake and its presence in processed food makes it all too easy to start piling on the pounds, regardless of how many calories you have cut or how much further you are running. It’s a connection that very few nutritionists or GPs are aware of.
A sign of the widespread damage the Survival Switch can cause is that there are low ATP levels in the brains of people with disorders such as obesity, diabetes, fatty liver disease and Alzheimer’s. Understanding this points to new ways to cut the risks of these chronic disorders. Adenosine triphosphate (ATP) is a molecule that stores and provides energy for cells. It’s a key biomolecule that’s involved in almost all cellular processes.
A simple, but very effective solution, is to run a blood test – HbA1c – the gold standard test GPs use to screen for diabetes. HbA1c is a test that measures your average blood sugar level (glucose) over the past two to three months. A recent study of 374,021 older men with diabetes found that keeping the level of HbA1c stable at an optimal level over a period of three years cut risk of dementia by a third. Similar benefits have been found with patients with pre-diabetes (Prediabetes means that your blood sugars are higher than usual, but not high enough for you to be diagnosed with type 2 diabetes. It also means that you are at high risk of developing type 2 diabetes.) But far lower levels of HbA1c than those used to diagnose diabetes are associated with the first signs of brain shrinkage, which is the hallmark of cognitive decline, even in teenagers.
That is why we offer, as part of our ‘citizen science’ research, an at home pin-prick test of HbA1c, to find out not only who is at risk, but also how to reverse that risk. It also works alongside the free Cognitive Function Test that calculates your future Dementia Risk Index and suggests various lifestyle and nutrition changes to help reduce it, including a low fructose diet (Find out more about low fructose foods here).
We also recommend increasing omega-3 intake from oily fish, increasing B vitamins, especially B12, as well as an active lifestyle, as part of COGNITION, our personalised 6-month programme. In this programme we also dive deeper into lowering your ‘glycaemic load’ (GL), which is low in fructose, alongside periods of time of eating in a ‘ketogenic’ way by keeping sugar and carbohydrates to a minimum. The body responds by creating ketones, energy packets that can replace glucose as an energy source for the brain, helping to undo the damage.
(You get access to COGNITION when you become a FRIEND of Food for the Brain here)
‘Burning ketones can also increase the number and output of the cell’s energy factories, known as mitochondria, which are damaged by fructose,’ says Professor Robert Lustig of the University of California, author of the best-selling book Metabolical and who sits on our Scientific Advisory Board. You can read more in his detailed article here.
Both Professor Johnson and Professor Lustig are also part of the Alzheimer’s Prevention Expert Group who have written to UK dementia prevention authorities to add sugar, and specifically a high fructose diet, to the list of known risk factors.
—
The connection to Ozempic…
This low fructose approach also naturally promotes the enzyme GLP-1, targeted by the weight loss drugs Ozempic and Wegovy, but without the side-effects or rebound weight gain.
Our founder Patrick Holford says: “Today’s typical diet of burgers, carbonated drinks, fruit juice, ice cream, bread, biscuits, cakes and confectionery, plus alcohol and salt, is a dementia time-bomb. Our brains are literally being ‘fructed’. We see the same shrinkage in the same regions of the brain in teenagers with a high sugar intake that are seen in older Alzheimer’s patients. We think of the resulting dementia as type-3 diabetes.”
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.
References:
Johnson RJ et al. The fructose survival hypothesis for obesity. Philos Trans R Soc Lond B Biol Sci. 2023 Sep 11;378(1885):20220230. doi: 10.1098/rstb.2022.0230
Underwood PC et al HbA1cTime in Range and Dementia JAMA Netw Open. 2024 Aug 1;7(8):e2425354. doi: 10.1001/jamanetworkopen.2024.25354
Yau PL et al Obesity and metabolic syndrome and structural brain impairments in adolescence. Pediatrics. 2012 Oct;130(4):e856-64. doi: 10.1542/peds.2012-0324
For those who felt they missed out on the uplifting and enlightening Upgrade Your Brain seminars, Patrick is coming to Wrexham, Leeds, the Yorkshire Dales and Glasgow at the end of October, giving 2 hour Upgrade Your Brain blockbuster seminars and an exclusive one day Upgrade Your Brain retreat in the Burgoyne Hotel in the beautiful Yorkshire Dales. See details and book your place here.
Translations are in full swing and Patrick is going to China and Japan to launch the project at the end of November. We are immensely grateful to Mr Ai of Sharejoy in China where Patrick has been training the staff who will help spread the word, and Dr Atsuo Yanagisawa, President of the Japanese Orthomolecular Society, for their generous support.
—
—
Meanwhile, thanks to our growing army of Ambassadors, we have launched COGNITION in Australia and New Zealand – thank you Linda, Drs Ron Erlich and Ian Brighthope for your support.
Although the blood tests are not yet available there, Alice Coulson is spreading the word in Kenya as our East African Ambassador. Asante Sana!
—
Alice Coulson and Patrick in Kenya Ron Erlich and Linda Conder
—
Not only will we be able to reach and help millions of people to dementia-proof their diet and lifestyle, it also means that our research database will become the biggest and most comprehensive in the world. This means that researchers will want to access our data, created by you as Citizen Scientists, to do their research.
This expansion of knowledge is vital to change the whole health paradigm.
To achieve all this, which requires major technical advancements, server power and investment, we are launching COGNITION International Ltd, a company wholly owned by the charity, to maximise the potential. We do need investment and can offer what are called ‘redeemable preference shares’ for ‘impact’ investors who want both a return on their investment and their money actually being used to make a difference. If you might be interested contact Fran on donations@foodforthebrain.org.
But also know that this continued rapid growth of Foodforthebrain.org, the COGNITION project, and the ongoing development of COGNITION for Smart Kids and Teens, would never have happened if you, FRIENDS of the charity, giving £50 a year, hadn’t supported us.
In the past year we have grown to 2,000 FRIENDS. If you have yet to join please support us in this way and help us reach our next goal of 3000! You can also pay £5 a month if that is easier for you.
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices. Please support our research by becoming a Friend of Food for the Brain.