How the Guardian halves impact of prevention – and what steps make the biggest difference.
Friday’s Guardian article on ‘I refuse to get old’ about how readers strive to keep dementia at bay, on the face of it, seems like a good message. Most cases given focussing on people increasing physical and mental activity, as an active lifestyle is certainly a positive step towards prevention. But these two prevention steps reduce risk by less than B vitamins, omega-3 and reducing sugar and carbs.
The first error is the extent to which dementia can be prevented. The article says by 40%, which is based on the inaccurate Lancet Commission’s Livingston report which, despite being sent all the evidence, doesn’t even mention B vitamins and homocysteine, which is the single most important prevention step. There’s also only one mention of omega-3 from a redundant study so this risk factor is also ignored to arrive at the ‘40% preventable’ figure.
80% of dementia cases could be prevented, not 40%
The latest assessment of how much can be prevented, based on UK Biobank data is “47%–73% of dementia cases could be prevented.” This was published last week in Nature and even this is an underestimate because, while including B vitamins, it excludes the impact of omega-3 and seafood. If that modifiable risk factor were included it is likely that around 80% of dementia cases could be prevented. This would mean that the Guardian is halving the impact of prevention.
The next error is no-one quoted in the article mentions diet, let alone B vitamins or omega-3, except for Professor David Smith. He rightly says: ‘The large leap forward in what we know about preventability has informed his own retirement lifestyle: he walks for half an hour a day, spends at least 15 minutes on an exercise bike, drinks alcohol sparingly, and follows a Mediterranean diet.
Having led a clinical trial into the benefits of B vitamins in people with mild cognitive impairment – a memory-loss condition that increases the chance of those who have it developing dementia – Smith takes 500mcg of vitamin B12 daily and fish oil with Omega 3. Nutrition, he believes, is not given enough prominence when we talk about prevention.’
When we calculated the attributable risk for each risk factor for our online Dementia Risk Index questionnaire each domain scores as follows, adding up to 100%:
B Vitamins 18%
Brain Fats 17%
Glycemic Load 15%
Active Body 15%
Active Mind 10%
Sleep & Calm 10%
Antioxidants 10%
Gut Health 5%
So, the biggest impact you can have on your risk is to supplement B vitamins, especially B12, and omega-3 fish oils, as David Smith does. But the Guardian article then downplays the role of supplements with this statement ‘Alzheimer’s Research UK does not recommend any supplements in particular, but says “there is no harm in people taking a supplement to reduce the risk of deficiency”.
B12 Reference Ranges are wrong
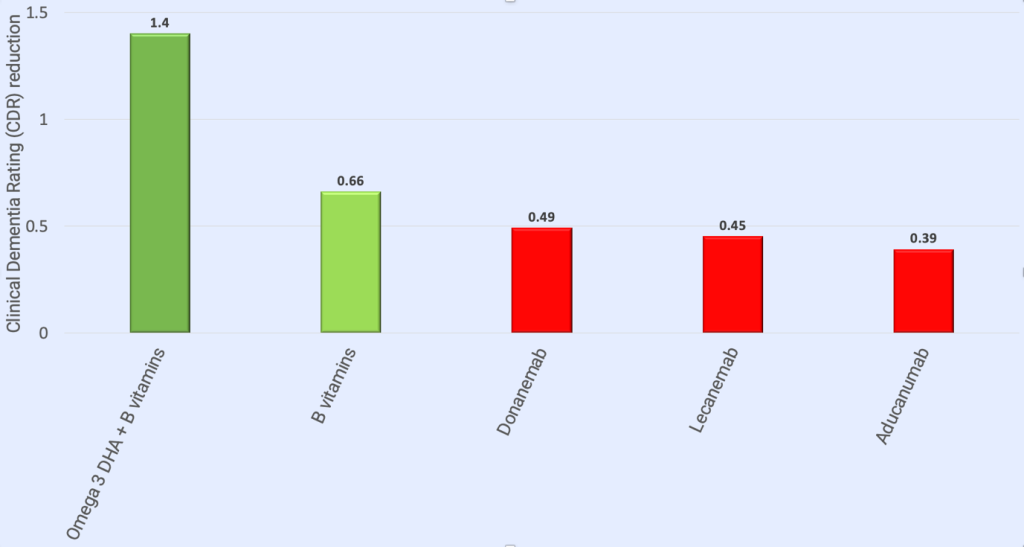
This is not only wrong because brain shrinkage occurs well within the ‘normal’ range of either B12 dietary intake or blood tests, but also ARUK, who largely promotes drug-based solutions, happened to know what they are saying is wrong because they funded, back in 2010, a top level, randomised placebo controlled trial on B vitamins that, virtually stopped cognitive decline and reduced brain shrinkage by 52% – in the group with higher omega 3 , by 73% – that is the most effective disease modifying treatment to date! In fact, David Smith and I have written to ARUK to stop making this inaccurate statement. Here’s why it’s wrong:
The reason so many people are low in B12 is less to do with dietary intake and more due to malabsorption which often becomes worse with age, due to lack of stomach acid secretions which are needed to absorb B12. So relying only of analysing what someone eats (meat, fish, eggs, dairy being the only sources of B12) doesn’t prove sufficiency. Note that David Smith says he supplements 500mcg of B12 daily, while the basic ‘Nutrient Reference Value’ (NRV) that you’ll see on the back of a vitamin supplement is 2.5mcg. So, why does he take two hundred times this amount? Because you cannot rely on your dietary intake to confirm sufficiency. Also, there is growing body of evidence from well designed studies showing that supplements giving nutrients at levels beyond the basic ‘recommended intakes’ delay, eliminate or ameliorate symptoms of dementia.
So, what about blood tests? One UK study reports that 2 in five people over 61 have insufficient levels of B12 to prevent accelerated brain shrinkage. Serum B12 is the ‘standard’ test used by doctors. The UK reference range of above 180pg/ml being sufficient (and the US lower level of 200pg/ml) is out of date and in need of revision. In Europe and Japan anything below 500pg/ml is considered deficient. Accelerated brain shrinkage due to a lack of B12 does happen with B12 levels below 500pg/ml.
In conclusion, while it is good to recommend a physically and intellectually lifestyle, ignoring the need to supplement B vitamins, especially B12, eat fish and supplement omega-3, and cut your intake of carbs and sugar, is not doing anyone any favours.
Food for the Brain is a non-for-profit educational and research charity that offers a free Cognitive Function Test and assesses your Dementia Risk Index to be able to advise you on how to dementia-proof your diet and lifestyle.
By completing the Cognitive Function Test you are joining our grassroots research initiative to find out what really works for preventing cognitive decline. We share our ongoing research results with you to help you make brain-friendly choices.
Please support our research by becoming a Friend of Food for the Brain.